Keywords
Drug Therapy; gemcitabine; Neoplasm Metastasis; Pancreatic Neoplasms
Abbreviations
FOLFIRI: 5-fluorouracil, leucovorin, irinotecan; FOLFIRINOX: 5-fluorouracil, leucovorin, irinotecan, and oxaliplatin
What We Knew Before the 2012 American Society of Clinical Oncology (ASCO) Annual Meeting
Pancreatic cancer is the fourth leading cause of cancer deaths in men and women [1]. The estimated deaths from pancreatic cancer in 2012 in the United States are 37,390, and the five-year survival for all patients with pancreatic adenocarcinoma is less than 5% [2]. Metastatic pancreatic cancer remains a difficult disease to cure. Gemcitabine has been the standard of care for pancreatic cancer for a long time. Even though gemcitabine is tolerated well, its efficacy is marginal with median survival of less than 7 months in metastatic pancreatic cancer patients [3, 4]. Combination chemotherapy with gemcitabine has thus far shown no meaningful survival in metastatic pancreatic cancer [5, 6, 7]. In 2010, Conroy et al. presented the data with combination of 5-fluorouracil, leucovorin, irinotecan, and oxaliplatin (FOLFIRINOX) compared with gemcitabine in metastatic pancreatic cancer patients which showed impressive efficacy, but with major toxicity profile [8]. The median overall survival with this combination was 11.1 months vs. 6.8 nonths in gemcitabine arm. Progression free survival and response rates were significantly improved with FOLFIRINOX (6.4 vs. 3.3 months and 31.6% vs. 9.4%, respectively). Since then, FOLFIRINOX has been the standard of care in good performance metastatic pancreatic cancer patients.
What We Learnt at the 2012 American Society of Clinical Oncology (ASCO) Annual Meeting
This paper summarizes the abstract presentations of metastatic pancreatic cancer at recent ASCO Annual Meeting (Table 1).
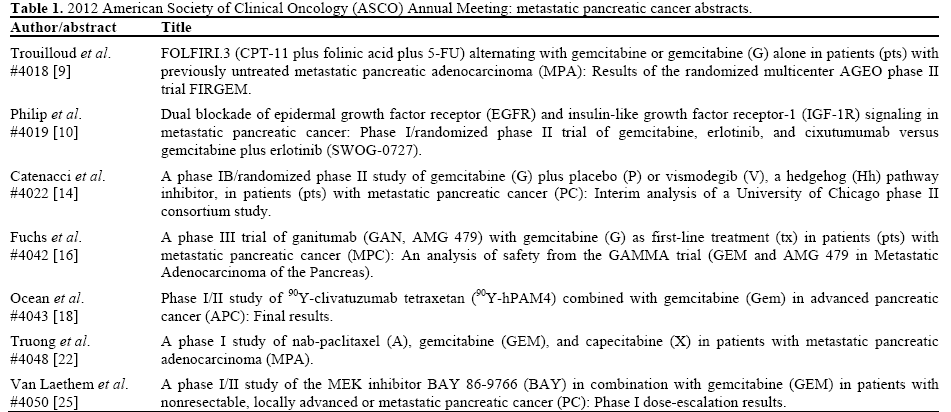
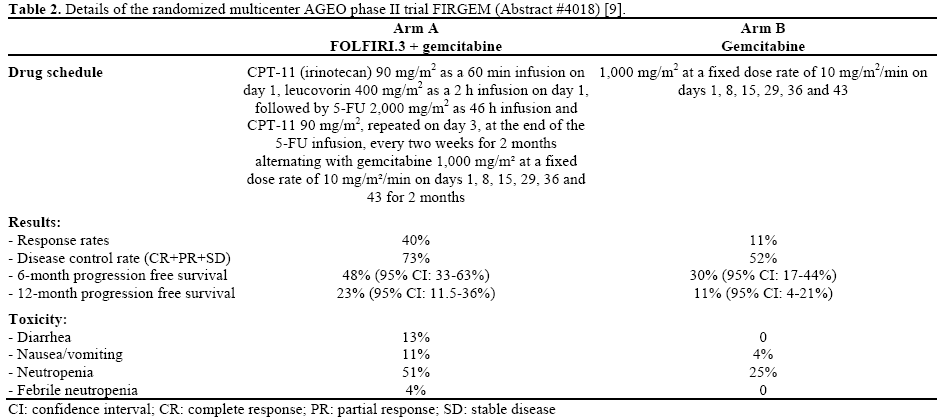
FOLFIRI.3 (CPT-11 plus Folinic Acid plus 5-FU) Alternating with Gemcitabine or Gemcitabine alone in Patients with Previously Untreated Metastatic Pancreatic Adenocarcinoma (MPA): Results of the Randomized Multicenter AGEO Phase II Trial FIRGEM (Abstract #4018) [9]
CPT-11 (irinotecan) has been shown to be efficacious in metastatic pancreatic adenocarcinoma. Conroy, et al. showed dramatic improvement in overall survival with the use of CPT-11 in the FOLFIRINOX regimen; however, there was considerable toxicity [8]. The authors of this abstract present result from the FIRGEM trial that has investigated a new strategy to improve tolerability and efficacy of CPT-11 in metastatic pancreatic adenocarcinoma.
This phase II study enrolled 98 patients in France between 2007 and 2011. Of these 59 patients were males and the median age was 62 years. Performance status was 0-1 and the median follow-up was 23 months. Patients were randomized to 5-fluorouracil, leucovorin (folinic acid), irinotecan (CPT-11) (FOLFIRI.3) for 2 months alternating with gemcitabine for 2 months or gemcitabine alone for two months (detailed in Table 2). The primary end point of the study was progression free survival. Result data are presented below in Table 2. Toxicity profile was much more significant in the experimental arm with more grade 3-4 toxicities as detailed in Table 2. Despite this, the authors concluded that this regimen had a manageable toxicity profile and was more effective in the treatment of metastatic pancreatic adenocarcinoma than gemcitabine alone.
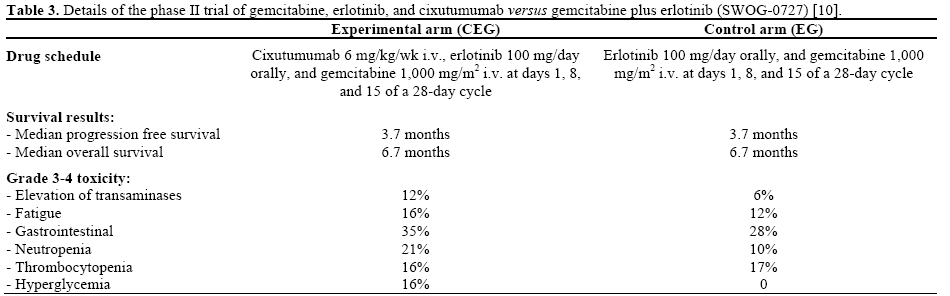
Dual Blockade of Epidermal Growth Factor Receptor (EGFR) and Insulin-Like Growth Factor Receptor-1 (IGF-1R) Signaling in Metastatic Pancreatic Cancer: Phase I/Randomized II Trial of Gemcitabine, Erlotinib, and Cixutumumab versus Gemcitabine plus Erlotinib (SWOG-0727) (Abstract #4019) [10]
This phase I and randomized phase II trial investigated the use of cixutumumab, an anti-IGF-1R monoclonal antibody in combination with erlotinib and gemcitabine. EGFR is over expressed in pancreatic adenocarcinoma and thus a potential therapeutic target [11]. Previous studies have shown marginal improvement of outcomes with erlotinib added to gemcitabine [12, 13]. The hypothesis here is that by targeting both the EGFR and the IGF-1R pathways there would be improvement in survival by manipulating pathways of resistance for each drug.
Ten patients were enrolled in the phase I safety portion and 114 patients with no prior treatment for metastatic pancreatic cancer were eligible in the randomized phase II trial conducted in North America. Drug schedule is shown in Table 3. Cixutumumab 6 mg/kg/wk i.v., erlotinib 100 mg/day orally, and gemcitabine 1,000 mg/m2 i.v. at days 1, 8, and 15 of a 28-day cycle (CEG) was administered in the phase I study and to the experimental arm of the phase II study. Erlotinib 100 mg/day orally, and gemcitabine 1,000 mg/m2 i.v. at days 1, 8, and 15 of a 28-day cycle (EG) was administered to the control arm of the phase II study. The phase I study demonstrated safety of the combination. The primary end point of the phase II study was progression free survival. One-hundred and 24 patients were evaluated with 114 eligible. Fifty-nine percent of patients were female in the experimental arm and 40% in the control arm. The results are shown in Table 3. Toxicities were similar between the two arms with more grade 3-4 toxicities seen in the experimental arm. There were five treatment-related deaths reported (2 cardiac in each arm and 1 pulmonary in the experimental arm). The authors concluded that cixutumumab did not provide improvement in progression free survival or overall survival when combined with erlotinib and gemcitabine.
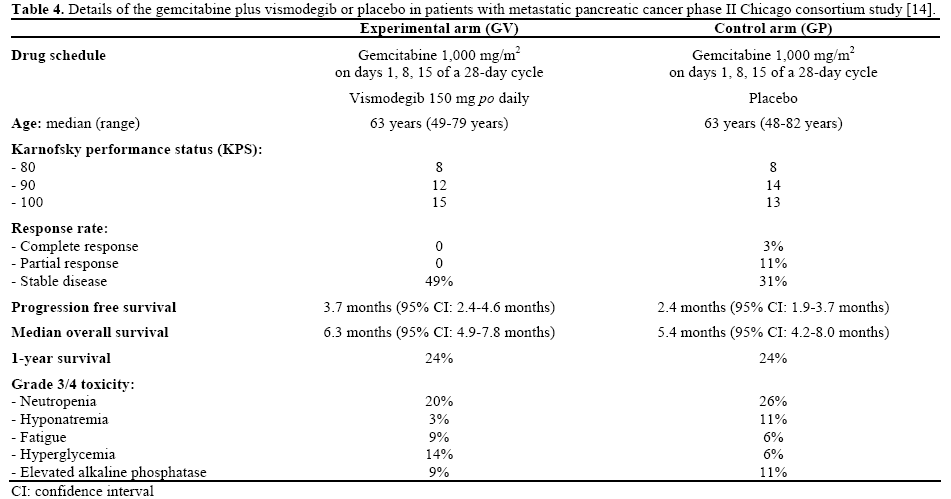
Gemcitabine (G) plus Placebo (P) or Vismodegib (V), a Hedgehog (Hh) Pathway Inhibitor, in Patients (pts) with Metastatic Pancreatic Cancer (PC): Interim Analysis of a University of Chicago Phase II Consortium Study (Abstract #4022) [14]
Activation of sonic hedgehog signaling occurs in the majority of pancreatic cancers [15]. Sonic hedgehog has been shown to act at multiple stages in the development of pancreatic cancer from enhancing proliferation of pancreatic epithelial cells to preventing apoptosis. It has also been shown to coordinate with activated K-ras to promote tumor development; suggesting a novel target for pancreatic cancer treatment.
This study is a multi-center, placebo-controlled, phase IB/randomized phase II trial of gemcitabine with vismodegib or placebo (GV vs. GP) conducted at 12 centers in the United States from February 2010 to June 2011. Patients in this study had a good performance status and were either untreated with metastatic pancreatic cancer or had completed adjuvant therapy more than 6 months prior. Patient characteristics are reviewed in Table 4. Patients were stratified by Karnofsky performance status (KPS: 80 vs. 90 vs. 100) and disease status (newly diagnosed vs. recurrent disease) and randomized to either gemcitabine plus vismodegib or gemcitabine plus placebo (drug schedule shown in Table 4). The primary end-point of the study was progression free survival. Patients in the control (gemcitabine plus placebo) arm who demonstrated progression were allowed to crossover to the experimental arm. This interim analysis was negative (but did not meet criteria for futility) with accrual completed in early 2012 and final report to be made after 90 events. Complete results from the abstract are listed in Table 4. The authors concluded that gemcitabine plus vismodegib has a tolerable toxicity profile and are awaiting the final analysis.
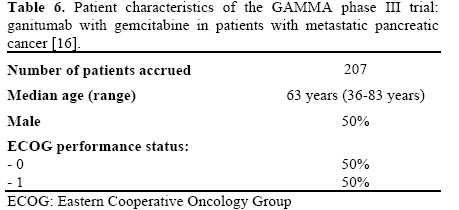
A Phase III trial of Ganitumab (GAN, AMG 479) with Gemcitabine (G) as First-Line Treatment (tx) in Patients (pts) with Metastatic Pancreatic Cancer (MPC): An Analysis of Safety from the GAMMA trial (GEM and AMG 479 in Metastatic Adenocarcinoma of the Pancreas) (Abstract #4042) [16]
For more than a decade gemcitabine has been standard of care for advanced pancreatic cancer [3]. The addition of chemotherapy or targeted therapy to gemcitabine has not yielded any significant benefit [4, 7, 17]. The authors of this abstract presented an ongoing study of ganitumab in a phase III trial of metastatic pancreatic cancer.
This phase II study is taking place globally and is ongoing to evaluate the safety and efficacy of monoclonal antibody inhibitor of IGF-1R, ganitumab as first line treatment in metastatic pancreatic cancer. The estimated sample size is 825 and 207 patients were presented in this abstract. Of those, 204 patients received the study drug. Primary endpoint of the study is overall survival and secondary endpoints are progression free survival, safety and patient-reported outcomes. Drug schedule is presented in Table 5 and patient characteristics are presented in Table 6. Grade 3-4 adverse events in all three treatment arms reported include, neutropenia followed by thrombocytopenia, fatigue, hyperglycemia and liver function test abnormalities. Neutropenia has been a predominant side effect of the therapy. Ten patients died during or within 30 days of the termination of treatment.

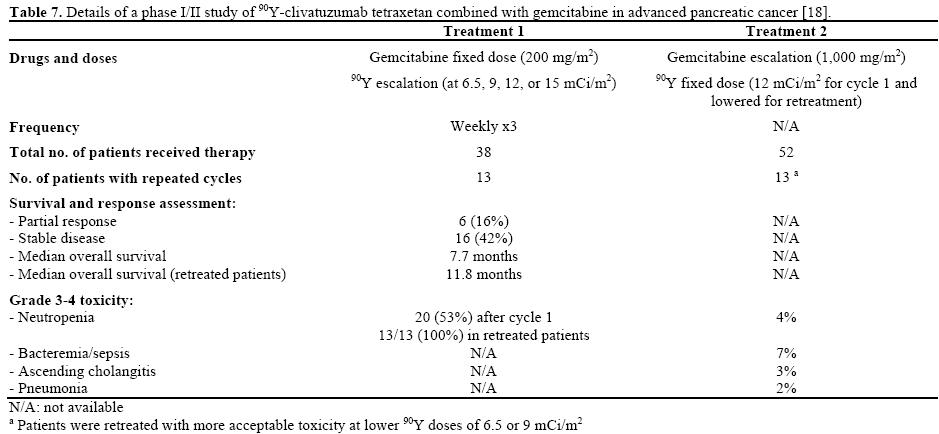
Phase I/II Study of 90Y-Clivatuzumab Tetraxetan (90YhPAM4) Combined with Gemcitabine in Advanced Pancreatic Cancer (APC): Final Results (Abstract #4043) [18]
Pancreatic cancer is one of the most difficult cancers to treat to date. In non-Hodgkin’s lymphoma external radiation and 90Y-labeled antibodies showed promising results [19]. In the preclinical studies, combination of 90Y-hPAM4 and gemcitabine showed enhanced tumor activity with myelosuppression being the most common toxicity [20, 21].
This abstract presents the final results of the phase I/II trial of 90Y-labeled humanized monoclonal antibody, 90Y-hPAM4, and gemcitabine with single or repeated cycles of fractionated radioimmunotherapy as a first line treatment in stage III or IV pancreatic cancer. Treatment was continued until progression, intolerable toxicity or study withdrawal. Table 7 details the therapy schedule and describes the results reported. Improvement in the performance status and pain control was also reported. The toxicities of the regimen are also reported in Table 7. Along with the adverse events reported in the table, infections requiring treatment and one case of bleeding were seen. Low dose gemcitabine 200 mg/m2 was tolerated in combination with fractionated immunoradiotherapy (90Y-hPAM4) as first line treatment for stage 3-4 pancreatic cancer. Main dose limiting toxicity was hematological toxicity.
A Phase I Study of Nab-Paclitaxel, Gemcitabine, And Capecitabine in Patients with Metastatic Pancreatic Adenocarcinoma (Abstract #4048) [22]
Metastatic pancreatic cancer remains a lethal disease with no improvements in combination regimens. A phase III trial of gemcitabine in combination with capecitabine compared to gemcitabine alone showed increased response rate (P=0.034) and progression free survival (P=0.04), but no improvement in overall survival [23]. Hermann et al. in a phase III trial showed that gemcitabine and capecitabine did not improve the overall survival, but subgroup analysis showed combination of gemcitabine and capecitabine improved overall survival compared to single-agent gemcitabine [7]. Meta-analysis of 35 trials of gemcitabine combination regimens showed gemcitabine with capecitabine or oxaliplatin improved overall survival and objective response rate [24]. Here, we discuss the abstract presentation results of a phase I study of gemcitabine, capecitabine and nab-paclitaxel in firstline treatment of metastatic pancreatic cancer.
Patients with Eastern Cooperative Oncology Group (ECOG) performance status of 0-1 were eligible for participation. Treatment included nab-paclitaxel, gemcitabine and capecitabine. Primary goal was to establish the maximum tolerated dose of the regimen and secondary goal is to assess the safety and efficacy of this regimen. Median age range for the enrolled 15 patients was 45-74 years. Initial dose level for this course of therapy was nab-paclitaxel 100 mg/m2, gemcitabine 750 mg/m2, and capecitabine 750 mg/m2 bid and this was established as final maximum tolerated dose. Median number of cycles received was 4 (range: 2-16). Grade 3-4 toxicities were noted in 67% of the patients (10 out of 15 patients) with this combination regimen and included nausea, vomiting, fatigue and liver function test abnormalities. Other side-effects of all grades included fatigue in 87% of the patients, rash or hand foot syndrome in 67%, nausea and vomiting in 53%, diarrhea in 40% and neuropathy in 33% of the patients. Seventy-tree percent of patients had progression of disease and discontinued the treatment. Of the 14 evaluable patients, response rates with this combination were 2 partial responses, 8 stable responses and 4 progressions of disease with a disease control rate of 71%. Out of 12 patients who had elevated CA 19-9 level prior to therapy, 42% (4 patients) of the patients had more than 50% drop in CA 19-9. Authors concluded that the modest response rate could be from the lower dosing of the regimen and the results did not correlate with the phase I/II trial of gemcitabine 1,000 mg/m2 and nab-paclitaxel 125 mg/m2 possibly from the small sample size and the limitations of comparing two different studies.
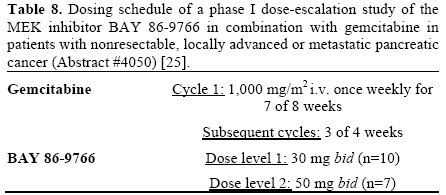
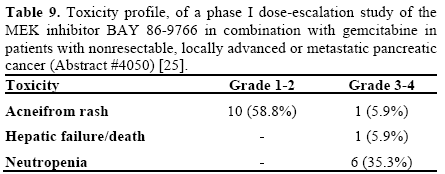
A Phase I/II Study of the MEK Inhibitor BAY 86-9766 (BAY) in Combination with Gemcitabine in Patients with Nonresectable, Locally Advanced or Metastatic Pancreatic Cancer: Phase I Dose-Escalation Results (Abstract #4050) [25]
K-ras mutations are found in approximately 90% of pancreatic cancers [26] and are present exclusively in the cancer cells. Cetuximab failed to show survival advantage in pancreatic cancer harboring K-ras mutation even with predominant K-ras mutation presence in pancreatic cancer [13]. Thus, targeting the RAS-RAF-MEK-ERK pathways may prove to be beneficial in the treatment of K-ras mutant pancreatic cancer.
This abstract presents the results of a phase I/II dose escalation study of the MEK inhibitor BAY 86-9766 and gemcitabine in pancreatic cancer patients. A 3+3 design was used for dose escalation. After dose level 2 of BAY 86-9766, no dose escalation was done. Table 8 shows the treatment details. Maximum tolerated dose was defined as the highest dose at which maximum 1 out of 6 patients had dose limiting toxicity during cycle 1. Seventeen patients were reported to receive treatment of which 10 were at dose level 1 and 7 were at dose level 2. Partial response was seen in 4 out of 10 patients at dose level 1 and one of 3 patients at dose level 2. There was no interaction noted between gemcitabine and BAY 86-9766 at dose level 1. Table 9 shows the toxicity profile of this regimen. The most common side effect of BAY 86-9766 was acneiform rash. The conclusion of this abstract was that BAY 86- 9766 and gemcitabine combination was tolerated well.
Discussion
Gemcitabine remains the standard of care in poor performance patients with metastatic pancreatic cancer patients. Trials with gemcitabine combinations, while well-tolerated, have provided little in the way of survival benefits. A number of abstracts were presented at ASCO examining new combinations. Combinations include traditional chemotherapeutic agents as well as targeted therapies. Preliminary data have not been promising in the realm of targeted agents with the hedgehog pathway inhibitor, MEK inhibitor as well as the EGFR and IGF-1R inhibitors with negative or equivocal preliminary results. Full assessment of these agents cannot be made until the final results are available; however, further investigation into combination agents should continue. Combinations with more traditional chemotherapeutic agents have been more promising but with increased toxicity as shown in the recent FOLFIRINOX study [8].
FOLFIRINOX has emerged as a standard regimen in good performance metastatic pancreatic cancer patients. The toxicity profile tampered the enthusiasm to use this regimen in the oncology world. An abstract presented at the 2012 ASCO Gastrointestinal Cancers Symposium showed that dose attenuations of FOLFIRINOX maintained its efficacy with improvement in the toxicity profile in advanced pancreatic cancer patients [27]. This should prompt further evaluation of FOLFIRINOX as the backbone for the future trials in advanced pancreatic cancer patients. The FIRGEM trial (Abstract #4018) [9] also shows that a more aggressive chemotherapy regimen, like FOLFIRI.3 could be alternated with gemcitabine to improve outcomes and augment toxicities. More information is needed from these and other ongoing clinical trials as the standard of care in metastatic pancreatic cancer continues to evolve.
Authors’ disclosures of potential conflicts of interest
Muhammad Wasif Saif: research funding (Infinity and Clovis); Krishna S Gunturu: None; Jamie Jarboe: None
References
- Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin 2010;60:277-300.
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin 2012;62:10-29.
- Burris HA, 3rd, Moore MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997;15:2403-2413.
- Rocha Lima CM, Green MR, Rotche R, et al. Irinotecan plus gemcitabine results in no survival advantage compared with gemcitabine monotherapy in patients with locally advanced or metastatic pancreatic cancer despite increased tumor response rate. J Clin Oncol 2004;22:3776-3783.
- Heinemann V, Boeck S, Hinke A, et al. Meta-analysis of randomized trials: evaluation of benefit from gemcitabine-based combination chemotherapy applied in advanced pancreatic cancer. BMC Cancer 2008;8:82.
- Heinemann V, Quietzsch D, Gieseler F, et al. Randomized phase III trial of gemcitabine plus cisplatin compared with gemcitabine alone in advanced pancreatic cancer. J Clin Oncol 2006;24:3946- 3952.
- Herrmann R, Bodoky G, Ruhstaller T, et al. Gemcitabine plus capecitabine compared with gemcitabine alone in advanced pancreatic cancer: a randomized, multicenter, phase III trial of the Swiss Group for Clinical Cancer Research and the Central European Cooperative Oncology Group. J Clin Oncol 2007;25:2212-2217.
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011;364:1817-1825.
- Trouilloud I, Dupont-Gossard AC, Artru P, Lecomte T, Gauthier M, ThomasAparicio T, et al. FOLFIRI.3 (CPT-11 plus folinic acid plus 5-FU) alternating with gemcitabine or gemcitabine (G) alone in patients (pts) with previously untreated metastatic pancreatic adenocarcinoma (MPA): Results of the randomized multicenter AGEO phase II trial FIRGEM. J Clin Oncol 2012; 30(Suppl):Abstract 4018.
- Philip PA, Goldman BH, Ramanathan RK, Lenz HJ, Lowy AM, Whitehead RP, et al. Dual blockade of epidermal growth factor receptor (EGFR) and insulin-like growth factor receptor-1 (IGF-1R) signaling in metastatic pancreatic cancer: Phase I/randomized phase II trial of gemcitabine, erlotinib, and cixutumumab versus gemcitabine plus erlotinib (SWOG-0727). J Clin Oncol 2012; 30(Suppl):Abstract 4019.
- Fjallskog ML, Lejonklou MH, Oberg KE, et al. Expression of molecular targets for tyrosine kinase receptor antagonists in malignant endocrine pancreatic tumors. Clin Cancer Res 2003;9:1469-1473.
- Moore MJ, Goldstein D, Hamm J, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007;25:1960-1966.
- Kullmann F, Hartmann A, Stohr R, et al. KRAS mutation in metastatic pancreatic ductal adenocarcinoma: results of a multicenter phase II study evaluating efficacy of cetuximab plus gemcitabine/oxaliplatin (GEMOXCET) in first-line therapy. Oncology 2011;81:3-8.
- Catenacci DVT, Bahary N, Edelman MJ, Nattam SR, de Wilton Marsh R, Kaubisch A, et al. A phase IB/randomized phase II study of gemcitabine (G) plus placebo (P) or vismodegib (V), a hedgehog (Hh) pathway inhibitor, in patients (pts) with metastatic pancreatic cancer (PC): Interim analysis of a University of Chicago phase II consortium study. J Clin Oncol 2012; 30(Suppl):Abstract 4022.
- Ogden SK, Ascano M, Jr., Stegman MA, et al. Regulation of Hedgehog signaling: a complex story. Biochem Pharmacol 2004;67:805-814.
- Fuchs CS, Ikeda M, Bodoky G, Okusaka T, Ohkawa S, Mizuno N, et al. A phase III trial of ganitumab (GAN, AMG 479) with gemcitabine (G) as first-line treatment (tx) in patients (pts) with metastatic pancreatic cancer (MPC): An analysis of safety from the GAMMA trial (GEM and AMG 479 in Metastatic Adenocarcinoma of the Pancreas). J Clin Oncol 2012; 30(Suppl):Abstract 4042.
- Poplin E, Feng Y, Berlin J, et al. Phase III, randomized study of gemcitabine and oxaliplatin versus gemcitabine (fixed-dose rate infusion) compared with gemcitabine (30-minute infusion) in patients with pancreatic carcinoma E6201: a trial of the Eastern Cooperative Oncology Group. J Clin Oncol 2009;27:3778-3785.
- Ocean AJ, Guarino MJ, Pennington KL, Springett GM, Gulec SA, Bekaii-Saab TS, et al. Phase I/II study of 90Y-clivatuzumab tetraxetan (90Y-hPAM4) combined with gemcitabine (Gem) in 30(Suppl):Abstract 4043.
- Morschhauser F, Kraeber-Bodere F, Wegener WA, et al. High rates of durable responses with anti-CD22 fractionated radioimmunotherapy: results of a multicenter, phase I/II study in non-Hodgkin's lymphoma. J Clin Oncol 2010;28:3709-3716.
- Cardillo TM, Blumenthal R, Ying Z, et al. Combined gemcitabine and radioimmunotherapy for the treatment of pancreatic cancer. Int J Cancer 2002;97:386-392.
- Gold DV, Schutsky K, Modrak D, et al. Low-dose radioimmunotherapy ((90)Y-PAM4) combined with gemcitabine for the treatment of experimental pancreatic cancer. Clin Cancer Res 2003;9:3929S-3937S.
- Truong TG, Tempero MA, Kantoff E, Jones K, Dito E, Ong A, Ko AH. A phase I study of nab-paclitaxel (A), gemcitabine (GEM), and capecitabine (X) in patients with metastatic pancreatic adenocarcinoma (MPA). J Clin Oncol 2012; 30(Suppl):Abstract 4048.
- Cunningham D, Chau I, Stocken DD, et al. Phase III randomized comparison of gemcitabine versus gemcitabine plus capecitabine in patients with advanced pancreatic cancer. Clin Oncol 2009;27:5513- 5518.
- Hu J, Zhao G, Wang HX, et al. A meta-analysis of gemcitabine containing chemotherapy for locally advanced and metastatic pancreatic adenocarcinoma. J Hematol Oncol 2011;4:11.
- Van Laethem JL, Heinemann V, Martens UM, Jassem J, Michl P, Peeters M, Weekes CD, Marechal R, Stieler J, Giurescu M, Rajagopalan P, Garosi VL, et al. A phase I/II study of the MEK inhibitor BAY 86-9766 (BAY) in combination with gemcitabine (GEM) in patients with nonresectable, locally advanced or metastatic pancreatic cancer (PC): Phase I dose-escalation results. J Clin Oncol 2012; 30(Suppl):Abstract 4050.
- Almoguera C, Shibata D, Forrester K, et al. Most human carcinomas of the exocrine pancreas contain mutant c-K-ras genes. Cell 1988;53:549-554.
- Krishna SoujanyaGunturu JRT, Howard S. Hochster, Stacey Stein, Xiaopan Yao, Xiangyu Cong, Jill Lacy et.al. Single-institution experience with FOLFIRINOX in advanced pancreatic cancer (PC). J Clin Oncol 2012;suppl 4; abstr 330.

