Lucia Calculli1, Raffaele Pezzilli2, Riccardo Casadei3, Marta Fiscaletti1, Giampaolo Gavelli1
Departments of 1Radiology, Department of 2Internal Medicine and 3Department of Surgery, Sant’Orsola-Malpighi Hospital. Bologna, Italy
- *Corresponding Author:
- Lucia Calcullis
Department of Radiology
Sant’Orsola-Malpighi Hospital
Via Massarenti, 9
40138 Bologna
Italy
Phone: +39-051.636.3383
Fax: +39-051.349.797
E-mail: calclucy@libero.it
Keywords
Pancreatitis; Pancreatitis, Acute
Necrotizing; Pancreatitis, Alcoholic;
Diagnostic Imaging; Tomography, X-Ray
Computed
Abbreviations
ARDS acute distress
respiratory syndrome; CT: computed
tomography; MDCT: multidetector computed
tomography; THAD: transient hepatic
attenuation difference
In clinical practice, it is important to establish
the severity of acute pancreatitis as soon as
possible. At present, the assessment of the
severity of acute pancreatitis is defined
according to the Atlanta clinical criteria [1].
From the clinical point of view we know that
the severity of acute pancreatitis is related to
the age of patients, the male sex, and the
alcoholic and idiopathic etiology of the illness
[2]. Furthermore, from a microbiological
point of view, the infection of the necrosis
reaches a peak in the third week from the
onset of an acute attack of pancreatitis [3].
Imaging plays an important role in answering
the clinical question: is the pancreatitis mild
or severe? The best way to answer to this
question is to determine the presence of
pulmonary or pleuric alterations at chest Xray,
associated or not with an increase in serum creatinine greater than 2 mg/dL. This
simple severity assessment has already been
demonstrated in clinical practice and a
multicenter Italian study was published in
1999 [4]. The authors demonstrated that in
539 acute pancreatitis patients, 163 of whom
(30.2%) had necrotizing pancreatitis, the
presence of pulmonary or pleural alterations
with or without a creatinine concentration
greater than 2 mg/dL had a sensitivity of 60%
and a specificity of 88% in evaluating the
presence of necrosis, a sensitivity of 73% and
a specificity of 75% in evaluating the
presence of infected necrosis, and a sensitivity
of 90% and a specificity of 76% in evaluating
the mortality rate. However, computed
tomography (CT) and the recently introduced
multidetector CT (MDCT) had an important
role in defining not only the presence of pancreatic alterations but also the presence of
associated extrapancreatic involvement; in
fact, the MDCT permits us to confirm the
clinical diagnosis of acute pancreatitis, to
establish the etiology of the illness, to weigh
the necrosis, and to evaluate the follow-up of
the pancreatic and extra-pancreatic
complications. Even if the MDCT is a more
sensitive technique than a traditional spiral
CT, the timing of the appearance of necrosis
using this technique was not changed; in fact,
the presence of necrosis is well-visualized after 48-72 hours from the onset of acute
pancreatitis. The MDCT has changed the
traditional Balthazar score [5] in assessing the
severity of acute pancreatitis. With this
technique, which is faster than the traditional
spiral CT, we can obtain more information
about the involvement of peri- and extrapancreatic
organ involvement; more
information may be obtained regarding
involvement of the portal vein, the mesenteric
superior vein, the mesenteric superior artery and celiac trunk. Furthermore, we can also
obtain information about pleural and
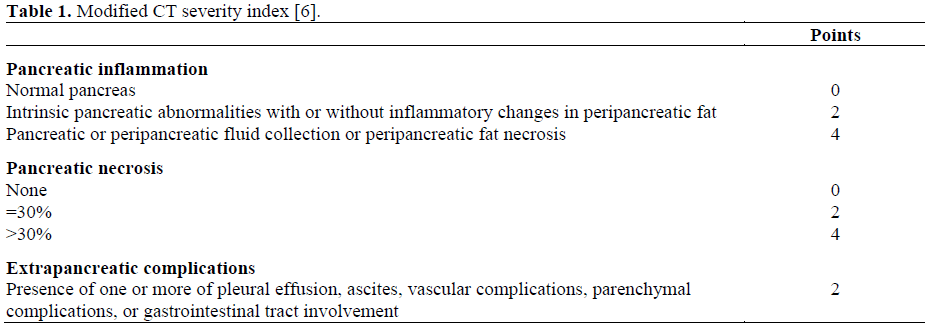
pulmonary alterations. Thus, a new CT
severity index has been proposed by Mortele
et al. [6]. These authors have reported that the
MDCT severity index (Table 1) was highly
related to hospital stay, surgery or
interventional radiological-related procedures
and the presence of infection (Table 2).

What does MDCT add to what is already
known about the imaging of acute
pancreatitis? The first important point is that
MDCT is able to exactly define the pancreatic
involvement: the edema (Figure 1), stranding
(Figure 2), fluid collections (Figure 3),
necrosis of the gland (Figure 4), and
peripancreatic fat (Figure 5) is easily
recognized with this technique. MDCT is also
able to reveal the presence of infection of the
necrosis with high resolution (Figure 6), the
development of pseudocysts (Figure 7), and
the possible link between the pseudocysts and
the pancreatic ducts (Figure 8).
Figure 1. Multidetector computed tomography scan:
edema of the pancreas.
Figure 2. Multidetector computed tomography scan:
stranding during an acute pancreatic inflammation.
Figure 3. Multidetector computed tomography scan:
fluid collections.
Figure 4. Multidetector computed tomography scan:
pancreatic necrosis.
Figure 5. Multidetector computed tomography scan:
peripancreatic fat necrosis.
Figure 6. Multidetector computed tomography scan:
pancreatic infected necrosis.
Figure 7. Multidetector computed tomography scan:
pancreatic pseudocyst.
Figure 8. Multidetector computed tomography scan:
link between pancreatic pseudocyst and the Wirsung
duct.
However, as reported above, the advantage of
this new technique is the diagnosis of extrapancreatic
alterations. MDCT is highly
sensitive in evaluating the presence of pleural
and pulmonary lesions as pleural effusions
(Figure 9), pulmonary infiltrates and acute
distress respiratory syndrome (ARDS; Figure
10). Using “ad hoc” software, MDCT is also able to demonstrate the multiplanar
reconstruction for the study of the vascular
system and the pancreatic ducts to evaluate
the presence of spleen involvement (Figure
11), the transient hepatic attenuation
difference (THAD) (Figure 12), the presence of pseudoaneurisms (Figure 13) or thrombosis
of the splenic vein (Figure 14).
Figure 9. Multidetector computed tomography scan:
pleural effusion.
Figure 10. Multidetector computed tomography scan:
pulmonary infiltrates (a.) and acute respiratory distress
syndrome (b.).
Figure 11. Multidetector computed tomography scan:
spleen involvement.
Figure 12. Multidetector computed tomography scan:
transient hepatic attenuation difference.
Figure 13. Multidetector computed tomography scan:
pseudoaneurism.
Figure 14. Multidetector computed tomography scan:
thrombosis of the splenic vein.
MDCT recognizes small lesions such as the
presence of small pancreatic cancers which
may be associated with a mild acute
pancreatitis in about 6% of the cases [7]
(Figure 15).
Figure 15. Multidetector computed tomography scan:
small pancreatic cancer in a patient with mild acute
pancreatitis.
This technique is of assistance to clinicians
with interventional radiological procedures
such as the sampling of the necrosis for
microbiological assessment (Figure 16), and
the percutaneous treatment of fluid collections
and pseudocysts in high risk patients.
Figure 16. Multidetector computed tomography scan:
Interventional procedure in a patient with necrotizing
pancreatitis.
References
- Bradley EL 3rd. A clinically based classification
system for acute pancreatitis. Summary of the
International Symposium on Acute Pancreatitis,
Atlanta, Ga, September 11 through 13, 1992. Arch
Surg 1993; 128:586-90. [PMID 8489394]
- Talamini G, Uomo G, Pezzilli R, Rabitti PG, Billi
P, Bassi C, Cavallini G, Pederzoli P. Serum creatinine
and chest radiographs in the early assessment of acute
pancreatitis. Am J Surg 1999; 177:7-14. [PMID
10037300]
- Beger HG, Bittner R, Block S, Buchler M.
Bacterial contamination of pancreatic necrosis. A
prospective clinical study. Gastroenterology 1986;
91:433-8. [PMID 3522342]
- Pezzilli R, Billi P, Morselli-Labate AM. Severity
of acute pancreatitis: relationship with etiology, sex
and age. Hepatogastroenterology 1998; 45:1859-64.
[PMID 9840164]
- Balthazar EJ, Robinson DL, Megibow AJ, Ranson
JH. Acute pancreatitis: value of CT in establishing
prognosis Radiology 1990; 174:331-6. [PMID
2296641]
- Mortele KJ, Wiesner W, Intriere L, Shankar S,
Zou KH, Kalantari BN, Perez A, vanSonnenberg E,
Ros PR, Banks PA, Silverman SG. A modified CT
severity index for evaluating acute pancreatitis:
improved correlation with patient outcome. AJR Am J
Roentgenol 2004; 183:1261-5. [PMID 15505289]
- Imamura M, Asahi S, Yamauchi H, Tadokoro K,
Suzuki H. Minute pancreatic carcinoma with initial
symptom of acute pancreatitis. J Hepatobiliary
Pancreat Surg 2002; 9:632-6. [PMID 12541052]

















