Keywords
Pneumococcal infection; Conjugate vaccine; PCV7; Immunogenicity; Specific pneumococcal serotype; Highrisk disease; Opsonophagocytic assay; Geometric mean titre
Introduction
Pneumococcal disease is a leading cause of childhood morbidity and mortality worldwide [1]. In 2005, the World Health Organization estimated that 1.6 million people die from pneumococcal diseases annually, 0.7-1.0% of whom are children under the age of 5 years [2]. The causative agent of pneumococcal disease, Streptococcus pneumoniae (Pneumococcus), is a Gram-positive bacterium that causes pneumonia, meningitis, and acute otitis media [3]. Invasive pneumococcal disease (IPD) is defined as the isolation of S. pneumoniae from a normally sterile site (blood, cerebral spinal fluid, joint fluid, and pleural or pericardial fluid) [4]. IPD predominately occurs among children aged <5 years and adults aged ≥65 years [5]. Non-invasive pneumococcal disease may progress to IPD, such as when an ear infection leads to sepsis [6]. Preventing pneumococcal disease is an important international public health priority because of its high associated morbidity and mortality, especially among children in developing countries [7].
S. pneumoniae can be differentiated by its capsular polysaccharide (PS) into serotypes [8]. Antibodies to S. pneumoniae capsular PS antigens provide serotype-specific protection against pneumococcal infections [2]. Two different pneumococcal vaccine types are currently available on the market: pneumococcal conjugate vaccines (PCVs) routinely used in children and the pneumococcal polysaccharide vaccine (PPV) used in adults [9]. Currently, a heptavalent PCV (PCV7) and an unconjugated PPV covering 23 serotypes (PPV23) are marketed internationally. PPV23 has been available since the early 1980s, whereas PCV7 has been available since 2009 [10].
In the U.S., the Advisory Committee on Immunization Practices for the Centers for Disease Control and Prevention [11] and the American Academy of Pediatrics [12] have recommended routine administration of PCV7. PCV7 has been shown to induce immunity against the seven most common serotypes causing IPD in children (4, 6B, 9V, 14, 18C, 19F, and 23F), as detected by opsonophagocytic activity [13]. PCV7 was licensed in 2000 and is recommended for use by the Advisory Committee on Immunization Practices [14] to be given to all children in the U.S. aged 2-23 months and children aged 24-59 months at increased risk for morbidity and mortality due to pneumococcal infection. Unlike PPV23, PCV7 elicits a T-celldependent response, protecting young children against pneumococcal disease [15]. The use of PCV7 has dramatically reduced the rates of IPD, otitis media, and nasal carriage of vaccine serotypes among all vaccinated age groups, including immuno-compromised and older individuals [16]. In 2010, the U.S. Food and Drug Administration licensed a 13-valent PCV (PCV13) [17]. PCV13 has been recommended by the Advisory Committee on Immunization Practices to replace PCV7 [18]. PCV13 stimulates immunity against the same seven serotypes as PCV7 and six additional serotypes known to cause IPD in the U.S. (1, 3, 5, 6A, 7F, and 19A) [19].
PCV7 is approved for use in all children aged ≤ 2 years and children aged 2-5 years at increased risk for developing IPD [12]. PCV7 not only protects immunised children from pneumococcal disease but also provides protection via herd immunity [14]. The immunogenicity of a pneumococcal vaccine is typically determined using an enzyme-linked immunosorbent assay (ELISA) to evaluate serotype-specific antibody concentrations. However conventional antibody detection of pneumococcal PS antigens is not specific because the purified PS used for ELISA is contaminated with cell wall PSs [20]. The PS ELISA has been made more specific by neutralizing interfering cell wall PS antibodies [21-23] and irrelevant capsular PS (e.g. serotype 22F PS) [24]. However, ELISA is not very specific because it does not correlate well with the function of protective antibodies [25] and cannot differentiate between non-protective low-avidity antibodies and protective high-avidity antibodies [26]. A better test to determine protective antibody responses is to measure the ability of granulocytes to opsonise pneumococci, which correlates well with vaccine-induced immunoprotection [27]. Such an assay has been developed, which is called the opsonophagocytic assay (OPA). The best OPA is the opsonophagocytic killing assay (OPKA), which measures the reduction in the number of viable bacteria due to phagocytes, antibodies, and complement [27]. Song et al. [28] studied pneumococcal vaccine efficacy using the OPKA and reported this assay is an ideal marker of pneumococcal vaccine efficacy. Recent technical developments have allowed OPKAs to be used for many vaccine studies [29,30]. The results appear to correlate well with disease protection, particularly when evaluating crossprotection.
In the present study, young Thai children with risk factors for IPD including congenital heart disease, chronic lung disease, haematological defects, prematurity, and HIV infection were immunised with PCV7 at different dosages according to agebased immunisation schedules. This immunisation project was conducted in 2010, when no other advanced vaccine was imported to Thailand. The retrospective work was thus investigated on these frozen-stock sera. We used the OPKA to determine bactericidal antibody titres against the seven PCV7 vaccine serotypes and relevant serotype 19A in pre- and postvaccination sera. If effective, PCVs could be used to prevent pneumococcal disease among Thai children at high risk for IPD, who suffer from underlying diseases and are likely to have less efficient immune responses.
Subjects and Methods
Subjects
A total of 129 Thai children (72 males and 57 females; aged 2 months to 8 years) from a general paediatric outpatient department at the Hospital for Tropical Diseases, Mahidol University Bangkok, and two orphanages in Bangkok were enrolled. Children suffering from various illnesses were included in the immunisation scheme. Study subjects were children classified as high risk for IPD. All children were divided into the following groups based on their illnesses:
1. Children born prematurely (gestational age <37 weeks) or born small for gestational age (birth weight <2,500 g) were included in the premature (PMT) group.
2. Children with chronic heart diseases including congenital or acquired heart disease, e.g. rheumatic heart disease diagnosed by a certified paediatric cardiologist, were included in the chronic heart disease (CHD) group.
3. Children with chronic lung diseases or asthma were included in the chronic lung disease (CLD) group; children with CLD had radiographic changes consistent with bronchopulmonary disease and use of supplemental oxygen at 36 weeks of postconceptional age, whilst asthmatic patients had episodic symptoms of airflow obstruction that could be at least partially reversible.
4. Children with haemoglobinopathies including thalassemia disease confirmed by haemoglobin typing were included in the haematological disease (HMT) group.
5. Children with HIV infection were included in the HIV group.
Exclusion criteria included a history of allergy to PCV7 or its components and patients who received a blood transfusion or immunoglobulin in the 3-month period prior to the study.
Serum samples
Serum samples were obtained from each study subject prior to initial vaccination and 4 weeks after completing PCV7 vaccination. All sera were stored at −20°C until analysis.
Vaccine dosages and time schedules
PCV7 (Prevnar®, Wyeth Pharmaceuticals, Philadelphia, PA, USA) was given to all study subjects. The PCV7 vaccine regimen followed the recommendations of the American Academy of Pediatrics Red Book [31]. For children aged ≤ 6 months on initiation of the primary vaccine series, 3 doses of the vaccine were given at least a month apart, followed by a booster dose at age 12-15 months. For children aged 7-11 months on initiation, 2 doses of the vaccine were given at least a month apart, followed by a booster dose at age 12-15 months. For children aged ≥ 12 months on initiation, 2 doses of the vaccine were given at least a month apart.
Ethical considerations
This study was approved by the Ethics Committee of the Faculty of Tropical Medicine, Mahidol University (approval number 2009-048-04). Written informed consent was obtained after giving a full explanation of the study aim and a detailed description of its protocol from the legal guardians of all participating children, including orphans with approval obtained from orphanages.
OPKA
The functional capacities of vaccine-raised antibodies against the seven vaccine serotypes (4, 6B, 9V, 14, 18C, 19F, and 23F) and related serotype 19A were measured in pre- and postvaccinated sera by OPKA as previously described by Kim et al. with some modification. Due to the limited volume of sera available from young children enrolled in this study, a starting serum dilution of 1:4, followed by two-fold dilutions, was used (1:4-1:64). Two-fold serum dilutions were prepared in a 96-well plate (Nunc™ MicroWell™ Thermo Fisher Scientific, Waltham, MA, USA). Ten microlitres containing S. pneumoniae at 1,000 CFU/μl was added to 20 μl of test serum. After incubation at room temperature for 30 min, 40 μl of HL-60 cell suspension (4 × 105 cells/well) and 10 μl of guinea pig complement were added to each well. Opsonisation buffer (Hank’s balanced salt solution containing 0.1% gelatin and 10% fetal calf serum) was added to control wells. The solution was incubated for 1 h at 37°C with shaking. Ten microlitres of reaction mixture were then plated onto Todd-Hewitt agar-yeast extract plates. After the fluid was absorbed into the agar, molten Todd-Hewitt agar (0.75%) containing yeast extract (0.5%) and 100 mg/litre of 2,3,5- triphenyl tetrazolium chloride (TTC; Sigma, Singapore) and selected antibiotics were poured on top of the agar layer. The plates were then incubated in a candle jar at 37°C overnight. The number of bacterial colonies of each serotype surviving on the plates was then counted. The opsonisation titre was defined as the serum dilution resulting in a reduction of half the number of colonies from control wells.
In the multiplexed OPKA assay, the target bacteria were an equal mixture of one streptomycin-resistant and one optochinresistant pneumococcal strain from two different serotypes (e.g. streptomycin-resistant 6B and optochin-resistant 19F) (Table 2). The bacterial pair was put in one assay tube and the reaction mixture was plated onto selective medium containing different antibiotic markers. During the assay, sera that were positive to each bacterial serotype were collected and included as a positive control in each experiment (Table 2). Experiments were repeated if the titre of control sera was not same as the previous result.
Statistical analysis
In the OPKA, the lowest dilution of tested serum in the assay is 1:4 dilutions. The first serum dilution that did not kill 50% of bacteria was reported as ‘1.0’ for analysis purposes; the other two-fold dilutions of 1:4, 1:8, 1:16, 1:32, and 1:64 were reported as 4, 8, 16, 32, and 64, respectively. The log value of two-fold dilution gave a more symmetrical distribution for which an arithmetic mean was appropriated; therefore, results were reported as the log geometric mean (GM) titre. The GM titre (and 95% confidence intervals) of each studied group was compared using the paired sample t-test between pre- and postvaccination sera. Statistical analyses were conducted using SPSS software (version 18). P values <0.05 were considered statistically significant. The one sample T test was also used to compare the mean of your sample data to a known value, in this study the sample mean was compared to the population mean.
Results
A total of 129 children (72 males) were included in the study. Risk factors for IPD among study subjects included haematological disease (n=4), HIV (n=13), premature birth (n=16), congenital heart disease (n=40), and chronic lung or reactive airway disease (n=56).
Positive control sera
Sera with high titres to relevant serotypes (Table 1) were selected for inclusion in each OPKA assay to validate that HL-60 cells, complement, and all reagents were standardised.
| Age (months) |
>12 |
7–12 |
2–6 |
Total Number |
| Number of vaccine doses |
2 |
3 |
4 |
|
| Congenital heart disease group |
28 |
7 |
5 |
40 |
| Prematurity group |
10 |
1 |
5 |
16 |
| Chronic lung disease group |
41 |
7 |
8 |
56 |
| Haematological disease group |
4 |
0 |
0 |
4 |
| HIV group |
12 |
0 |
1 |
13 |
| Total |
95 |
15 |
19 |
129 |
| Sex |
>12 |
7–12 |
2–6 |
Total Number |
| Male |
52 |
9 |
11 |
72 |
| Female |
43 |
6 |
8 |
57 |
| Total |
95 |
15 |
19 |
129 |
Table 1: Distribution of vaccinated children at high risk of pneumococcal infection.
Selected positive control sera to each serotype used in each assay to monitor the reproducibility of the assay are shown in Table 2.
| Streptomycin-resistant serotype |
Optochin-resistant serotype |
No. of sera as positive control |
| 6B |
19F |
111 |
| 9V |
4 |
112 |
| 23F |
18C |
136 (23F), 40 (18C) |
| 14 |
19A |
39 |
Table 2: Paired Streptococcus pneumoniae serotypes and their corresponding antibiotic markers.
Control positive sera that strongly reacted to bacterial pairs are indicated in parentheses.
GM titre of opsonophagocytic activity
Prior to PCV7 vaccination, all children had antibody titres of <1:4. Table 3 shows the GM OPKA titres for each serotype. OPKA titres of pre-vaccination sera were approximately 1, whilst post-vaccination sera titres were significantly increased in all children (p<0.05).
| Disease group |
Chronic heart disease |
Prematurity |
Chronic lung disease |
Haematological disease |
HIV |
| Pneumococcal serotype |
Geometric mean titre |
Fold increase |
Geometric mean titre |
Fold increase |
Geometric mean titre |
Fold increase |
Geometric mean titre |
Fold increase |
Geometric mean titre |
Fold increase |
| pre |
post |
pre |
post |
pre |
post |
pre |
post |
pre |
post |
| 4 |
1.04 |
3.48 |
3.3 |
1.00 |
4.36 |
4.3 |
1.03 |
4.26 |
4.1 |
1.00 |
4.00 |
4 |
1.38 |
3.41 |
2.4 |
| 6B |
1.07 |
13.69 |
12.7 |
1.19 |
9.93 |
8.3 |
1.13 |
12.49 |
10.1 |
1.00 |
5.66 |
5.66 |
1.00 |
4.45 |
4.4 |
| 9V |
1.00 |
1.27 |
1.2 |
1.00 |
1.35 |
1.3 |
1.00 |
1.41 |
1.4 |
1.00 |
1.68 |
1.68 |
1.00 |
1.00 |
1 |
| 14 |
1.32 |
10.93 |
8.2 |
1.00 |
10.83 |
10.8 |
1.25 |
8.72 |
6.9 |
1.00 |
11.31 |
11.31 |
1.53 |
10.44 |
6.8 |
| 18C |
1.00 |
6.5 |
6.5 |
1.00 |
5.91 |
5.9 |
1.00 |
5.00 |
5.0 |
1.00 |
4 |
4 |
1.00 |
3.79 |
3.7 |
| 19A |
1.11 |
6.06 |
5.4 |
1.00 |
4.18 |
4.1 |
1.10 |
32.57 |
2.3 |
1.00 |
9.51 |
9.51 |
1.11 |
3.41 |
3.1 |
| 19F |
1.04 |
6.73 |
6.4 |
1.00 |
4.97 |
4.9 |
1.00 |
12.80 |
12.8 |
1.00 |
6.73 |
6.73 |
1.00 |
5.81 |
5.8 |
| 23F |
1.00 |
2.22 |
2.2 |
1.00 |
2.71 |
2.7 |
1.03 |
2.18 |
2.1 |
1.00 |
2.38 |
2.38 |
1.00 |
2.61 |
2.6 |
Table 3: Geometric mean OPKA titres in pre- and post-vaccination sera in each disease group. The fold increase that was equal of more than 4 was in bold.
A four-fold increase in antibody titre is generally regarded as a good response. Antibody responses of post-vaccination sera to serotypes 9V and 23F increased more than four-fold from prevaccination titres. Antibody titres to serotype 19F (vaccine serotype) ranged from 4.97 to 12.3, whilst those to serotype 19A (its closely related strain) ranged from 2.57 to 9.51. The antigenicity of serotype 19F was thus similar to serotype 19A. However, antibody raised against serotype 19A was decreased in the CLD group (2.3-fold) and HIV group (3.1-fold).
Overall, all disease groups demonstrated good responses to pneumococcal serotypes tested. CHD and CLD groups demonstrated a four-fold increase in antibody titres to five of eight serotypes, whilst PHT and HMT groups showed a four-fold increase in antibody titres to six of eight serotypes. The poorest response was observed in the HIV group, which exhibited good responses to only three of eight serotypes, indicating the immunodeficiency status among this group.
We next compared sera titres to each serotype among disease groups by one sample t-test. As shown in Table 4 and Figure 1, the mean log titres to serotypes 4, 9V, 14, 18C, and 23F of each disease group were not significantly different from mean log titres set as test values.
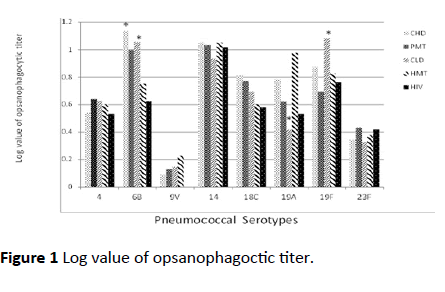
Figure 1: Log value of opsanophagoctic titer.
| Serotype |
N |
4 |
|
6B |
|
9V |
|
14 |
|
| Test value =0.6 |
Test value = 0.9 |
Test value = 0.1 |
Test value = 1 |
| Mean |
Sig.
(two-tailed) |
Mean |
Sig.
(two-tailed) |
Mean |
Sig.
(two-tailed) |
Mean |
Sig.
(two-tailed) |
| CHD |
40 |
0.5418 |
0.368 |
1.1362 |
0.002* |
0.0903 |
0.780 |
1.0535 |
0.495 |
| PMT |
16 |
0.6396 |
0.615 |
0.9970 |
0.298 |
0.1316 |
0.668 |
1.0346 |
0.708 |
| CLD |
56 |
0.6279 |
0.597 |
1.0586 |
0.019* |
0.1453 |
0.189 |
.9341 |
0.250 |
| HMT |
4 |
0.6020 |
0.993 |
0.7525 |
0.644 |
0.2257 |
0.616 |
1.0535 |
0.582 |
| HIV |
13 |
0.5325 |
0.651 |
0.6251 |
0.115 |
0.0000 |
|
1.0187 |
0.854 |
| Mean log titre |
|
0.5887 |
|
0.9139 |
|
0.1186 |
|
1.0189 |
|
| Serotype |
|
18C |
|
19A |
|
19F |
|
23F |
|
| |
Test value = 0.7 |
Test value = 0.6 |
Test value = 0.8 |
Test value = 0.3 |
| N |
Mean |
Sig.
(two-tailed) |
Mean |
Sig. (two-tailed) |
Mean |
Sig. (two-tailed) |
Mean |
Sig. (two-tailed) |
| CHD |
40 |
0.8127 |
0.116 |
0.7826 |
0.053 |
0.8729 |
0.329 |
0.3461 |
0.402 |
| PMT |
16 |
0.7713 |
0.465 |
0.6208 |
0.903 |
0.6960 |
0.498 |
0.4326 |
0.165 |
| CLD |
58 |
0.6954 |
0.924 |
0.4151 |
0.006* |
1.0846 |
0.000* |
0.3269 |
0.578 |
| HMT |
4 |
0.6020 |
0.677 |
0.9782 |
0.339 |
0.8277 |
0.860 |
0.3762 |
0.758 |
| HIV |
13 |
0.5788 |
0.245 |
0.5325 |
0.675 |
0.7640 |
0.772 |
0.4167 |
0.333 |
| Mean log titre |
|
0.6920 |
|
0.6658 |
|
0.8490 |
|
0.3797 |
|
Table 4: Log values of opsonophagocytic titres from post-vaccination sera. The mean titre in each disease group was compared by the one sample t-test. Sig. = Significant Asterisk (*) = the significant value that less than 0.05. The abbreviation for each disease group were; the premature (PMT) group ; the chronic heart disease (CHD) group; the chronic lung disease (CLD) group; the haematological disease (HMT) group and HIV- infected children (HIV).
However, for serotype 6B, antibody titres of CHD and CLD groups were significantly higher than the test values (p=0.002 and p=0.019, respectively) (Table 4), suggesting CHD and CLD groups have better responses to PCV7 than the other disease groups. Moreover, the CLD group demonstrated a significantly lower mean antibody titre to serotype 19A (p=0.006) and higher antibody titre to serotype 19F (p<0.001) than the test values. This finding suggests that antibody to serotype 19F may not be sufficient to provide protection against serotype 19A in CLD patients.
Discussion
In the present study, the immunogenicity of PCV7 was evaluated among Thai children at high risk of developing severe pneumococcal infections, including premature children and children with CLD, CHD, HMT, and HIV.
Vaccine-induced immunity was previously evaluated by measuring serotype-specific antibodies in pre- and postvaccinated sera with PCV7 by ELISA [32]. However, this particular ELISA cannot differentiate non-protective low-avidity antibodies from protective high-avidity antibodies. Protective immunity can be estimated by directly measuring the opsonic capacity of vaccine-induced antibodies because such antibodies can provide protection via phagocytic opsonisation of pneumococci [33]. Since host protection is mediated mainly by opsonin-dependent phagocytosis, an in vitro measurement of the opsonophagocytic activity of anti-capsular antibodies using the OPKA is believed to be a reliable method for evaluating the protective efficacy of vaccination [34]. In vitro OPKA is often used to supplement pneumococcal ELISA, and it should be a good surrogate assay for predicting immuno-protection induced by pneumococcal vaccines [35].
Although only serotype 19F is included in PCV7, we also evaluated serotype 19A in the OPKA to evaluate the presence of cross-reactivity between these closely related serotypes. It was expected that immunological similarities between vaccine serotype 19F and related serotype 19A would elicit crossprotection, as observed for serotype 6B and its related serotype 6A [33,36]. 19F and 19A PSs are composed of similar trisaccharide units polymerised through phosphate diester groups that differ only in the position of the linkage to Lrhamnose residue [α(1 × 2) for 19F and α(1 × 3) for 19A] [37]. The PCV7 vaccination schedule used in the present study elicited antibody responses to both serotypes, confirming the antibody cross-reactivity previously noted between these two strains. However, immune responses to serotype 19F were higher than those to serotype 19A in all vaccinated children, particularly those in the CLD group.
Overall, sera from children in all disease groups showed low antibody responses to serotypes 9V and 23F, suggesting that these two strains are poor immunogens. Moderate responsive antibody titres were observed for serotypes 4, 18C, 19A, and 19F, whilst high antibody titres were observed for serotypes 6B and 14. However, HIV-infected children had deficient immune responses, as they demonstrated responsive antibody to only three of eight serotypes, whilst children in the other disease groups exhibited responsive antibody to five or six serotypes. Moreover, the mean antibody titre to each serotype among the disease groups was not significantly different from the mean log titre set as the test value. All studied groups thus had similar responsiveness to PCV7. Therefore, the main disadvantage of PCV7 among children with chronic disease appeared to be low immunogenicity of serotypes 9V and 23F.
Jauneikaite et al. [38] reported that the serotype distribution of invasive pneumococcal isolates was 19F, 23F, 14, 6B, 1, 19A, and 3 (in rank order), and this distribution was found to be similar across countries in the Association of South East Asian Nations (ASEAN) region (Laos, Malaysia, the Philippines, Singapore, Thailand, and Vietnam). In 2000-2005, the most common S. pneumoniae serotypes isolated from sterile sites in Thai children younger than 5 years in the Medical Institution of Bangkok were serotypes 6B (27.8%), 23F (20.0%), 14 (10.4%), and 19F (9.6%). The results found in the present study revealed low immune response to serotype 23F after PCV7 vaccination, leading to an awareness that PCV7 vaccination may not protect against predominant serotypes causing pneumococcal infections in Thailand. The low- or non-specific antibody responses to serotypes 9V and 23F might be improved by boosting with another vaccine, such as PPV23. PPV23 boosting can increase serum pneumococcal antibody concentrations and functional antibody titres against certain PCV7 and non-PCV7 serotypes as much as or more than boosting with PCV7 [39].
Conclusion
In conclusion, functional immune responses were detected among children with high risk of pneumococcal infection in Thailand following PCV7 vaccination. Importantly, our results also showed some children with haematological diseases and HIV could be responsive to PCV7, similarly to other high-risk groups with chronic disease. However, low- or non-specific antibody responses to serotypes 9V and 23F were noted, thus boosting with another vaccine may be required.
Acknowledgements
This work was supported by a research grant from the Faculty of Tropical Medicine, Mahidol University, Thailand, during 2014-2015. We thank Christina Croney, PhD, from Edanz Group (www.edanzediting.com/ac), and Prof. Dr. Srisin Khusamirh for editing a draft of this manuscript.
Authors’s Contributors
Dr. W. Hattasingh is a paediatric medical doctor who created this research project, organizing the subjects on vaccination, and collecting all sera samples. Mr. W. Tunyong did all laboratory work, collect data and statistical analysis of all results. Dr. Y. Mahakunkijcharoen supported the macrophage cell lines during the assay. Dr. T. Kalambaheti assisted in setting up the opsanophagocytic assay, data analysis and writing the manuscript.
References
- Wong SS, Toh ZQ, Dunne EM, Mulholland EK, Tang MLK, et al. (2013) Inhibition of Streptococcus pneumoniae adherence to human epithelial cells in vitro by the probiotics. Barson WJ, Kaplan SL. (eds), ( GG. BMC Research Notes. 6: 135.
- WHO (2007) Pneumococcal Conjugate Vaccine for Childhood Immunization – WHO position paper. Weekly Epidemiological Record. 82: 93-104.
- Wald ER, Mason EO Jr., Bradley JS, Barson WJ, Kaplan SL (2001) Acute otitis media caused by Streptococcus pneumoniae in children's hospitals between 1994 And 1997. Pediatr Infect Dis J. 20(1): 34-39.
- Tan TQ. (2012) Pediatric invasive pneumococcal disease in the United States in the era of pneumococcal conjugate vaccines. Clin Microbiol Rev. 25(3): 409-419.
- Zhao C, Zhang F, Chu Y, Cao B (2013) Phenotypic and genotypic characteristic of invasive pneumococcal isolates from both children and adult patients from a multicenter surveillance in China 2005-2011. PLOS ONE 8(12): e82361.
- Ludwig E, Bonanni P, Rohde G, Sayiner A, Torres A (2012) The remaining challenges of pneumococcal disease in adults. Eur Respir Rev: An Official Journal of the European Respiratory Society 21(123): 57-65.
- Roca A, Dione MM, Bojang A, Townend J, Egere U, et al. (2013) Nasopharyngeal carriage of pneumococci four years after community-wide vaccination with Pcv-7 in the Gambia: long-term evaluation of a cluster randomized trial. PLOS ONE. 8(9): e72198.
- Pai VB, Heyneman CA, Erramouspe J (2002) Conjugated heptavalent pneumococcal vaccine. The Annals of Phamacotherapy 36(9): 1403-1413.
- José R, Brown J (2017) Adult pneumococcal vaccination: Advances, impact, and unmet needs. Curr Opin Pulm Med. 23(3): 225-30.
- WHO (2012) Pneumococcal Vaccines; WHO position paper. Weekly Epidemiological Record. 14(87): 129-144.
- Smith JC, Snider DE, Pickering LK (2009) Immunization policy development in the United States: The Role of the Advisory Committee on Immunization Practices. Ann Intern Med. 150(1): 45-49.
- Pavia M, Bianco A, Nobile CGA, Marinelli P, Angelillo IF (2009) Efficacy of pneumococcal vaccination in children younger than 24 months: A meta-analysis. Pediatrics.123(6):e1103.
- Russell FM, Carapetis JR, Burton RL, Lin J, Licciardi PV, et al. (2011) Opsonophagocytic activity following a reduced dose 7-valent pneumococcal conjugate vaccine infant primary series and 23-valent pneumococcal polysaccharide vaccine at 12 months of age. Vaccine 29(3): 535-544.
- Hsu HE, Shutt KA, Moore MR, Beall BW, Bennett NM, et al. (2009) Effect of pneumococcal conjugate vaccine on pneumococcal meningitis. N Engl J Med. 360(3): 244-256.
- Darkes M, Plosker G (2002) Pneumococcal conjugate vaccine (Prevnar; Pncrm7): A review of its use in the prevention of Streptococcus pneumoniae infection. Pediatric Drugs. 4: 609-630.
- Pelton SI, O’Klein J. (2002)The future of pneumococcal conjugate vaccines for prevention of pneumococcal diseases in infants and children. Pediatrics 110: 805-814.
- Casey CG (2010) Invasive pneumococcal disease in young children before licensure of 13-valent pneumococcal conjugate vaccine — United States. In: Shaw FE, (ed). (2010) MMWR Morbidity and Mortality Weekly Report: Centers for Disease Control and Prevention p. 253-257.
- Moran JS (2010) Invasive pneumococcal disease and 13-valent pneumococcal conjugate vaccine (Pcv13) coverage among children aged ≤ 59 months — selected U.S. regions, 2010-2011. In: Moolenaar RL, (ed). (2011) Morbidity Mortality Weekly Report: Centers for Disease Control and Prevention p. 1477-1481.
- Yeh SH, Gurtman A, Hurley DC, Block SL, Schwartz RH, et al. (2010) Immunogenicity and safety of 13-valent pneumococcal conjugate vaccine in infants and toddlers. Pediatrics 126: e493.
- Sorensen UBS, Henrichsen J, Chen HC, Szu SC (1990) Covalent linkage between the capsular polysaccharide and the cell wall peptidoglycan of Streptococcus pneumoniae revealed by immunochemical methods. Microb Pathog. 8: 325-334.
- Koskela M. (1987) Serum antibodies to pneumococcal c polysaccharide in children: response to acute pneumococcal otitis media or to vaccination. Pediatr Infect Dis J. 6: 519-526.
- Musher DM, Chapman AJ, Goree A, Jonsson S, Briles D, et al. (1986) Natural and vaccine-related immunity to streptococcus pneumoniae. J Infect Dis. 154: 245-256.
- Siber GR, Priehs C, Madore DV (1989) Standardization of antibody assays for measuring the response to pneumococcal infection and immunization. Pediatr Infect Dis J. 8: S84-S91.
- Concepcion NF, Frasch CE (2001) Pneumococcal type 22f polysaccharide absorption improves the specificity of a pneumococcal-polysaccharide enzyme-linked immunosorbent assay. Clin Diagn Lab Immunol. 8: 266-272.
- Coughlin RT, White AC, Anderson CA, Carlone GM, Klein DL, et al. (1998) Characterization of pneumococcal specific antibodies in healthy unvaccinated adults. Vaccine. 16(16): 1761-1767.
- Kyung HK, Jigui Y, Moon HN (2003) Efficiency of a pneumococcal opsonophagocytic killing assay improved by multiplexing and by coloring colonies. Clin Diagn Lab Immunol. 10(4): 616-621.
- Romero-Steiner S, Libutti D, Pais LB, Dykes J, Anderson P, et al. (1997) Standardization of an opsonophagocytic assay for the measurement of functional antibody activity against Streptococcus pneumoniae using differentiated Hl-60 cells. Clin Diagn Lab Immunol. 4(4): 415-422.
- Song JY, Moseley MA, Burton RL, Nahm MH (2013) Pneumococcal vaccine and opsonic pneumococcal antibody. J infect chemother : Official Journal of the Japan Society of Chemotherapy. 19(3): 412-425.
- Abbanat D, Davies TA, Amsler K, He W, Fae K, et al. (2017) Development and qualification of an opsonophagocytic killing assay to assess immunogenicity of a bioconjugated Escherichia coli vaccine. CVI. 24(12): e00123-17.
- Yang F, Gu J, Yang L, Gao C, Jing H, et al. (2017) Protective efficacy of the trivalent Pseudomonas aeruginosa vaccine candidate Pcrv-Opri-Hcp1 in murine pneumonia and burn models. Scientific reports. 7(1): 3957.
- American Academy of Pediatrics (2009) Pneumococcal infections. In: Pickering LK, Baker C, Kimberlin DW, Long SS, (eds). Red Book: Report of the Committee on Infectious Diseases. (28th edn) Elk Grove Village (IL): American Academy of Pediatrics. p. 524-535.
- Nahm MH, Briles DE, Yua X (2000) Development of a multi-specificity opsonophagocytic killing assay. Vaccine 18: 2768-2771.
- Lee H, Nahm MH, Burton R, Kim KH (2009) Immune response in infants to the heptavalent pneumococcal conjugate vaccine against vaccine-related serotypes 6a And 19a. CVI. 16(3): 376-381.
- Dagan R, Givon-Lavi N, Zamir O, Sikuler-Cohen M, Guy L, et al. (2002) Reduction of nasopharyngeal carriage of Streptococcus pneumoniae after administration of a 9-valent pneumococcal conjugate vaccine to toddlers attending day care centers. J Infect Dis.185: 927-936.
- Bogaert D, Sluijter M, De Groot R, Hermans PWM (2004) Multiplex opsonophagocytosis assay (Mopa): A useful tool for the monitoring of the 7-valent pneumococcal conjugate vaccine. Vaccine. 22: 4014-4020.
- Whitney CG, Pilishvili T, Farley MM, Schaffner W, Craig AS, et al. (2006) Effectiveness of seven-valent pneumococcal conjugate vaccine against invasive pneumococcal disease: A matched case-control study. Lancet. 368: 1495-1502.
- Poolman J, Frasch C, Nurkka A, Kayhty H, Biemans R, et al. (2011) Impact of the conjugation method on the immunogenicity of Streptococcus pneumoniae serotype 19f polysaccharide in conjugate vaccines. CVI. 18(2): 327-336.
- Jauneikaite E, Jefferies JM, Hibberd ML, Clarke SC (2012) Prevalence of Streptococcus pneumoniae Serotypes Causing Invasive and non-invasive disease in South East Asia: A review. Vaccine. 30(24): 3503-3514.
- Thisyakorn U, Chokephaibulkit K, Kosalaraksa P, Benjaponpitak S, Pancharoen C, et al. (2014) Immunogenicity and safety Of 23-valent pneumococcal polysaccharide vaccine as a booster dose in 12- to 18-month-old children primed with 3 doses of 7-valent pneumococcal conjugate vaccine. Hum Vaccines Immunother. 10(7): 1859-1865.

