Keywords
Pancreatectomy; Pancreatic Fistula; Surgical Stapling
Abbreviations
ISGPF: International Study Group on Pancreatic Fistula
INTRODUCTION
Pancreatic fistula formation remains the Achilles heel of pancreatic surgery and continues to challenge clinicians since it is the main cause of postoperative morbidity and mortality [1, 2]. Several factors, such as a fatty, soft, non-calcified, non-fibrotic gland [3, 4], have been suggested to increase the risk of pancreatic fistulae. In addition, the underlying pathology, e.g. duodenal, ampullary, and distal common bile duct lesions, have been shown to increase the risk. Despite this knowledge, the definition of the details of the risk profile of each individual patient is still an enigma [5, 6].
Resection of the pancreas to the left side of the superior mesenteric vein, defined as a distal pancreatectomy, is performed less frequently than resections of the pancreatic head [7]. Both a lower incidence of disease affecting this part of the pancreas and more advanced stages of cancer at the time of diagnosis explain this difference [7]. Distal pancreatectomy is considered by many surgeons to be a less demanding and complex operation than a Whipple procedure, a view which is far from well substantiated [8, 9]. With centralization of pancreatic resections, the mortality rate has decreased considerably [10, 11, 12, 13, 14, 15, 16, 17, 18], but morbidity remains substantial [10, 11, 12, 13, 14, 15], even after distal pancreatectomy. Overall postoperative morbidity has been reported to range from 9 to 57% [1, 3, 10, 12, 19, 20]. The most common and important postoperative complication after distal pancreatectomy is pancreatic fistula, which may manifest itself as a frank fistula or an intra-abdominal fluid collection. Pancreatic fistula is associated with both local and general complications (e.g. intraabdominal fluid abscesses, wound infection, delayed gastric emptying, respiratory complications and sepsis) but it has additional important implications in terms of the need for revisional surgery and drainage with a prolonged hospital stay [11, 13].
Pancreatic fistula is thought to depend on a variety of factors, some of which are surgeon-dependent [21, 22, 23]. There is, for example, significant variation in and debate about which surgical technique should be used for closure of the pancreatic transection area [5, 24, 25, 26, 27, 28, 29, 30]. Besides this, other risk factors are poorly characterized.
The aim of the current study was to analyze factors which may affect the risk of pancreatic fistulae after distal pancreatectomy.
METHODS
A study was conducted on a cohort of consecutive patients undergoing distal pancreatectomy between March 1999 and December 2007 at the Karolinska University Hospital. All data on demographics, clinicopathological features, operative information, complications and in-hospital mortality were collected prospectively in the local pancreatic database.
Definition of Pancreatic Fistula
Patients were categorized as having developed a clinically relevant fistulae (i.e. grade B or C) based on the definitions of the International Study Group on Pancreatic Fistula (ISGPF). In other words, a clinically significant pancreatic fistula is a fistula requiring any therapeutic intervention (grade B) or a fistula with severe clinical sequelae (grade C). The incidence of biochemical leakage (regarded as grade A), defined as any measurable output on, or after, the 3rd postoperative day from an operatively positioned abdominal drain and displaying pancreatic amylase more than 3 times the upper serum reference value, was not included in the analyses of this study.
Radiological Analysis
Preoperative computed tomography or magnetic resonance imaging were analyzed by the same radiologist who was blinded to the postoperative course. The volume of the pancreatic remnant was measured using a Voxar® 3D workstation (Barco NV, Kortrijk, Belgium) with 3D segmentation and volume calculation (Figures 1 and 2). The length and width of the resection plane were measured. The caliber of the main pancreatic duct was measured in the resection plane and in the head of the pancreas, as was the distance of the resection margin from the lesion.
Figure 1. Computed tomography of the pancreas. 3D volume
rendering image of the pancreas with the remaining pancreas shown
in blue.
Figure 2. Computed tomography of the pancreas showing 3D
segmentation and volume calculation of the pancreatic remnant (in
blue) in transverse (a.), coronal (b.), and sagittal (c.) images.
ETHICS
The study protocol conforms to the ethical guidelines of the “World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004. The study protocol was approved by the Ethics Committee of the Karolinska University Hospital, Karolinska Institute, Sweden.
STATISTICS
Binary logistic regression analysis was performed to identify the risk factors for pancreatic fistulae, with and without simultaneous adjustment for competing risk factors. Crude associations were studied in a univariate model which was followed by a multivariate analysis of significant factors. Robust standard errors were computed to account for the clustering of patients by a single surgeon. The associations were presented as odds ratios (ORs) with 95% confidence intervals (CIs). The unpaired Students’ t-test was used to compare mean values. Data are presented as medians and ranges or frequencies. All tests of statistical significance were two-sided, and statistical significance was considered to occur at alpha less than 0.05. The statistical analyses were performed using SPSS 17.0 software (SPSS Inc, Chicago, IL, USA).
RESULTS
Patients, Surgery, and Diagnoses
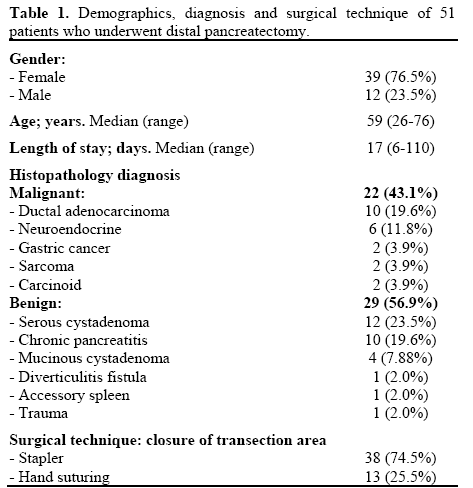
During the study period, a total of 51 patients (39 females, 12 males) having a median age of 59 years underwent distal pancreatectomy. Splenectomy was carried out in 47 patients (92.2%) and the median hospital stay was 17 days. The diagnosis was malignant in 22 patients (43.1%) and benign or premalignant in 29 (56.9%) patients. The transection area was closed by means of a stapler in 38 cases (74.5%) and by hand suturing in 13 (25.5%). These data are shown in detail in Table 1.
Surgical Complications
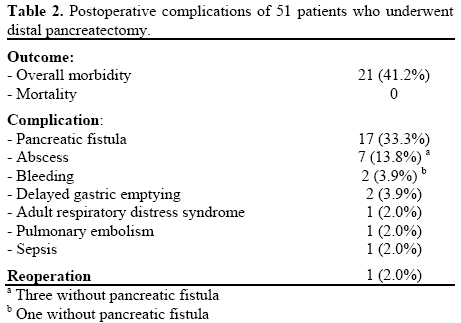
Overall, 21 patients (41.2%) experienced postoperative complications (Table 2). The most common complication was pancreatic fistula, which was observed in 17 patients (33.3%). Three of the 7 patients with intra-abdominal abscesses had a local abscess without apparent pancreatic leakage. The occurrence of a pancreatic fistula increased the median length of hospitalization from 11 (range: 6-16 days) to 30 days (range: 14-110 days) (P=0.014). One patient required reoperation (2.0%); otherwise, complications were treated conservatively without any mortality (Table 2).
Risk Factor Analysis
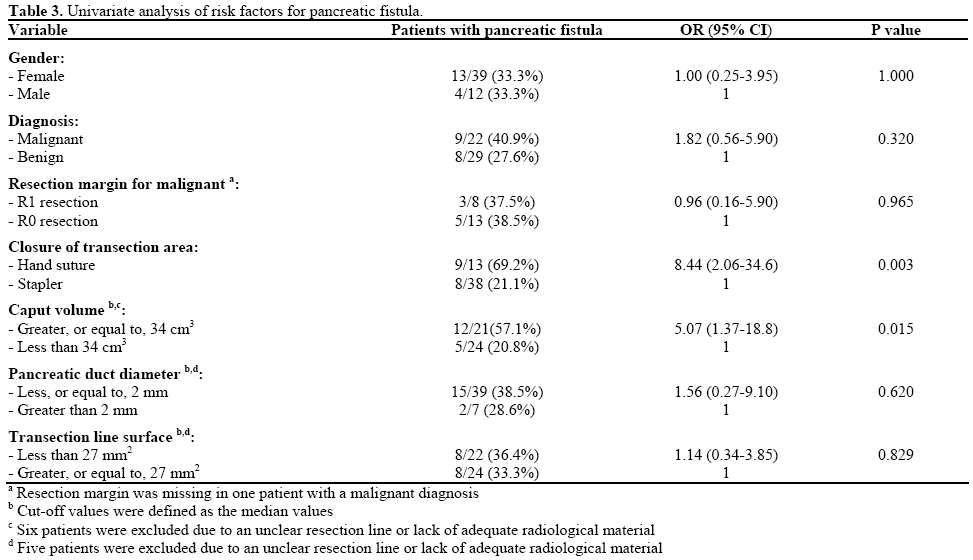
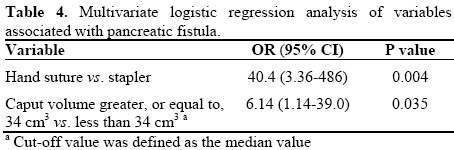
Pancreatic fistulae occurred more frequently after hand suturing (9/13, 69.2%) as compared to the use of a stapler (8/38, 21.1%). At univariate analysis, hand suturing of the transection surface significantly increased the risk of a pancreatic fistula (OR: 8.44; 95% CI: 2.06-34.6; P=0.003). A radiological median value volume of the remaining gland equal to, or greater than, 34 cm3 exerted a negative impact on the risk of a pancreatic fistula (OR: 5.07; 95% CI: 1.37- 18.8) (Table 3). In the subsequent multivariate analysis, both factors remained independent risk factors for pancreatic fistulae (Table 4).
DISCUSSION
It has clearly been demonstrated that distal pancreatectomy is associated with significant morbidity, which is very much related to the occurrence and perpetuation of a pancreatic fistula. The internationally recognized classification of pancreatic fistula [31] is very helpful in attempts to define those at risk. However, the design of the present analysis, as that of many other studies in the field, does not allow a comprehensive elucidation of issues and consequences related to those fistulae which are grade A and B [1, 5, 10, 20, 22, 32]. However, it is reasonable to assume that abscess formation in close conjunction with the resection area is closely linked to such phenomena. We did not include such abscesses in the final analyses of the pancreatic fistulae because we were unable to detect any pancreatic juice remnant at the time of abscess puncture or drainage.
The surgical method for closure of the transected pancreatic gland is still a matter of debate. A recently performed careful survey of the current literature [5, 19, 24, 33] brought into focus the fact that most studies were of suboptimal quality and underpowered. The conclusion was that additional well-designed, randomized clinical trials were urgently needed. The current study reporting a strong association between pancreatic fistulae and the use of a manual suturing technique reinforces the need for such trials. It is clear that laparoscopic resection of the body and tail of the gland is preferred in many institutions [34, 35, 36]. This operative approach does not resolve the problem of leakage and the morbidity rate is comparable to open procedures [37].
A novel finding of the present study consisted in the association between the size of the remaining gland and the risk of pancreatic fistulae. This is a plausible and logical observation since the larger the volume of the remaining gland, the greater the quantity of actively secreting parenchyma with the potential of exerting detrimental, digestive effects on the sealed transection area. This brings to our attention mechanisms by which the secreted juice from the remaining pancreatic head may be deviated away from the area of the closed transection line. Downstream control by use of a pancreatic stent would be such an option [38]; again something which has to be explored in a clinical trial where enrolled patients must be stratified also with regard to the volume of the tissue drained through the papilla.
We were unable to find any impact of other radiological variables, such as pancreatic and biliary duct diameter, area of the transected surface or gross amount of resected tissue. In this context, it is interesting to recall a recent observation in which dynamic magnetic resonance imaging has been hypothesized to be able to to assess the texture of the gland tissue in the form of high and normal contrast enhancement, thereby having the potential of predicting the risk of leakage after a Whipple resection [32]. If this technology is combined with volume assessments, a novel and precise instrument, with an obvious clinical potential, might well be launched and therefore deserves to be tested in well-designed clinical trial protocols. In conclusion, the development of pancreatic fistulae after distal pancreatectomy remains a challenge. The technique of closure of the transected surface of the pancreas and the volume of the remaining gland were found to affect the risk of pancreatic fistulae.
Conflict of interest
Authors report no conflict of interest
References
- Fahy BN, Frey CF, Ho HS, Beckett L, Bold RJ. Morbidity, mortality, and technical factors of distal pancreatectomy. Am J Surg 2002; 183:237-41. [PMID 11943118]
- Cullen JJ, Sarr MG, Ilstrup DM. Pancreatic anastomotic leak after pancreaticoduodenectomy: incidence, significance, and management. Am J Surg 1994; 168:295-8. [PMID 7524375]
- Yang YM, Tian XD, Zhuang Y, Wang WM, Wan YL, Huang YT. Risk factors of pancreatic leakage after pancreaticoduodenectomy. World J Gastroenterol 2005; 11:2456-61. [PMID 15832417]
- Mathur A, Pitt HA, Marine M, Saxena R, Schmidt CM, Howard TJ, et al. Fatty pancreas: a factor in postoperative pancreatic fistula. Ann Surg 2007; 246:1058-64. [PMID 18043111]
- Knaebel HP, Diener MK, Wente MN, Buchler MW, Seiler CM. Systematic review and meta-analysis of technique for closure of the pancreatic remnant after distal pancreatectomy. Br J Surg 2005; 92:539-46. [PMID 15852419]
- Adams DB. The pancreatic anastomosis: the danger of a leak, which anastomotic technique is better? J Gastrointest Surg 2009; 13:1182-3. [PMID 19333663]
- Andren-Sandberg A, Wagner M, Tihanyi T, Lofgren P, Friess H. Technical aspects of left-sided pancreatic resection for cancer. Dig Surg 1999; 16:305-12. [PMID 10449975]
- Adam U, Makowiec F, Riediger H, Trzeczak S, Benz S, Hopt UT. Distal pancreatic resection: indications, techniques and complications. Zentralbl Chir 2001; 126:908-12. [PMID 11753802]
- Cogbill TH, Moore EE, Morris JA Jr, Hoyt DB, Jurkovich GJ, Mucha P Jr, et al. Distal pancreatectomy for trauma: a multicenter experience. J Trauma 1991; 31:1600-6. [PMID 1749029]
- Kleeff J, Diener MK, Z'graggen K, Hinz U, Wagner M, Bachmann J, et al. Distal pancreatectomy: risk factors for surgical failure in 302 consecutive cases. Ann Surg 2007; 245:573-82. [PMID 17414606]
- Lillemoe KD, Kaushal S, Cameron JL, Sohn TA, Pitt HA, Yeo CJ. Distal pancreatectomy: indications and outcomes in 235 patients. Ann Surg 1999; 229:693-8. [PMID 10235528]
- Balcom JH 4th, Rattner DW, Warshaw AL, Chang Y, Fernandez-del Castillo C. Ten-year experience with 733 pancreatic resections: changing indications, older patients, and decreasing length of hospitalization. Arch Surg 2001; 136:391-8. [PMID 11296108]
- Fernandez-del Castillo C, Rattner DW, Warshaw AL. Standards for pancreatic resection in the 1990s. Arch Surg 1995; 130:295-9. [PMID 7887797]
- Büchler MW, Wagner M, Schmied BM, Uhl W, Friess H, Z'graggen K. Changes in morbidity after pancreatic resection: toward the end of completion pancreatectomy. Arch Surg 2003; 138:1310-4. [PMID 14662530]
- Birkmeyer JD, Siewers AE, Finlayson EV, Stukel TA, Lucas FL, Batista I, et al. Hospital volume and surgical mortality in the United States. N Engl J Med 2002; 346:1128-37. [PMID 11948273]
- Cameron JL, Riall TS, Coleman J, Belcher KA.One thousand consecutive pancreaticoduodenectomies. Ann Surg 2006; 244:10-5. [PMID 16794383]
- Hines OJ, Reber HA. Pancreatic surgery. Curr Opin Gastroenterol 2005; 21:568-72.
- Eppsteiner RW, Csikesz NG, McPhee JT, Tseng JF, Shah SA. Surgeon volume impacts hospital mortality for pancreatic resection. Ann Surg 2009; 249:635-40. [PMID 19300225]
- Balzano G, Zerbi A, Cristallo M, Di Carlo V. The unsolved problem of fistula after left pancreatectomy: the benefit of cautious drain management. J Gastrointest Surg 2005; 9:837-42. [PMID 15985241]
- Nathan H, Cameron JL, Goodwin CR, Seth AK, Edil BH, Wolfgang CL, et al. Risk factors for pancreatic leak after distal pancreatectomy. Ann Surg 2009; 250:277-81. [PMID 19638926]
- Ridolfini MP, Alfieri S, Gourgiotis S, Di Miceli D, Rotondi F, Quero G, et al. Risk factors associated with pancreatic fistula after distal pancreatectomy, which technique of pancreatic stump closure is more beneficial? World J Gastroenterol 2007; 13:5096-100. [PMID 17876875]
- Ferrone CR, Warshaw AL, Rattner DW, Berger D, Zheng H, Rawal B, et al. Pancreatic fistula rates after 462 distal pancreatectomies: staplers do not decrease fistula rates. J Gastrointest Surg 2008; 12:1691-7. [PMID 18704597]
- Kajiyama Y, Tsurumaru M, Udagawa H, Tsutsumi K, Kinoshita Y, Akiyama H. Quick and simple distal pancreatectomy using the GIA stapler: report of 35 cases. Br J Surg 1996; 83:1711. [PMID 9038547]
- Olah A, Issekutz A, Belagyi T, Hajdu N, Romics L Jr. Randomized clinical trial of techniques for closure of the pancreatic remnant following distal pancreatectomy. Br J Surg 2009; 96:602-7. [PMID 19434697]
- Bilimoria MM, Cormier JN, Mun Y, Lee JE, Evans DB, Pisters PW. Pancreatic leak after left pancreatectomy is reduced following main pancreatic duct ligation. Br J Surg 2003; 90:190-6. [PMID 12555295]
- Pannegeon V, Pessaux P, Sauvanet A, Vullierme MP, Kianmanesh R, Belghiti J. Pancreatic fistula after distal pancreatectomy: predictive risk factors and value of conservative treatment. Arch Surg 2006; 141:1071-6. [PMID 17116799]
- Wagner M, Gloor B, Ambühl M, Worni M, Lutz JA, Angst E, Candinas D. Roux-en-Y drainage of the pancreatic stump decreases pancreatic fistula after distal pancreatic resection. J Gastrointest Surg 2007; 11:303-8. [PMID 17458602]
- Okabayashi T, Kobayashi M, Sugimoto T, Namikawa T, Okamoto K, Hokimoto N, Araki K. Postoperative pancreatic fistula following distal pancreatectomy for pancreatic neoplasm; can pancreatic fistula be prevented? Hepatogastroenterology 2004; 51:1838-41. [PMID 15532838]
- Ohwada S, Ogawa T, Tanahashi Y, Nakamura S, Takeyoshi I, Ohya T, et al. Fibrin glue sandwich prevents pancreatic fistula following distal pancreatectomy. World J Surg 1998; 22:494-8. [PMID 9564295]
- Velanovich V. The use of tissue sealant to prevent fistula formation after laparoscopic distal pancreatectomy. Surg Endosc 2007; 21:1222. [PMID 17484008]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005; 138:8-13. [PMID 16003309]
- Dinter DJ, Aramin N, Weiss C, Singer C, Weisser G, Schoenberg SO, et al. Prediction of anastomotic leakage after pancreatic head resections by dynamic magnetic resonance imaging (dMRI). J Gastrointest Surg 2009; 13:735-44. [PMID 19057965]
- Sheehan MK, Beck K, Creech S, Pickleman J, Aranha GV. Distal pancreatectomy: does the method of closure influence fistula formation? Am Surg 2002; 68:264-7. [PMID 11893105]
- Mabrut JY, Fernandez-Cruz L, Azagra JS, et al. Laparoscopic pancreatic resection: results of a multicenter European study of 127 patients. Surgery 2005; 137:597-605. [PMID 15962401]
- Kooby DA, Gillespie T, Bentrem D, Nakeeb A, Schmidt MC, Merchant NB, et al. Left-sided pancreatectomy: a multicenter comparison of laparoscopic and open approaches. Ann Surg 2008; 248:438-46. [PMID 18791364]
- Taylor C, O'Rourke N, Nathanson L, Martin I, Hopkins G, Layani L, et al. Laparoscopic distal pancreatectomy: the Brisbane experience of forty-six cases. HPB (Oxford) 2008; 10:38-42. [PMID 18695757]
- Borja-Cacho D, Al-Refaie WB, Vickers SM, Tuttle TM, Jensen EH. Laparoscopic distal pancreatectomy. J Am Coll Surg 2009; 209:758-65. [PMID 19959046]
- Fischer CP, Bass B, Fahy B, Aloia T. Transampullary pancreatic duct stenting decreases pancreatic fistula rate following left pancreatectomy. Hepatogastroenterology 2008; 55:244-8. [PMID 18507117]



