Keywords
Fistula; Pancreatic Neoplasms; Pancreaticoduodenectomy; Prognosis; Survival
Abbreviations
ESPAC: European Study Group for Pancreatic Cancer; ISGPF: International Study Group of Pancreatic Fistula
INTRODUCTION
Pancreatic ductal adenocarcinoma is an aggressive cancer and surgical resection remains the only potentially curative option. Even in specialist centres, only 15% of patients diagnosed with pancreatic cancer are found suitable for surgical resection as the majority of these patients present with advanced disease [1]. Despite improvements in post operative care and the routine use of adjuvant chemotherapy [2], prognosis remains poor with a median survival of 13.3 months and 5-year survival of 10.5% [3]. Extended resections have not been shown to improve survival in randomised trials [4].
Pancreatic leaks following pancreaticoduodenectomy are a major cause of post operative morbidity and mortality [5]. The variations in the method of pancreatic stump management and the volume of literature on the subject indicate the ongoing efforts to prevent this complication. Anastomotic leak has been reported as an adverse prognostic factor affecting the long term survival of colorectal cancer patients [6, 7, 8, 9]. Studies have not convincingly demonstrated the effect of pancreatic leakage following Whipple’s resection on long term outcome.
The aim of this study is to analyse the impact of pancreatic leak on disease recurrence and long term survival in patients who underwent a pancreaticoduodenectomy at Addenbrooke’s hospital for pancreatic head ductal adenocarcinoma.
PATIENTS AND METHODS
All patients who underwent a pancreaticoduodenectomy from June 2002 to June 2007 at the HPB Unit in Addenbrooke’s Hospital, Cambridge were identified from a prospectively held pancreatic database. Patients with a final postoperative histological diagnosis of pancreatic ductal adenocarcinoma were selected for inclusion in the study.
In all patients a standard Whipple’s pancreaticoduodenectomy was performed. Reconstruction consisted of an end-to-side pancreaticojejunostomy and an end-to-side- hepaticojejunostomy on a 70 cm Rouxen- Y loop. A gastrojejunal anastomosis and a side-toside enteroenterostomy were also performed. Standard (non-extended) lymphadenectomy was carried out in all cases.
Patients undergoing Whipple’s resection had drain fluid amylase measured on a daily basis until drain removal. Pancreatic leaks were defined as drain output of any measurable volume of fluid on or after postoperative day 3 with amylase content 3 times greater than serum amylase activity according to the International Study Group of Pancreatic Fistula (ISGPF) definition [10]. In addition, fistula severity was graded as A, B, C according to ISGPF clinical criteria as follows: grade A fistula (a transient, asymptomatic fistula with only elevated drain amylase levels and treatments or deviation in clinical management are not required); grade B fistula (a symptomatic, clinically apparent fistula requiring diagnostic evaluation and therapeutic management); and grade C fistula (a severe, clinically significant fistula requiring a major deviations in clinical management and unequivocal aggressive therapeutic interventions). All patients received prophylactic octreotide (Sandostatin®, Novartis Parmaceutical, Camberley, United Kingdom) 100 micrograms administered subcutaneously 3 times a day for 5 days and which was subsequently continued in patients with a pancreatic leak. Patients with missing fluid amylase values were excluded from the study.
Patients with a pancreatic leak were managed conservatively with a regimen of nil by mouth, total parenteral nutrition or enteral nutrition through a feeding jejunostomy, percutaneous drainage of intrabdominal collections, treatment of sepsis, wound care and octreotide. Laparotomy with wash-out and completion pancreatectomy were reserved for patients with generalized peritonitis. All patients were followed-up life-long in the surgical clinic on a six monthly basis. CA 19-9 levels and CT scan of the chest, abdomen and pelvis were carried out during each follow-up visit. Patients with a final postoperative histology of pancreatic ductal adenocarcinoma were considered for adjuvant chemotherapy with a 5-fluorouracil or gemcitabine (mostly within the European Study Group for Pancreatic Cancer (ESPAC-3) trial [11]). None of these patients received pre-operative chemo- or radiotherapy.
Demographic details, International Union Against Cancer (UICC) disease stage, 30-day mortality, mean hospital stay and administration of adjuvant chemotherapy were noted from the database. Recurrence was deemed to be present if further lesions were noted on the follow-up CT scans, with or without an associated rise in CA 19-9 levels. Patients were divided in two groups: those with leaks and those without.
ETHICS
Informed consent for research was obtained from each patient and the study protocol conforms to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki 1, Finland, June 1964, as revised in Tokyo2004.
STATISTICS
Overall survival was calculated by using the Kaplan- Meier method and was compared between the two groups by means of the log-rank test. Comparison of demographic details and recurrence between the two groups was performed by using the Fisher’s exact tests and the linear-by-linear chi-square. A two-tailed P value less than 0.05 was considered significant. SPSS 16.0 (SPSS, Chicago, Illinois, USA) was used for statistical analysis.
RESULTS
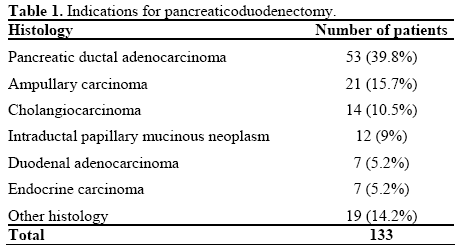
There were 133 Whipple’s resections carried out during the study period. The indications for pancreaticoduodenectomy are illustrated in Table 1. Of the 53 patients with pancreatic ductal adenocarcinoma, 6 (11.3%) were excluded due to missing data. Thus 47 patients satisfied the inclusion criteria for the study of whom 9 had a pancreatic leak (19.1%) graded A (2 patients), B (6 patients) and C (1 patient). All patients with pancreatic leak were managed conservatively except for one patient (11.1%) who underwent completion total pancreatectomy.
Median follow-up was 30.8 months. Demographic and clinicopathological data for patients with and without leaks are given in Table 2. Postoperative morbidity was 29.8% (14 cases). There were no significant differences in the demographic details between the two groups. Overall median survival was 19 months for the whole cohort. Median survival in the pancreatic leak group was 16.5 months and median survival in the group without pancreatic leak was 27.5 months. However, this was not statistically significant (Figure 1; P=0.411, log-rank test).
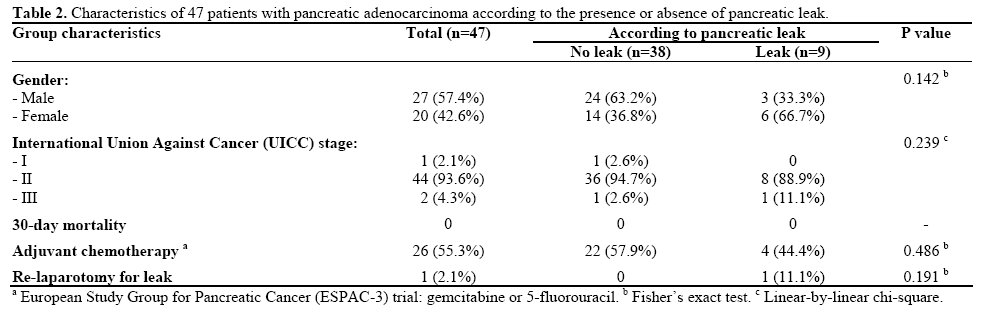
Figure 1: Kaplan-Meier curve showing no significant difference in
the overall survival following pancreaticoduodenectomy between 9
patients with pancreatic leaks and 38 patients without pancreatic
leaks.
Recurrence occurred in 70.2% of patients (33/47), of whom 88.9% (8/9) were in the leak group and 65.8% (25/38) in the group without pancreatic leak. No statistically significant difference was noted in terms of presence of recurrence between the two groups (P=0.244, Fisher’s exact test).
DISCUSSION
Pancreatic anastomotic leaks following pancreaticoduodenectomy have an obvious negative impact on the perioperative morbidity and mortality. However, it is less clear whether this effect extends itself to long term overall and recurrence free survival. Studies which look at long term outcome following Whipple’s resection usually include peri-operative deaths (often due to pancreatic leaks) in their survival analysis. Inclusion of such deaths confuses the issue of whether pancreatic leaks have a direct effect on the oncological outcomes following Whipple’s resection. In the present study, in line with increasing numbers of publications from large volume centres, there were no perioperative deaths. Hence the findings give a more accurate indication of the effects of pancreatic leaks on the overall and disease free survival.
The presence of a significant post-operative pancreatic leak could be associated with reduced immunity in the patient, thus leading to an increased risk of recurrence and poor survival. Some authors have demonstrated that post operative drain fluid cytology from the pancreatic bed after ‘curative’ resection contained malignant cells and was related to long term outcome [12]. It has also been shown that exfoliated malignant cells have the potential to grow in-vitro and in immunosuppressed animal models [13]. We were unable to show a statistically significant difference in the overall and disease free survival in patients with pancreatic leak.
It could also be argued that the local sepsis and caustic environment associated with a pancreatic leak might have a local beneficial effect in inhibiting recurrence by destroying any residual malignant cells remaining in the pancreatic bed. However, there is nothing in our study to support this hypothesis with equivalent survival shown in both groups. It is not clear from this study whether the presence of a pancreatic leak in the post operative period might have an effect in reducing life span from natural other than cancer related causes. It is possible that major surgery with its inherent complications might enhance any associated comorbidities in the patient thus reducing the overall life span. However, this study was neither designed nor powered to look at reduced life span from non cancer causes. Looking for any underlying association with post-operative pancreatic leaks we found that there were no major demographic or clinicopathological differences between the pancreatic leak group and the group without pancreatic leaks. We have kept the selection criteria for this study deliberately strict by including only those patients with pancreatic head ductal adenocarcinoma (excluding periampullary carcinomas, cholangiocarcinomas, cystic cancers and neuroendocrine carcinomas). Similarly the definition of pancreatic leak was kept uniform and objective by adopting the ISGPF criteria. This, we believe, strengthens the conclusions of the study despite the low number of patients. The limitations of this retrospective study would need to be addressed in a larger prospective cohort study in order to confirm these findings.
Conflict of interest The authors have no potential conflict of interest
References
- Neoptolemos JP, Russell RC, Bramhall S, Theis B. Low mortality following resection for pancreatic and periampullary tumours in 1026 patients: UK survey of specialist pancreatic units. UK Pancreatic Cancer Group. Br J Surg 1997; 84:1370-6. [PMID 9361591]
- Chua YJ, Cunningham D. Adjuvant treatment for resectable pancreatic cancer. J Clin Oncol 2005; 23:4532-7. [PMID 16002844]
- Alexakis N, Halloran C, Raraty M, Ghaneh P, Sutton R, Neoptolemos JP. Current standards of surgery for pancreatic cancer. Br J Surg 2004; 91:1410-2. [PMID 15499648]
- Pedrazzoli S, DiCarlo V, Dionigi R, Mosca F, Pederzoli P, Pasquali C, et al. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: a multicenter, prospective, randomized study. Lymphadenectomy Study Group. Ann Surg 1998; 228:508-17. [PMID 9790340]
- Reid-Lombardo KM, Farnell MB, Crippa S, Barnett M, Maupin G, Bassi C, Traverso LW; Pancreatic Anastomotic Leak Study Group. Pancreatic anastomotic leakage after pancreaticoduodenectomy in 1,507 patients: a report from the Pancreatic Anastomotic Leak Study Group. J Gastrointest Surg 2007; 11:1451-8. [PMID 17710506]
- Law WL, Choi HK, Lee YM, Ho JW, Seto CL. Anastomotic leakage is associated with poor long-term outcome in patients after curative colorectal resection for malignancy. J Gastrointest Surg 2007; 11:8-15. [PMID 17390180]
- McArdle CS, McMillan DC, Hole DJ. Impact of anastomotic leakage on long-term survival of patients undergoing curative resection for colorectal cancer. Br J Surg 2005; 92:1150-4. [PMID 16035134]
- Walker KG, Bell SW, Rickard MJ, Mehanna D, Dent OF, Chapuis PH, Bokey EL. Anastomotic leakage is predictive of diminished survival after potentially curative resection for colorectal cancer. Ann Surg 2004; 240:255-9. [PMID 15273549]
- 9. Ptok H, Marusch F, Meyer F, Schubert D, Gastinger I, Lippert H; Study Group Colon/Rectum Carcinoma (Primary Tumour). Impact of anastomotic leakage on oncological outcome after rectal cancer resection. Br J Surg 2007; 94:1548-54. [PMID 17668888]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005; 138:8-13. [PMID 16003309]
- ESPAC-3(v2) Phase III Adjuvant Trial in Pancreatic Cancer Comparing 5FU and D-L-Folinic Acid vs. Gemcitabine. Leeds, UK: National Cancer Research Network Trials Portfolio, 2004.
- Ishikawa O, Wada H, Ohigashi H, Doki Y, Yokoyama S, Noura S, et al. Postoperative cytology for drained fluid from the pancreatic bed after "curative" resection of pancreatic cancers: does it predict both the patient's prognosis and the site of cancer recurrence? Ann Surg 2003; 238:103-10. [PMID 12832972]
- Skipper D, Jeffrey MJ, Cooper AJ, Taylor I, Alexander P. Preferential growth of bloodborne cancer cells in colonic anastomoses. Br J Cancer 1988; 57:564-8. [PMID 3408643]


