Keywords
Morbidity; Pancreatectomy; Quality of Life
Abbreviations
EORTC: European Organisation for Research and Treatment of Cancer; FACT: Functional Assessment of Cancer Therapy
INTRODUCTION
Through a greater expansion of training and better post-operative care, pancreatectomies for malignant and benign disease are increasingly being performed worldwide. Studies have shown that pancreatectomy is being performed in increasing numbers for various malignant and benign diseases of the pancreas and periampullary region [1]. However, despite the increasing number of pancreatectomies, there are very few studies exploring the quality of life (QoL) in patients undergoing pancreatectomy for benign and especially for malignant disease of the pancreas [2]. Thus more studies are needed for comparative behavior of the QoL of patients operated on for pancreatic diseases [2].
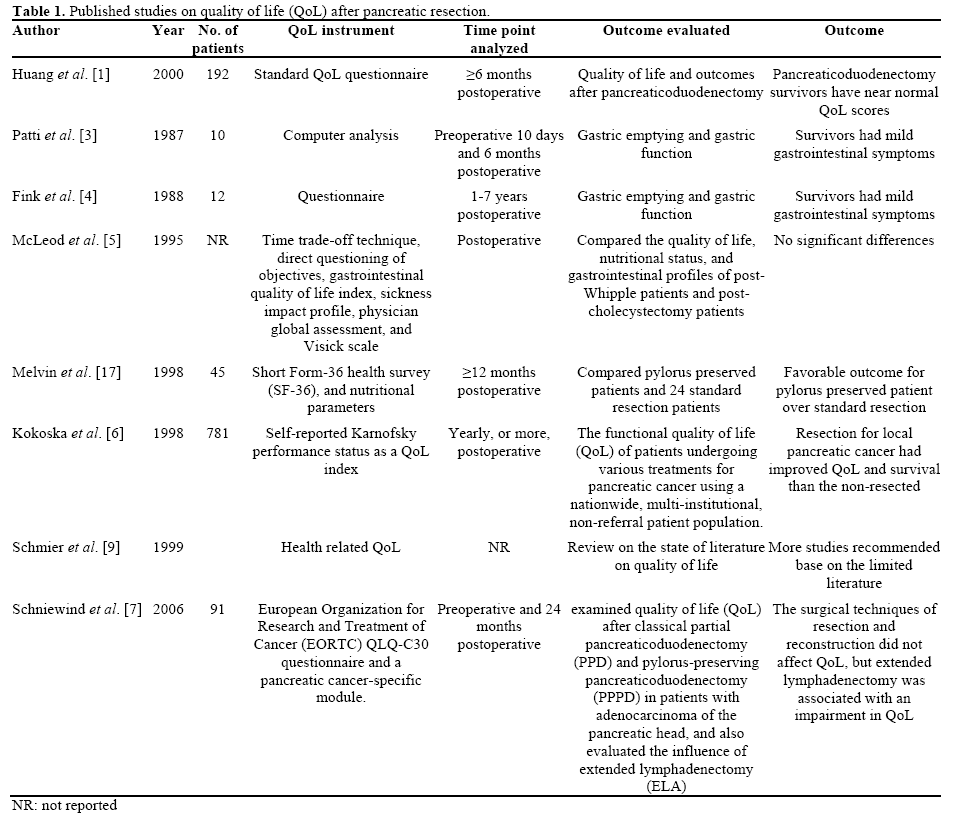
Recent studies that have evaluated QoL in pancreatectomy have reported conflicting outcomes (Table 1). Huang et al. [1] demonstrated that pancreatectomy survivors have near-normal QoL scores. Patti et al. [3] and Fink et al. [4] found that pancreatectomy patients have mild gastrointestinal symptoms. McLeod et al. [5] demonstrated that there was no significant difference between pancreatectomy patients compared to cholecystectomy patients regarding QoL after surgery. Kokoska et al. [6] reported an improvement in QoL and survival for pancreatectomy patients compared to nonpancreatectomy patients. Schniewind et al. [7] on the other hand concluded that surgical techniques of resection and reconstruction did not affect QoL, but extended lymphadenectomy was associated with impairment in QoL. Despite these studies on QoL, in 2007 Pezzilli et al. [8] joined Schmier et al. [9] in suggesting the need for more prospective evaluations into the research of QoL. Similarly, only two of these studies [3, 7] have evaluated QoL both pre-operatively and postoperatively, which is a key protocol requirement to ensure that a relationship to baseline QoL is possible. Thus the primary goal of this study was to analyze the QoL changes reported by patients with pancreatic cancer undergoing pancreatectomy.
METHODS
Study Design
A prospective evaluation of patients undergoing pancreatectomy for benign or malignant disease was recruited into this observational study of QoL from March 2006 to March 2008. QoL assessment was performed pre-operatively at the time of pre-admission testing, and then again at first follows visit (2-3 postoperative weeks), 6 weeks, 3 months and 6 months.
Patients
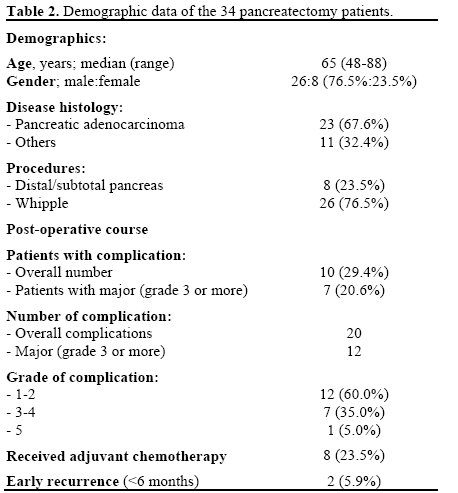
Thirty-four patients agreed to participate in this study. This included 26 men (76.5%) and 8 women (23.5%), with a median follow-up of 1.2 years (range: 0.3-2.9 years). Basic data also included the prevalence of comorbidities (n=15, 44.1%), length of stay (median 6 days; range: 5-19 days), and overall operative time (median 200 minutes; range: 160-300 minutes). The pancreatic resection group was: Whipple 26 (76.5%), and distal/subtotal pancreas in 8 (23.5%). Adjuvant chemotherapy was administered in 8 patients (23.5%), most often in conjunction with radiotherapy (n=6). A total of 20 complications occurred in 10 patients. Major (grade 3-5) complications occurred in 7 patients. Early (<6 month) recurrence was noted in 2 patients (5.9%) (Tables 2 and 3). All eligible patients completed the questionnaire at the established time points apart from 3 patients (8.8%) that did not complete the 6 month QoL metric due to refusal for participation (n=2) or death (n=1).

Surgery
The decision to perform pancreatic resection was at the surgeon’s discretion. The procedure was carried out following the protocol as described by Martin et al. [10].
Comorbidities were defined as significant cardiac (past coronary infraction), pulmonary, renal, or pancreatic dysfunction. Additional organ resection excluded cholecystectomy and included colon resection, gastric, or any other solid organ in combination with pancreatic resection. Therefore, cholecystectomy at the time of pancreatic resection was not considered as an additional organ.
Postoperative complications and the length of hospital stays were recorded and graded by using our standard classification scale of complications which has been reported previously [11]. For patients with more than one complication, comparisons of in-hospital and 90- day postoperative complications were evaluated by assigning the complication with the highest severity for each patient. Complications were defined by publishing criteria [10]. A postoperative death was defined as any patient death that occurred within 90 days postoperatively. Anemia was defined as the day of discharge hemoglobin. Anemia was categorized according to values <10 g/dL and ≥10 g/dL, based on the fact this is a more clinically relevant value in post pancreatectomy patients [12], and occurred in 17 (50.0%) patients.
Study Procedures
This study was observational; no study-specific treatment was provided to these patients through this investigation. We used a pre-post test design to assess a patient’s symptoms and concerns before and after pancreatic resection. Quality of life parameters were recorded prospectively by a single trained interviewer preoperatively, at the first post-operative outpatient visit, and at the 6-week, 3-month, and 6-month followup using the European Organisation for Research and Treatment of Cancer (EORTC QLQ-C30: https://groups.eortc.be) instrument and the Functional Assessment of Cancer Therapy FACT-Anemia (FACTAn: https://www.facit.org) [12]. The reason for the use of these QoL measures was based on our past experience with these instruments and the sensitivity of identifying clinically relevant QoL effects following abdominal surgery [13, 14].
Upon enrollment, the study coordinator, research assistant, or investigator completed the treatment history and demographics. At this time the patients completed a baseline questionnaire battery consisting of EORTC QLQ-C30 and FACT-An. Upon discharge after pancreatectomy, each patient completed the Functional Health and Symptom Index (FHSI-8) [14, 15], which includes questions that are applicable to the hospitalization (the data of this questionnaire are not presented in the present study). At the remaining time points, each patient completed the EORTC QLQ-C30 questionnaire. Clinical events (type of surgery, complications, and repeat hospitalization) were documented at the 4 follow-up time-points. These visits coincided with the scheduled follow-up appointments and did not burden the patient. If a patient missed an appointment or continued follow-up elsewhere, the follow-up questionnaire was mailed to the patient. For those patients that survived less than 6 months after surgery, QoL assessment was continued until the last follow-up visit by the patient. All questionnaires were completed in English.
The quality of the data obtained from each patient was evaluated when the patient completed all questionnaire forms at each visit. The study coordinator, research assistant, or investigator who had enrolled the patient reviewed each form immediately after receiving them to identify any missing data.
The quality of data entry is evaluated by the use of range checks on all variables and by double data entry for small portion (10%) of the data. This process allowed for the evaluation of the accuracy of the data entered by the primary data entry assistant.
QoL Instrument
The FACT-An is a validated instrument for assessing QoL in patient with anemia following pancreatectomy. This instrument is a 47-item self-report instrument that incorporates the 27 FACT-G and 20-item anemic subscale. The 27-item FACT-G measures QoL in 4 life domains: physical (7 items), social (7 items), emotional (6 items), and functional (7 items). The additional 20 items relate to anemia due to loss of blood. The patients circle on a scale of 0 (not at all) to 4 (very much) how true was each statement. The scores were adjusted so that lower scores indicated higher QoL on all the items.
The European organization for Research and Treatment of Cancer (EORTC) core questionnaire used in this investigation has been described in a previous publication [12].
ETHICS
The study protocol was approved by the institutional review board (IRB), and all patients were provided with written informed consent. The study protocol and the patient care conforms to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008. Only patients who wished to be consented and followed for QoL were included in this study and not all pancreatic resections at our institutions were included during this time interval.
STATISTICS
Post-hoc analysis of a clinical trial was performed examining the safety of intraoperative autotransfusion during oncologic resection. Frequencies, as well as median and range or mean and SD, are used as descriptive statistics. All P values are based on 2-sided tests. The generalized linear models by using JMP V4.1 (SAS, Inc., Cary, NC, USA) were applied in order to analyze data. The repeated-measure design was used when different time points were involved in the analysis.
RESULTS
EORTC QLQ-C30 Questionnaire
Using EORTC QLQ-C30, increased severity of fatigue (P=0.032), pain (P=0.043), dyspnea (P=0.022), and loss of appetite (P=0.012) over baseline (pre-operative) were noted at initial follow-up; however, symptom scores normalized at 6 weeks follow-up, and remained stable at 6 months. A significant (P=0.022) decline in cognitive function vs. baseline was noted at 6 months follow-up after pancreatectomy. This was demonstrated to be predominantly related to the patients who had started and were undergoing adjuvant chemotherapy. Using a repeated-measures generalized linear model, neither age, nor complication occurrence, nor adjuvant therapy, nor early recurrence accounted for this cognitive decline (P>0.101). Moreover, no significant difference was noted in all EORTC QLQC30 QoL metrics between patients with or without major complications (P>0.113) at any time points (Figure 1).
FACT Questionnaire
The behavior or FACT anemia scores in patients undergoing pancreatectomy with and without anemia are shown in Figure 2a. In the anemic group the FACTphysical score (GP) showed a significant decrease in QoL at the first postoperative visit (P=0.023), with a return to baseline at 6 weeks and stability at 6 months when compared with the patients’ baseline QoL. For the anemic group, QoL was decreased compared to baseline at the first postoperative visit (P=0.038) and further declined at 6 weeks with a return to baseline at 3 months and improvement at 6 months (Figure 2b).
A high score in the FACT-social category (GS) denotes an increase in QoL parameters. For the anemic group, there was a decline in QoL at the 1st post operative visit, 6 weeks and 3 months with a return to baseline at 6 months. For the non-anemic group, at 1st post operative visit there was not an effect. However, there was a decline in QoL at 6 weeks, 3 months and a more dramatic (P=0.031) decrease at 6 months (Figure 2c). For FACT-emotional (GE), there was improvement in QoL for the anemic groups at 1st postoperative visit, 6 weeks, and 3 months with a slight decline at 6 months postoperative periods. However, the QoL at 6 months period was better than baseline. For the non-anemic group, there was little decline on the QoL at 1st postoperative visit, a significant decline at 6 weeks (P=0.027) but with a return to better QoL values at 3 and 6 months postoperative periods (Figure 2d).
For the FACT-function QoL effect (GF) , a high score denotes an increase in QoL parameters. Baseline values for QoL compared to first postoperative visit for the anemic group show a decline at both the 6 week and 3 months postoperative period, with a return to baseline at 6 months. For the non- anemic group, there was significant decline in QoL at the first postoperative visit, the 6 weeks, 3 months and 6 months follow-ups. (Figure 2e).
For FACT-additional (AN), in the anemic group, there was a significant decline in QoL at the 1st post operative visit with a return to baseline at 6 weeks and throughout the 6-month follow-up period. For the nonanemic group, there was a significant decline in QoL at 6 weeks post operative visit (P=0.023) with a return to baseline at 3 and improvement at 6 months (Figure 2f).
DISCUSSION
Despite the increasing number of pancreatectomies being performed, there is still the general impression that very little is known about the quality of life of a patient after this procedure [2]. Therefore, it is imperative to analyze the QoL changes reported by patients with pancreatic cancer undergoing pancreatectomy. Such findings may provide insight to adjuvant therapies still considered controversial in the treatment of pancreatic cancer.
In this prospective, longitudinal QoL study, we reported 34 pancreatic resection cases in our center. All patients completed this same survey preoperatively and then at four postoperative time points, allowing for measurement of changes in QoL over 6 months. Although other studies have reported QoL outcomes, this has been done in comparison with other procedures such as cholecystectomy [1, 5], gastric emptying [3, 4], or standard procedure versus pylorus-preserving procedures.
This report focuses on the QoL changes after pancreatic surgery. Eight major (grade ≥3) complications occurred in 7 patients; however, no significant difference was noted in QoL metrics between patients with or without complication. Increased severity of fatigue, pain, dyspnea, and loss of appetite compared to baseline was noted at initial follow-up; however, symptom scores normalized at 6 weeks follow-up, and remained stable at 6 months. A significant decline in cognitive function vs. baseline was noted at 6 months of follow-up after pancreatectomy; neither age, complication, adjuvant therapy, nor early recurrence explained this cognitive decline.
Although little has been published on QoL after pancreatectomy, some comparisons can be made between our report and those from the existing literature. Similar to most of the reports (Table 1), there is little change, or usually a return to a normal QoL, following pancreatectomy. In addition, this report demonstrated that symptoms scores remained stable at 6 months. This report compared with the report of Melvin et al. in their review of 45 pancreatectomy survivals showed some differences in regard to cognitive function. They used SF-36 to compare pylorus-preserving pancreatectomy and standard resection to a normal standard of age-matched control subjects from the U.S. population [1]. After analysis, they concluded that there were no differences in mental health between groups. In our study, using EORTC QLQ-30 with a postoperative time of 6 months, a significant decline in cognitive function vs. baseline was noted at 6 months follow-up after pancreatectomy. With the use of a repeated-measures generalized linear model, neither age, complication, adjuvant therapy, nor early recurrence explained this cognitive decline. This difference may have been because of the QoL instrument used, variables in the studies or most importantly the time point analyzed; in our case 6 months vs. 12 months for Melvin et al. [16]. Most importantly, the two studies analyzed different aspects in the QoL debate.
With pancreatectomy gaining acceptance and being increasingly performed in the treatment of pancreatic cancer, more consistent QoL surgical standards need to be established and more comparative studies need to be conducted. With pancreatectomy survivors in multimodality care and/on either adjuvant therapy or neoadjuvant therapy or both therapies, maximizing disease-free survival and/or overall survival limiting permanent QoL defects is imperative. Furthermore, minimizing the time for chemotherapy interruption is also important. This study, unlike the few other studies on pancreatectomy regarding QoL, shows the return to normalcy at 6 weeks and stability at 6 months. This could be helpful in determining the time to resume chemotherapy, thus accepting the concept of “time to resumption of chemotherapy” or “time to the induction of postoperative chemotherapy” as 8 weeks after pancreatic resection. This concept is important for collaborating as well as for educating other oncology specialties in the benefit as well as the limited QoL effect that pancreatic resection induces. Setting this time goal or, more importantly, this surgical standard in recovery is yet another potential quality measure that pancreaticoduodenal surgeons should consider as we proceed in overall patient outcome.
The limitation of this study is related to the small sample size of patients. A possibility exists that a larger sample size may create more variance in these results, but because of the close range of scores, this variance would probably be small. Even with this limitation, this study represents a solid foundation in which additional quality standards can be set as well as strived for in all pancreatic resection.
In conclusion, QoL metrics tend to normalize to preoperative levels after pancreatectomy. The occurrence of major complications does not predict a decrease QoL. The decrease in self-reported cognitive function at six months in this cohort merits further study.
Conflict of interest
The authors have no potential conflict of interest
References
- Huang JJ, Yeo CJ, Sohn TA et al.. Quality of life and outcomes after pancreaticoduodenectomy. Ann Surg 2000; 231: 890-898.
- Pezzilli R, Fantini L, Morselli-Labate AM. Pancreatectomy for pancreatic disease and quality of life. JOP. J Pancreas (Online) 2007; 8: 118-131.
- Patti MG, Pellegrini CA, Way LW. Gastric emptying and small bowel transit of solid food after pylorus-preserving pancreaticoduodenectomy. Arch Surg 1987; 122: 528-532.
- Fink AS, DeSouza LR, Mayer EA et al.. Long-term evaluation of pylorus preservation during pancreaticoduodenectomy. World J Surg 1988; 12: 663-670.
- McLeod RS, Taylor BR, O'Connor BI et al.. Quality of life, nutritional status, and gastrointestinal hormone profile following the Whipple procedure. Am J Surg 1995; 169: 179-185.
- Kokoska ER, Stapleton DR, Virgo KS et al.. Quality of life measurements do not support palliative pancreatic cancer treatments. Int J Oncol 1998; 13: 1323-1329.
- Schniewind B, Bestmann B, Henne-Bruns D et al.. Quality of life after pancreaticoduodenectomy for ductal adenocarcinoma of the pancreatic head. Br J Surg 2006; 93: 1099-1107.
- Pezzilli R, MorselliLabate AM, Fantini L et al.. Quality of life and clinical indicators for chronic pancreatitis patients in a 2-year follow-up study. Pancreas 2007; 34: 191-196.
- Schmier J, Elixhauser A, Halpern MT. Health-related quality of life evaluations of gastric and pancreatic cancer. Hepatogastroenterology 1999; 46: 1998-2004.
- Martin RC, Scoggins CR, Egnatashvili V et al.. Arterial and venous resection for pancreatic adenocarcinoma: operative and longterm outcomes. Arch.Surg. 2009; 144: 154-159.
- Martin RC, Scoggins CR, McMasters KM. A phase II study of radiofrequency ablation of unresectable metastatic colorectal cancer with hepatic arterial infusion pump chemotherapy. J Surg Oncol 2006; 93: 387-393.
- Bower MR, Ellis SF, Scoggins CR et al.. Phase II comparison study of intraoperative autotransfusion for major oncologic procedures. Ann Surg Oncol 2011; 18: 166-173.
- Martin RC, Eid S, Scoggins CR, McMasters KM. Health-related quality of life: return to baseline after major and minor liver resection. Surgery 2007; 142: 676-684.
- Eid S, Stromberg AJ, Ames S et al.. Assessment of symptom experience in patients undergoing hepatic resection or ablation. Cancer 2006; 107: 2715-2722.
- Heffernan N, Cella D, Webster K et al. Measuring health-related quality of life in patients with hepatobiliary cancers: the functional assessment of cancer therapy-hepatobiliary questionnaire. J Clin Oncol 2002; 20: 2229-2239.
- Melvin WS, Buekers KS, Muscarella P et al.. Outcome analysis of long-term survivors following pancreaticoduodenectomy. J Gastrointest Surg 1998; 2: 72-78.

