Kevin Varghese1, Nita Hubert2*, Kevin Saji Thomas1, Sara Ammu Chacko3 and Laly Jose1
1Dr. SMCSI Medical College, Karakonam, Kerala, India
2Department of Radiodiagnosis, Dr. S.M.C.S.I Medical College, Karakonam, India
3Gokulam Medical College, Trivandrum, India
Corresponding Author:
Nita Hubert
Department of Radiodiagnosis
Dr. S.M.C.S.I Medical College, Karakonam
Trivandrum District, Kerala, India
Tel: +919495280041
E-mail: nitasundar@yahoo.com
Received date: August 09, 2017; Accepted date: September 09, 2017; Published date: September 16, 2017
Citation: Varghese K, Hubert N, Thomas KS, Chacko SA, Jose L (2017) Improvement in Venous Clinical Severity Score Following Ultrasound Guided Foam Sclerotherapy. J Imaging Interv Radiol.1 No.1:2
Introduction
Varicose veins are abnormally dilated tortuous superficial veins caused by incompetent venous valves. The reasons why patients seek treatment for varicose veins are pain, itching, heaviness, swelling, cramps, spontaneous bleeding, ulceration & cosmetic [1]. In 2000, American venous forum developed the venous clinical severity score which was an improvement over the original CEAP scoring system. In 2010, revised VCSS was published and is currently used for documenting and evaluating the progression of CVD [2].
In the various treatment modalities for varicose veins like superficial venous surgery, endovascular laser ablation, sclerotherapy & radiofrequency ablation, surgery has been and is still the standard [3]. Sclerotherapy is gaining popularity as it is relatively a simple and effective procedure with minimal post procedural complications and a short recovery time [4]. Patient compliance is excellent and the financial burden on the patient is also very less compared to surgical modality of treatment. Sclerotherapy is injecting a sclerosant into the lumen of a varicose vein [1]. Foam sclerotherapy is the method by which foam is created by mixing air with the sclerosant and is then injected into the vein. Three major categories of sclerosants are hyperosmolar agents, detergents and chemical sclerosants [5].
a. Detergent sclerosants – include polidocanol, sodium tetradecylsulphate (STDS) and sodium morrhuate. They alter the surface tension around the endothelial cell, resulting in rapid over hydration. This causes endothelial damage. Most common among these are STDS and polidocanol.
b. Osmotic agents – include hypertonic saline. Endothelial damage is by dehydration of the endothelial cell.
c. Chemical irritants – include chromate glycerine and polyiodinated iodine. They act as corrosives and result in endothelial damage.
UGFS is a novel further development of traditional sclerotherapy. UGFS is a variant of liquid sclerotherapy wherein the liquidair mixture is injected into the varicose vein under ultrasound guidance, and is much more effective compared to liquid sclerotherapy [6,7]. Ultrasound guided foam sclerotherapy has become a popular non-surgical method of treating varicose veins because of its numerous advantages [8,9] like minimally invasive procedure, better patient compliance and very less adverse effect etc. In 2000, Tessari proposed forming the foam with 2 syringes connected by a three way stop cock. This method is widely accepted nowadays and is known as the Tessari’s method [1,10].
Very few similar studies are available in our country as per our knowledge, regarding the clinical effectiveness of ultrasound guided foam sclerotherapy [11].
Methodology
Study design and setting
An observational, prospective study was done in the Department of Radio diagnosis at Dr. Somervell memorial, C.S.I Medical College from December 2014 to November 2016. The study population belonged to a rural population in South Kerala.
Procedure
All patients referred for UGFS were clinically assessed using VCSS and Duplex Doppler was done to assess the site of reflux and involvement of the long saphenous or short saphenous system. UGFS was done in the Department of Radiodiagnosis after getting an informed written consent. A good peripheral IV access was secured with a 18/20G canula and continuous monitoring of vital parameters was done during the procedure. UGFS was done using sodium tetradecyl sulphate as sclerosant and foam was produced by mixing sclerosant and air in the ratio 1:1 by Tessari’s method. 4 ml sclerosant was mixed with 4ml air using two syringes connected by a three way stop cock for at least 20 times until stable foam is formed. Under ultrasound guidance a 23G cannula was positioned into the dilated vein selected for injection and the prepared foam sclerosant is injected. The distribution of the foam and the resultant vasospasm of the vessel were monitored by ultrasound. While injecting the sclerosant, the saphenofemoral or saphenopopliteal junction and major perforators near the site of injection are blocked manually, by an assistant. After the injection, the leg is elevated and compression bandage applied from the foot to the thigh. Following the procedure patient was kept under observation in the out-patient and encouraged to maintain moderate activity, like walking and good hydration. Patients were advised to wear elastocrepe bandage continuously for 2 weeks. Analgesics were prescribed as and when they were required. Follow up Duplex Doppler was advised at 1 week to evaluate associated complications and to assess venous occlusion. Patient came for review at 2 months to assess the efficacy of the procedure by Duplex Doppler and to assess the clinical improvement by post procedure VCSS.
Outcome
58 patients underwent UGFS, during the study period. However, only 49 patients came for follow up at 2 months, for evaluation of the outcome of the procedure by Duplex Doppler study and for clinical assessment by VCSS. Outcomes were based on the duplex Doppler findings of superficial venous occlusion and presence of reflux.
Successful outcome is defined as complete occlusion of the dilated superficial veins with no reflux at the junction or partial occlusion of dilated superficial veins without reflux. Failure is defined as partial occlusion of dilated superficial veins with persistent reflux or no occlusion of dilated superficial veins.
Ethical consideration
Approval was sought and obtained from the Ethics Committee of the Dr. S.M.C.S.I Medical College, Kerala University of Health Sciences, Kerala, India.
Informed written consent in their mother tongue was obtained from all participants for the procedure and for participation in the study. The risks and limitations of using STDS injection in the form of foam under guidance were explained in detail. Patients were identified on the basis of their record number and serial number, thus maintaining the personal details confidential.
Results and statistical analysis
44 (89.8%) out of the 49 cases followed up at 2months with duplex Doppler showed complete occlusion (75.5%) or partial occlusion with no reflux (14.3%) and 5 cases showed partial occlusion with persistent reflux (10.2%). No cases were seen where there was no occlusion (Table 1 and Figures 1 and 2).
| Duplex Doppler Follow up at 2 months |
Number (49) |
Percentage % |
| *Complete occlusion |
37 |
75.5 |
| *Partial occlusion without reflux |
7 |
14.3 |
| **Partial occlusion with reflux |
5 |
10.2 |
| **No occlusion |
0 |
0 |
Table 1: Effectiveness of UGFS at 2 months follow up duplex Doppler.
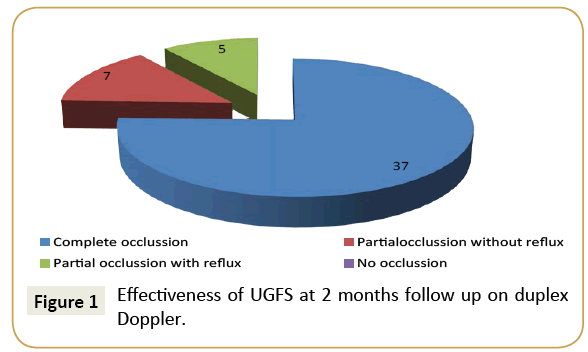
Figure 1: Effectiveness of UGFS at 2 months follow up on duplex Doppler.
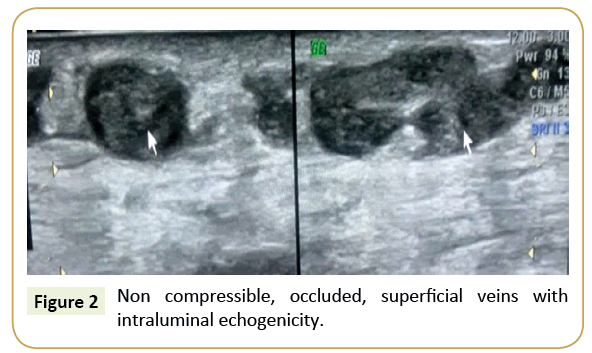
Figure 2: Non compressible, occluded, superficial veins with intraluminal echogenicity.
Persistent reflux even when associated with partial thrombosis of the superficial veins was considered a failed procedure (Table 2). However, even those 5 patients with persistent reflux and thus an unfavourable outcome, showed clinical improvement as determined by VCSS score.
| Outcome |
Number (49) |
Percentage % |
| *Success |
44 |
89.8 |
| **Failure |
5 |
10.2 |
Table 2: Outcome of UGFS at 2months assessed by duplex Doppler.
Out of the 19 patients who had venous ulcer, 17 of them (89%) showed healing of the ulcer (decrease in size or severity), at 2months post procedure. However, in 2 patients who had relatively large ulcers, even though there was partial healing persistence of ulcer was observed with no significant improvement in VCSS.
In this study, out of the successful 44 patients, all of them had a VCSS improvement by about 3 to 5 points.
In the study population, pre-procedure VCSS score ranged between 19 and 3 with a mean value of 10.7. Post procedure VCSS score ranged between 16 and 2 with a mean value of 7.6 This 3.1 decrease in post UGFS VCSS, with a t value of 11.08, was found to be statistically significant. Distribution of data showing improvement in VCSS following UGFS is displayed on the box plot.
Discussion
Ultrasound guided foam sclerotherapy is a simple, minimally invasive, cost effective, out-patient procedure which significantly decreases morbidity by improving the clinical condition as assessed by VCSS. Pre UGFS VCSS ranged between 3 and 19 with a mean of 10.5. 2 months following UGFS, there was a decrease in mean VCSS to 7.6, with a range between 2 and 16. The 3.1 decrease in post UGFS mean VCSS was statistically significant (P=0.01). A study by Asser et al showed significant improvement of VCSS 2 weeks following the UGFS in comparison to pre intervention VCSS, where P value was <0.0001. Also, there was significant improvement of VCSS 6 months following the UGFS in comparison to pre intervention VCSS, where P value was <0.000111.
Figueiredo et al. found a decrease in pain, oedema and inflammation with improvement in VCSS following treatment [12]. Significant improvement was also documented in our patients with no ulcer and who had low VCSS prior to UGFS. Improvement in VCSS by 3-5 was noted in 44 of the 49 patients who had good outcome of the procedure, as assessed by occlusion of the superficial veins with absence of reflux. 5 patients who had occlusion of superficial veins, but with persistent reflux were considered failed outcomes also had improvement in VCSS at 2 month follow up.
Ulcer healing is another important and clinically significant feature seen following UGFS. 17 of the 19 patients with ulcer prior to UGFS had completed healing at 2 months. 2 patients with very large ulcers had persistent ulcer during their 2 month follow up. According to Cerrati, significant ulcer healing was noted following UGFS (13 chronic venous ulcers) within two weeks; in 13 chronic venous ulcers, two ulcers healed and significant improvement was observed in the dimensions of eleven ulcers. UGFS produces excellent results in the treatment of chronic venous ulcers [1]. The authors have concluded that patients with severe venous insufficiency present a rapid response to ultrasound-guided foam sclerotherapy [1]. Another study of 27 cases of chronic venous ulcers that were treated with UGFS, showed that at 1 month follow-up 79% of the ulcers were completely healed and at six months follow up 96% of the ulcers were completely healed [1]. These results are similar to our study, where there was 89% healing of the ulcers at 2 month follow up.
Limitations
Out of the 58 patients enrolled in the study only 49 patients came for follow up at 2 months following UGFS. Patient compliance regarding use of bandage immediately following UGFS were not documented and considered in evaluation of outcome of UGFS. Associated co morbidities including peripheral vascular disease, diabetes, hypertension were not taken into consideration. Long term follow up was also beyond the scope of this study. Further studies with larger populations followed up over a longer period would be ideal to assess long term efficacy and recurrence.
Conclusion
In conclusion UGFS is a simple, cost-effective procedure, in the treatment of both great saphenous and short saphenous varicose veins. It is a relatively safe technique with very few complications and good efficacy, in the treatment of primary varicose veins and recurrent varicose veins. Ulcer healing and improvement in VCSS is noted as early as 2 months following UGFS [11].
Acknowledgement
Competing interests
The authors declare that they have no financial or personal relationships which may have inappropriately influenced them in writing this article.
Authors’ contributions
K. Varghese was the project leader and N. Hubert was responsible for the project design and procedure; K. Thomas was involved in doing the procedure with the project leader, S.A. Chacko was responsible for organizing the study, its conduct and sourcing of patients and L. Jose also contributed to the procedure.
References
- Ceratti S (2011) Ultrasound-guided foam sclerotherapy in the treatment of chronic venous insufficiency. Radiol Bras 44: 167-171.
- Vasquez MA, Wang J, Mahathanaruk M, Buczkowski G, Sprehe E, et al (2007) The utility of the venous clinical severity score in 682 limbs treated by radiofrequency saphenous vein ablation. J Vasc Surg 45: 1008-1014.
- O’Hare JL, Earnshaw JJ (2007) The use of foam sclerotherapy for varicose veins: A survey of the members of the Vascular Society of Great Britain and Ireland. Eur J Vasc Endovasc Surg 34 : 232-235.
- Kanwar A, Hansrani M, Lees T, Stansby G (2010) Trends in varicose vein therapy in England: Radical changes in the last decade. Ann R Coll Surg Engl 92: 341-346.
- Edwards GA, Baynham S, Lees T, Mitchell DC (2009) Management of varicose veins: A survey of current practice by members of the Vascular Society of Great Britain and Ireland. Ann R Coll Surg Engl 91: 77-80.
- Rabe E, Otto J, Schliephake D, Pannier F (2007) Efficacy and safety of great saphenous vein sclerotherapy using standardisedpolidocanol foam (ESAF): A randomised controlled multicentre clinical trial. Eur J Vasc Endovasc Surg 2: 238-245
- Yamaki T, Nozaki M, Iwasaka S (2004) Comparative study of duplex guided foam sclerotherapy and duplex guided liquid sclerotherapy for the treatment of superficial venous insufficiency. DermatolSurg 30: 718-22.
- Chapman-Smith P, Browne A (2009) Prospective five-year study of ultrasound-guided foam sclerotherapy in the treatment of great saphenous vein reflux. Phlebology 24: 183-188.
- Dietzek CL (2007) Sclerotherapy: Introduction to solutions and techniques. Perspect Vasc Surg Endovasc Ther 19: 317-324.
- Takashi Yamaki (2010) Compression sclerotherapy for primary valvular insufficiency. Ann Vasc Dis 3: 37-45.
- Asser AG, Saad RG (2013) Ultrasonic guided foam sclerotherapy for varicose vein. Egypt J Surg 32: 12-19.
- Figueiredo M, Araujo S, Barros Jr N, Miranda Jr F (2009) Results of surgical treatment compared with ultrasound-guided foam sclerotherapy in patients with varicose veins: A prospective randomised study. Eur J Vasc Endovasc Surg 38: 758-763.
