Obioma A1* and Chikanka AT2
1Faculty of Science, Department of Medical Laboratory Science, Rivers State University of Science and Technology, Nkpolu, Orowhorukwo Port Harcourt, Nigeria
2Department of Medical Microbiology, River State University of Port Harcourt, Nkpolu, Orowhorukwo, Nigeria
*Corresponding Author:
Dr. Azuonwu Obioma
Faculty of Science, Department of Medical Laboratory Science
Rivers State University of Science and Technology
Nkpolu, Orowhorukwo Port Harcourt, Nigeria
Tel: 234 803551968
E-mail: bimajacobs@yahoo.co.uk
Received Date: May 01, 2018 Accepted Date: May 31, 2018 Published Date: June 04, 2018
Citation: Obioma A, Chikanka AT (2018) Influence of Confounding Evidence Based Risk Factors Triggering the Incidence of HIV Antibodies among Screened Population of Niger Delta Extraction. Insights Biomed. Vol.3 No.2:11 doi: 10.21767/2572-5610.100046
Keywords
Human Immunodeficiency Virus (HIV); HIV transmission; Genital mutilation; Heterosexuality
Introduction
The Human Immunodeficiency Virus is a RNA retrovirus whose long term infection leads to AIDS (Acquired Immune Deficiency Syndrome). In Nigeria, two cases of AIDS resulting from HIV was first diagnosed in 1985 but reported in 1986; a female sex worker was among the two cases [1]. When it first emerged, it was perceived by some as “American Idea for Discouraging Sex” [2]. In recent times, surveillance on HIV prevalence has become eminent since epidemiological data available shows that HIV is still a public health concern which has led to the loss of about 25 million lives within the past 30 years [3]. Sub-Saharan Africa accounted for about 67.6% of the worldwide HIV prevalence in 2009 while 25.8 million persons were estimated to be living with HIV in the same region as at the end of 2014 [4]. Of these, 9% are based in Nigeria [5]. South Africa with 3 million infected persons ranks first in the continent with Nigeria being second in HIV prevalence in Africa [6].
Nevertheless, in 2005, its prevalence among women, youths and children was 4.4% in Nigeria while in 2012, the prevalence of HIV/AIDS in Nigeria was recorded to be between 4.1 and 6.0%. In 2014, a total number of 220,000 new cases were reported. Previous studies have however shown that most children who were infected with the virus got it from their mothers from birth [7]. Regardless of the presence of antiretroviral therapy, Nigeria with 3.2 million infected persons has been tagged second among nations with the HIV infection after South Africa which has an estimated 6.8 million infected persons [5,6]. Furthermore, practices such as female genital mutilation, multiple sex partners, traditional birth marks, tattooing and child delivery by unskilled traditional birth attendants are some of the confounding risk factors and practices that have led to increased HIV prevalence in Nigeria [8]. Having multiple sex partners has however, be found to be a major means of transmission of the virus as it accounts for 80% of cases; same sex intercourse and intravenous drug use are however beginning to be of public health concern globally [9]. As well known, AIDS resulting from HIV has no cure; however, with the help of antiretroviral drugs and the patient keeping away from critical risk factors, it can be managed to large extent [10].
Although there is increased awareness on HIV/AIDS, only about 28% and 20% of men and women respectively say they can buy vegetables from an individual who is living with AIDS [11]. This is because most persons believe HIV/AIDS can be acquired though the consumption of food items from an infected person and the belief that since HIV/AIDS is transmitted through blood, the food vendor may introduce his/her blood into the food and as such infect others. As Awofala and Ogundele noted, there is a good number of persons living with the HIV, yet the recorded prevalence is low [12]. It is therefore important that regular studies be carried out by relevant agencies on the prevalence of HIV in communities and states in Niger Delta, as this will help in knowing how far the fight against the virus has gone especially in our remote villages. It is for this reason that this study was carried out to determine the prevalence of the virus in some oil rich communities of Niger Delta. Nevertheless, it is therefore strongly expected that the epidemiological data generated from this study, would succinctly re-direct government policies towards an effective management strategy of this social scourge, especially among the weak and poor in the remote villages where access to functional health care facilities and availability of the antiretroviral drugs remains a massive critical challenge to handle [13-15].
Research Methodology
Sample area
Subjects for this study were drawn from seven (7) locations within Ahoada East Local Government Area of Rivers State located in the Niger Delta region of Nigeria. This area is one of the 23 Local government areas in the state and is made up of predominantly farmers, fishermen and traders. A few are civil servants who also indulge in subsistence farming. It is surrounded by Omoku, Rumuekpe, Ahoada West, Obagi, Elele, Obricom and Erema communities which are host communities to oil exploration and as such has a large presence of persons seeking for greener pastures in the oil and gas sector. The locations used include the Community Health Center Edeogha-Ekpeye (Location 1), Community Health center Ochigba (Location 2), Comprehensive Health Center Ahoada (Location 3) and Ahoada General hospital (Location 7). Samples were also collected from three (3) communities which are non-hospital/clinic-based collection centers namely Ula-upata (Location 4), Ahoada Timber Market (Location 5) and Ogbo town (Location 6). The age of the subjects was ≥15 and included both males and females (Figure 1).
Figure 1: Map of Rivers State (Blue spot indicates the study location).
Sample collection/Experimental procedure
Blood samples of the subjects were collected using sterile 2 ml syringe, immediately transferred to a serum bottle and allowed to clot. The collected samples were centrifuged at 2000 rpm for 5 minutes and sera recovered and stored at -20°C till they were needed. Screening for HIV1 and HIV2 was done using a double enzyme-linked immunosorbent assay (ELISA) method made up the Determine (Abbott Laboratories, Japan), and Stat-Pak HIV1 and HIV2 kits (Chembio Diagnostics, USA). The Determine HIV1 and HIV2 kits are used in vitro to qualitatively detect HIV type 1 and 2 antibodies in human serum while the Stat-Pak HIV1 and HIV2 kits is often used as a confirmatory test for the HIV. The Stat-Pak kit is based on immune chromatography and involves the combination of a specific antibody binding protein joined to a colloidal gold dye particle and HIV1 and HIV2 antigens bound to the membrane phase which is solid. In this study, all sero-positive samples were re-screened for the Subtype (1 and 2) using the SD Bioline HIV1 and HIV2 kits (Standard Diagnostics, Korea). The screening process was however done according to manufacturers’ instructions. Results were presented using charts.
Data analysis
The data obtained were analyzed using Microsoft Excel package 2010, and results were presented in charts with error bars as shown below.
Results
Analysis of HIV1 and HIV1 and HIV2 seropositive persons in randomly selected 1000 respondents in Ahoada East Local Government Area of River State recorded a 10.7% prevalence rate as 107 persons tested positive to the HIV antibody. Of these, 7.8% were HIV1 positive while 2.9% were HIV1 and HIV2 positives. Females made up 53.6% of the study population while males made up 46.4%. 47.4% and 52.6% were HIV1 positive among the males and females respectively while 41.4% and 58.6% were both HIV1 and HIV2 positives among the males and females respectively (Figure 2). Persons within ages 25-34 had the highest prevalence for HIV1 (44.9%); 15-24 had 34.6%, 35- 44 had 20.5 and 45-54 had none. Ages 45-54 had the highest prevalence of HIV1 and HIV2 cases (51.7%) while ages 15-24 and 25-34 had none as seen in Figure 3. Farmers made up a higher percentage of those with HIV1 and HIV2 while students made up a higher percentage of those with HIV1 as presented in Figure 4. Those with only First School Leaving Certificate (FSLC) constituted a major part of those with HIV1 while those with the Senior School Certificate (SSCE) made up a huge part of those with HIV1 and HIV2 as seen in Figure 5. Singles made up 67.9% of those who were HIV1 positive while married persons made up 55.2% of those positive for HIV1 and HIV2 (Figure 6). The majority of the positive subjects admitted to knowing that condoms could help prevent the transmission of HIV. Location 7 had the highest percentage occurrence of both HIV1 and HIV1 and HIV2 (Figures 7 and 8).
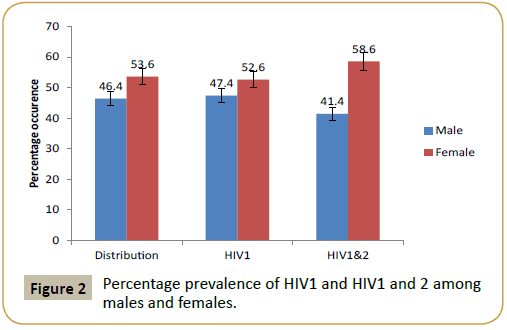
Figure 2: Percentage prevalence of HIV1 and HIV1 and 2 among males and females.
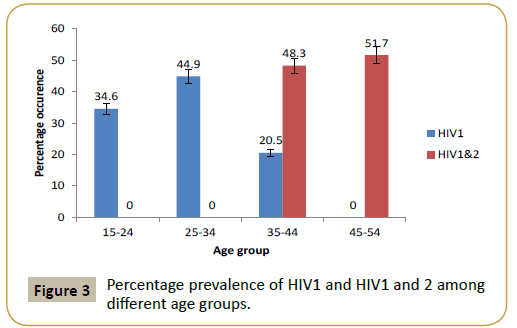
Figure 3: Percentage prevalence of HIV1 and HIV1 and 2 among different age groups.
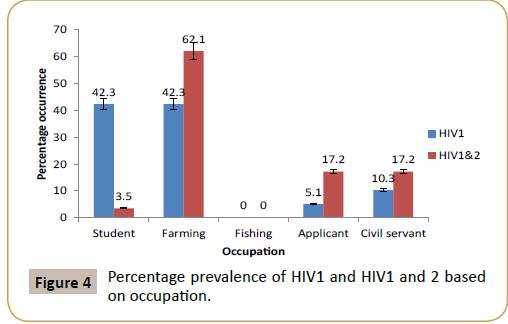
Figure 4: Percentage prevalence of HIV1 and HIV1 and 2 based on occupation.
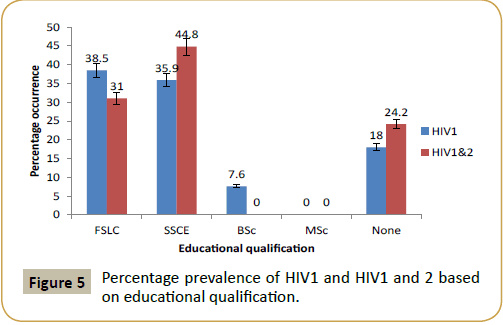
Figure 5: Percentage prevalence of HIV1 and HIV1 and 2 based on educational qualification.
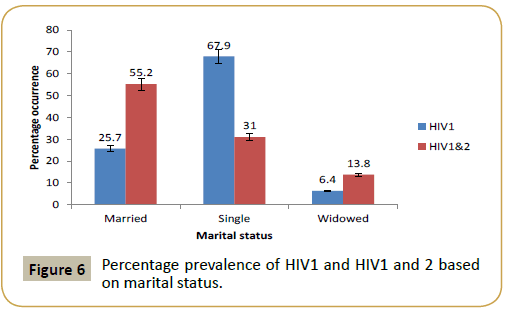
Figure 6: Percentage prevalence of HIV1 and HIV1 and 2 based on marital status.
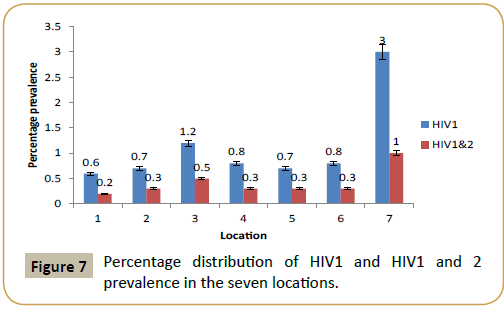
Figure 7: Percentage distribution of HIV1 and HIV1 and 2 prevalence in the seven locations.
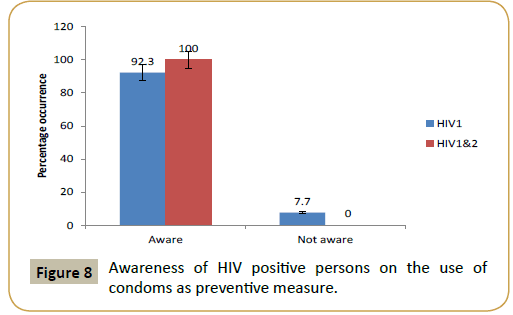
Figure 8: Awareness of HIV positive persons on the use of condoms as preventive measure.
Discussion
The study was carried out among indigenes of Ahoada East Local Government Area of Rivers State and recorded a total prevalence of 10.7%. Females accounted for 52.6% and 58.6% of the total HIV 1 and 2 prevalence, respectively. This increase in prevalence in females has been reported by NACA and Azuonwu et al. [13-15]. Also, in another study carried out by Akinjogunla and Adegokein Uyo, Nigeria, they recorded a higher prevalence among females compared with that of males [16]. This increase in female prevalence has been linked to poverty, harmful traditional rites, political and legal factors, girl child marriage, disabilities and gender-based violence [14]. Also, according to Azuonwu et al. [15], sexual promiscuity, rape and prostitution are some risk factors that may have led to the increased prevalence among females. The possibility of them contacting the disease from needles and blades used on their hair and nails from the saloon, manicure and pedicure shops is not inevitable, as safety and personal hygiene policies of the study location remains weak till date. From the results also, HIV 1 and 2 prevalence were higher than that of HIV 1 which means there was a coinfection and these persons may have contacted both serotypes from two sources without prior knowledge. Okerentugba et al. however recorded a prevalence of 67% and 33% for HIV 1 and 2 serotypes respectively among pregnant women in a hospital in Port Harcourt [17].
The prevalence among the different age groups differed even based on the serotypes. Ages 25-34 had a higher HIV 1 (44.9%) while ages 45-54 had a higher HIV 2 prevalence (51.7%). Although there is paucity of prevalence of the different HIV serotypes based on age, ages 25-34 are usually implicated in high HIV prevalence. Azuonwu et al. [15] recorded a higher HIV prevalence among persons between ages 22-28 in a study carried out in a Niger Delta community. Also, in another study carried out in a community in Rivers State, persons within ages 21-26 had the highest prevalence [13]. Idleness is also a factor as most youths who do not have jobs fall back to risky activities such as intravenous drug use as well as they may be victim of rape when they are probably under the influence of hard drugs. More often, this age group is seen as the age when there is high sexual demand and also sharing of sharp objects such as needles, blades and clippers which are all risk factors for HIV transmission.
Nonetheless, farmers recorded a higher HIV 1 and 2 prevalence (62.1%) while students and farmers recorded same HIV 1 prevalence (42.3%). The distance of the farms from dwelling places may have probably provided a room for the farmers to be involved in sexual promiscuity, as well as increase the incidence of rape. Students may have involved themselves in after school or even within school hour’s activities such as intravenous drug use and illicit sex behaviors. The desire to be like their peers who have been involved in these may have driven them to be involved in these activities.
More often, singles out of desperation and financial benefits also get involved in activities that predispose them to HIV. These may have been responsible for the increased HIV 1 prevalence in singles than the other two groups. Some persons even when married may be unfaithful to their spouses and end up being sexually promiscuous. On the other hand, these persons whether married, single or widowed may have been exposed to this virus because of the nature of their job (e.g. health personnel) especially in a weak health system that lack personal protective equipment and absolute barrier nursing is not practice enhancing the safety of staff.
It is worthy of note that persons with the highest educational qualification in this study (MSc) recorded no prevalence while those with BSc recorded the least prevalence of 7.6%. The highest prevalence was recorded among those with the Senior School Certificate (SSCE). Education within the four walls of a university may have thus played a huge role in reducing the occurrence of HIV among them. More often, they have knowledge of the use of condoms as a means of preventing the spread of HIV. On the other hand, persons with no education had a lower prevalence than those with FSLC and SSCE. This may be attributed to home training as in most homes, informal education is carried out and members of the home are advised to keep off from immoral behaviors. Location 7 accounted for a major percentage of the total prevalence of both HIV 1 and HIV 1 and 2 co-infection. This location is the Ahoada General Hospital and is usually busy as most persons visit the hospital often with complicated illnesses, thus this may probably be the reason for an increased prevalence rate.
The awareness on the use of condoms for the prevention of the HIV was very high as majority of the subjects admitted to knowing that condoms could prevent the spread of the virus. The issue is however not in knowledge but in the practice of that which is known. One could however say if a good number of the subjects knew condoms could prevent the spread of the virus and yet they contacted the virus; they may have contacted it through other means such as the sharing of sharp objects, rape or mother to child transmission.
Conclusion
In this study carried out, the HIV prevalence was 10.7% with 2.9% testing positive to both HIV 1 and 2 and 7.8% testing positive to HIV 1 and 2. Majority of the HIV positive subjects were HIV 1 and 2 positives. Some of the reasons pointed at for the presence of this virus were sexual promiscuity, sharing of sharp objects, child marriage, rape, heterosexuality, homosexuality, poverty, violence on a particular gender, disabilities and traditional rites that are harmful especially to females.
Recommendations
Continuous and frequent surveillance should be carried out especially in rural areas where little or no attention is given to individual’s health outcome. Individuals should be encouraged to visit a health facility to know their HIV status whether or not they feel ill as the virus may be latent and asymptomatic for a long period of time. Employment opportunities should be provided so as to prevent youths from indulging in illicit activities due to idleness.
Acknowledgments
We are sincerely grateful to all the subjects who willingly participated in the study. We are also thankful to Dr. Azuonwu, Goodluck, Dr. (Mrs) G.N. Wokem and all the laboratory staff where the assay was done for all their technical support.
Conflict of Interest
None noticed among authors.
References
- Nasidi A, Harry TO (2006) The epidemiology of HIV/AIDS in Nigeria. In: Adeyi O, Kanki PJ, Odutolu O, Idoko JA (Eds.), AIDS in Nigeria: A nation on the threshold. Harvard Center for Population and Development Studies, Cambridge, Massachusetts, UK.
- https://theses.gla.ac.uk/ 642/1/2009EzePhD.pdf
- https://www.who.int/hiv/pub/progressreports/update2014/en/
- https://www.usaid.gov/what-we-do/global-health/hiv-and-aids/technical-areas/orphans-and-vulnerable-children-affected-HIV
- https://naca.gov.ng/wordpress/wp-content/uploads/2016/11/NARHS-Plus-2012-Final-18112013.pdf
- https://www.medbox.org/ng-studies-reports/nigeria-national-hiv-aids-and-reproductive-health-survey-2012-narhs-plus/preview
- https://www.unaids.org/en/dataanalysis/knowyourre
- Nigeria National Agency for the Control of AIDS (2014) Global AIDS Response Country Progress Report, Nigeria.
- Nigeria National Agency for the Control of AIDS (2010) United Nations General Assembly Special Session (UNGASS) Country Progress Report, Nigeria.
- Azuonwu O, Erhabor O, Obire O (2012) HIV among military personnel in the Niger Delta of Nigeria. J Comm Health 37: 25-31.
- https://www.unicef.org/wcaro/english/WCARO_Nigeria_Factsheets_HIV-AIDS.pdf
- Awofala AA, Ogundele O (2016) HIV epidemiology in Nigeria. Saudi J Biol Sci 25: 697-703.
- Azuonwu O, Ihua A, Wokem GH, Igwe C (2017) Prevalence of Human Immunodeficiency Virus (HIV) Antibody among Subjects in Ogba/Egbema/Ndoni Local Government Area (LGA) of Rivers State of Nigeria. Translat Biomed 8: 118.
- Nigeria National Agency for the Control of AIDS (2015) Global AIDS Response Country Progress Report, Nigeria.
- Azuonwu O, Azuonwu TC, Akpelu G (2017) Evaluation of cofounding HIV sero-prevalence and associated risk factors among subjects in some upland communities of Niger delta, Nigeria. Int J Public Health Safety 2: 4
- Akinjogunla OJ, Adegoke AA (2009) Sero-prevalence of human immunodeficiency virus (HIV) 1 and 2 infections in Uyo metropolis, Akwa Ibom State. Scient Res Essay 4: 1381-1384.
- Okerentugba PO, Uchendu SC, Okonko IO (2015) Prevalence of HIV among Pregnant Women in Rumubiakani, Port Harcourt, Nigeria. Public Health Res 5: 58-65.

