Akira Hokama*, Kiyoshi Maeda, Ryosaku Tomiyama, Tetsuo Hirata, Fukunori Kinjo, Atsushi Saito
First Department of Internal Medicine, University of the Ryukyus. Okinawa, Japan
- *Corresponding Author:
- Akira Hokama,
First Department of Internal Medicine
University of the Ryukyus 207 Uehara,
Nishihara Okinawa 903-0215,
Japan,
Phone +81-98.895.1144
Fax +81-98.895.1414
E-mail hokama-a@med.u-ryukyu.ac.jp
Received: 24 May 2004 Accepted: 8 June 2004
Keywords
Case Reports; Diagnostic Imaging; Pancreatic Pseudocyst; Pancreatitis, Alcoholic; Splenic Diseases
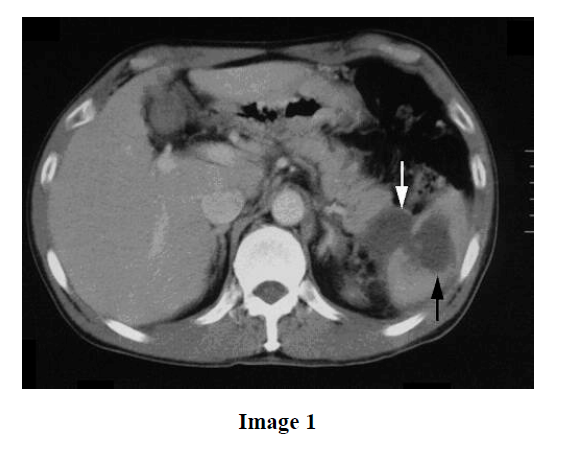
A 48-year-old man presented with severe left flank pain. He had been a known alcoholic for 20 years. On physical examination, he was afebrile and normotensive. Laboratory values were as follows: leukocytes, 14,700/mm3 (reference values: 3,900-9,800/mm3); lactate dehydrogenase, 190 IU/L (reference values: 120-230 IU/L); amylase, 89 IU/L (reference values: 40-123 IU/L); and C-reactive protein, 7.9 mg/dL (reference values: 0-0.27 mg/dL). A contrast-enhanced CT scan (Image 1) demonstrated pseudocysts of the pancreatic tail extending into the splenic hilum (white arrow) and splenic parenchyma (black arrow). Intrasplenic pancreatic pseudocysts associated with chronic alcoholic pancreatitis were diagnosed. His symptoms and laboratory values improved with conservative treatment including the intravenous administration of antibiotics. Follow-up imaging studies showed that the pseudocyst extension was markedly reduced. The patient remains asymptomatic.
As the pancreas and the spleen are located in close proximity, splenic complications may occur in the course of acute and chronic pancreatitis [1]. Although very rare (2%), splenic involvement of the pancreatitis includes splenic vascular injury, intrasplenic pseudocysts, abscess, hematoma, infarction, necrosis, and rupture [2, 3]. Among the above, intrasplenic pseudocysts are the most frequent. The most consistent symptom is abdominal pain in the upper left quadrant. Amylase levels may be normal in some cases [1]. These complications may be lifethreatening; therefore, patients should be closely monitored with imaging studies. Most cases can be managed conservatively; however, surgical interventions, such as splenectomy, distal pancreatectomy and percutaneous drainage, are indicated mainly as a result of clinical findings in order to avoid aggressive outcomes [3].
In conclusion, patients with the risk of chronic pancreatitis should be monitored for splenic complications.
References
- Lankisch PG. The spleen in inflammatory pancreatic disease. Gastroenterology 1990; 98:509-16. [PMID 2403954]
- Malka D, Hammel P, Levy P, Sauvanet A, Ruszniewski P, Belghiti J, Bernades P. Splenic complications in chronic pancreatitis: prevalence and risk factors in a medical-surgical series of 500 patients. Br J Surg 1998; 85:1645-9. [PMID 9876067]
- Fishman EK, Soyer P, Bliss DF, Bluemke DA, Devine N. Splenic involvement in pancreatitis: spectrum of CT findings. AJR Am J Roentgenol 1995; 164:631-5. [PMID 7863884]

