Muhammad Wasif Saif
Columbia University, College of Physicians and Surgeons and the Herbert Irving Cancer Center. New York, NY, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Columbia University; College of Physicians and Surgeons and the
Herbert Irving Cancer Center; 177 Fort Washington Avenue, Suite
6-435; New York, NY 10032; USA
Phone: +1-212.305.4954
Fax: +1-212.3050.3035
E-mail: mws2138@columbia.edu
Received November 16th, 2010 - Accepted November 18th, 2010
Keywords
Adenocarcinoma; Hepatectomy; Neoplasm Metastasis; Pancreatic Neoplasms; Pancreaticoduodenectomy
Dear Sir,
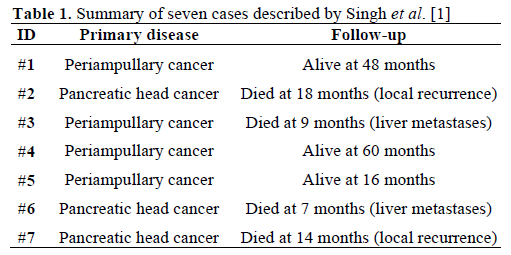
We read with interest the paper by Singh et al. who described their experience with synchronous resection of solitary liver metastases with pancreaticoduodenectomy [1]. Two-hundred and thirty patients underwent pancreaticoduodenectomy for pancreatic and periampullary cancer at their institution unit between September 2003 and September 2009. Seven patients (3%) underwent synchronous resection of a solitary liver metastasis. Among these seven patients, four had periampullary cancer while three underwent pancreaticoduodenectomy for pancreatic cancer. Liver metastasis was located in the left lobe in three patients while it was in the right lobe in four patients. Resections were in the form of left lateral segmentectomies in two patients and metastasectomy in five patients. In patients undergoing resection of liver metastasis, there were four recurrences over a mean follow-up of 21 months. All patients who had synchronous liver resections received chemotherapy versus 134 (60.1%) of the other 223 patients undergoing pancreaticoduodenectomy (P=0.576).
In my opinion, the results of this small case series was akin to previous experiences, in particular to Johns Hopkins experience [2]. The authors mentioned that all the patients who had synchronous liver resections received chemotherapy but no regimen was disclosed. Gemcitabine remains the only chemotherapeutic agent approved by FDA for the treatment of pancreatic cancer, both in the adjuvant and metastatic setting. Review of cases (Table 1) indicated that two only patients had pancreatic cancer and their survival was 7 and 14 months, respectively. Adjuvant gemcitabine study by Oettle et al. [3] showed that median diseasefree survival was 13.4 months in the gemcitabine group (95% confidence interval (CI): 11.4-15.3 months) and 6.9 months in the control group (95% CI: 6.1-7.8 months; P<0.001, log-rank test).
Neoptolemos et al. [4] performed the European Study Group for Pancreatic Cancer (ESPAC-3) study, a multicenter, international, open-label, randomized, controlled, phase III trial that aimed at comparing of adjuvant 5-fluorouracil/leucovorin versus gemcitabine in patients with resected pancreatic adenocarcinoma. Patients with an R0/R1 resection for pancreatic adenocarcinoma were randomized (stratified for resection margin status and country) starting before 8 weeks of surgery to receive either 5-fluorouracil/ leucovorin or gemcitabine for 6 months. The study confirmed the role of adjuvant chemotherapy. However, overall survival was similar on both arms, hence showing that gemcitabine is not superior to 5- fluorouracil in adjuvant setting. Median overall survival was 23.0 months (95% CI: 21.1-25.0 months) with 5-fluorouracil/leucovorin and it was 23.6 months (95%CI: 21.4-26.4 months) with gemcitabine. There was no significant difference in the effect of treatment across subgroups according to R status (P=0.56). The study also confirmed the role of prognostic factors (whatever adjuvant chemotherapy): grade, stage, nodal status, resection status. The authors did not give any information on the grade and nodal status of the patients [1].
We concur that surgical resection of adenocarcinoma of the pancreas or periampullary area potentially offers the only possibility of long-term survival, however, the role of metastasectomy in patients with hepatic metastases from pancreatic adenocarcinoma remains to be elucidated. Despite an aggressive surgical approach that involved extirpation of both the primary and metastatic disease sites, patients with synchronous pancreatic adenocarcinoma and hepatic metastases have a poor prognosis as revealed in this study (Table 1; last two patients). Also, the complications of this surgery in low volume centers can be very risky.
Given the poor prognosis of patients with metastatic disease, we suggest that neo-adjuvant approaches with systemic chemotherapy, especially with newer regimens, such as 5-fluorouracil, leucovorin, irinotecan and oxaliplatin (FOLFIRINOX), [5] should be used in these patients before making any surgical decisions. Laparoscopic staging should always be performed.
In a nut shell, the selection of appropriate patients for hepatic resection of metastatic pancreatic and periampullary cancers must be individualized. Careful clinical judgment and prudent selection of patients as part of a multidisciplinary approach are mandatory.
Conflict of interest
The author has no potential conflict of interest
References
- Singh A, Singh T, Chaudhary A. Synchronous resection of solitary liver metastases with pancreaticoduodenectomy. JOP. JPancreas (Online) 2010; 11:434-8. [PMID 20818110]
- Gleisner AL, Assumpcao L, Cameron JL, Wolfgang CL, ChotiMA, Herman JM, et al. Is resection of periampullary or pancreaticadenocarcinoma with synchronous hepatic metastasis justified?Cancer 2007; 110:2484-92. [PMID 17941009]
- Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, RidwelskiK,et al. Adjuvant chemotherapy with gemcitabine vs observation inpatients undergoing curative-intent resection of pancreatic cancer: arandomized controlled trial. JAMA 2007; 297:267-77. [PMID17227978]
- Neoptolemos J, Büchler M, Stocken DD, Ghaneh P, Smith D, C. Bassi C, et al. A multicenter, international, open-label, randomized,controlled phase III trial of adjuvant 5-fluorouracil/folinic acid (5-FU/FA) versus gemcitabine (GEM) in patients with resected pancreatic ductal adenocarcinoma. J ClinOncol 2009; 27(18Suppl):Abstract LBA4505.
- Breysacher G, Kaatz O, Lemarignier C, Chiappa P, Roncalez D, Denis B; et al. Safety and clinical effectiveness of FOLFIRINOX inmetastatic pancreas cancer (MPC) after first-line chemotherapy. 2010ASCO Gastrointestinal Cancers Symposium. Abstract No. 269.

