Keywords
Pancreatic Function Tests; Pancreatic Neoplasms; Pancreatitis; Secretin; Zinc
Abbreviations
CP: chronic pancreatitis; EGD: esophagogastroduodenoscopy; ERCP: endoscopic retrograde cholangiopancreatography; EUS: endoscopic ultrasound; FNA: fine needle aspiration; PC: pancreatic cancer
Presentation
This study is an oral presentation in distinguished abstract plenary sessions at Digestive Disease Week, May 14- 19, 2005, Chicago, Illinois
INTRODUCTION
Pancreatic cancer (PC) is the fourth leading cause of cancer death, with more than 30,000 fatal cases annually in the United States [1]. Several reports have demonstrated that chronic pancreatitis (CP) may be one of the most significant risk factors for pancreatic cancer with the pathogenesis yet to be identified [2, 3, 4, 5]. This could be due to possible effects of reactive oxygen species generated during episodes of acute and chronic pancreatitis on tumor initiation and transformation [5]. Previous studies have shown that malignant transformation is usually accompanied by lowered antioxidant activities [6, 7]. In addition, increased cellular reactive oxygen species are associated with carcinogenesis, whereas antioxidants prevent malignant transformation both in vitro and in vivo studies [8, 9]. Therefore, an imbalance of free oxygen species and scavenging processes has been implicated in the pathogenesis of pancreatic injury resulting in malignant transformation.
Zinc is one of the major components of antioxidant enzymes and may play a role in the pathogenesis of CP and PC [5, 10]. A recent report demonstrated a significant decrease in level of pancreatic zinc output in patients with CP [11]. Thus, the level of zinc output was proposed as an alternative marker to assess pancreatic function for the diagnosis of CP [11]. However, this proposed method requires a double-lumen tube placement with the tip positioned close to the ligament of Treitz for aspiration of fluid for 90 minutes. Due to the cumbersome nature of prolonged duodenal intubation resulting in patient’s discomfort and the unavailability of this procedure across the majority of community hospital in United States, this method is likely not applicable to general practice.
Recently, we reported our experiences with an endoscopic pancreatic function test using a standard esophagogastroduodenoscopy (EGD) following an intravenous injection of secretin to collect fluid exiting from the ampulla of Vater for 10 minutes [12]. This method is simple and more practical to use in clinical practice [12]. In the current study, we aim to determine the role of zinc concentration in pancreatic fluid to differentiate normal pancreas from CP and PC using our previously reported technique [12]. We hypothesize that patients with pancreatic diseases, either CP or PC, have significantly reduced zinc concentrations in pancreatic fluid compared to controls with normal pancreas.
PATIENTS AND METHODS
Between January 2003 and May 2004, 75 consecutive patients with clinical signs and/or symptoms suggestive of pancreatic diseases were prospectively evaluated at the pancreas clinic of the Mayo Clinic Jacksonville, Florida, USA.
The final diagnosis of CP was determined according to the Cambridge classification at endoscopic retrograde cholangiopancreatography (ERCP) [13] and by histology in patients who underwent surgery. The diagnosis of PC was established using cytology results demonstrating malignant cells by endoscopic ultrasonography (EUS)- guided fine needle aspiration (FNA) and/or final pathology in patients who had surgery. All patients underwent EGD and ERCP under standard conscious sedation (intravenous midazolam and meperidine). The EGD and ERCP were performed on different days but within 60 days (median: 2 days; range: 0-53 days) of each other.
Secretion of pancreatic fluid was induced by an intravenous injection of secretin (SecreFloTM; Repligen Corporation, Silver Spring, MD, USA) at the dose of 0.2 μg/kg immediately before an EGD [12]. A total of 10 mL of pancreatic fluid exiting from the ampulla of Vater was collected from the second portion of the duodenum using a standard disposable washing aspiration catheter (7 French size, 240 cm in length; Wilson Cook, Winston-Salem, NC, USA) immediately frozen in liquid nitrogen and stored at -80 °C until the analysis was performed.
Zinc concentrations were determined using inductively coupled plasma optical emission spectroscopy. Aqueous acidic calibrating standards were diluted with a matrix plasma or serum containing a normal concentration of zinc. Blanks were diluted with the aqueous acidic diluent containing internal standards but no serum matrix. Patient samples and quality control specimens were also diluted in an identical manner. In turn, all diluted blanks, calibrating standards, quality control samples, and patient samples were aspirated into a pneumatic nebulizer and the resulting aerosol directed to the hot plasma discharge by a flow of argon. In the annular plasma, the aerosol was vaporized, atomized, and then ionized. Emission signals from zinc and the internal standard were observed axially by the emission spectrometer. Instrumentation response was defined by using the linear relationship of analyte concentration versus the ration of the zinc emission signal ratioed with the internal standard. After reagent blank subtraction, unknown zinc concentration of samples was calculated by entering the net unknown zinc intensity ratio into the linear calibration equation.
Patient characteristics and zinc concentrations of pancreatic fluid from patients with CP and PC were compared to control patients with normal pancreas.
ETHICS
The study was reviewed and approved by the Mayo Foundation Institutional Review Boards and the protocol conforms to the ethical guidelines of the World Medical Association Declaration of Helsinki.
STATISTICS
Median range and frequencies were used as descriptive statistics. All statistical analyses were performed by SPSS (Statistical Package for the Social Sciences. Chicago, IL, USA) software version 13. Comparisons were performed using non-parametric tests (Kruskal-Wallis and Pearson chi-square test). Multinomial logistic regression was further performed to adjust for confounding factors. Statistical significance was achieved for a P value less than 0.05.
RESULTS
Of 75 patients enrolled in the study, 38 controls were confirmed to have normal pancreas by normal ERCP while 20 and 17 patients were determined to have CP and PC, respectively. Of 20 patients with CP, 16 patients were diagnosed by ERCP and the remaining 4 patients were diagnosed by pathology. Of 17 patients with PC, 12 patients had positive cytology results from EUS-FNA and the remaining 5 patients were diagnosed by pathology. Fourteen of these patients (82%) had pancreatic ductal adenocarcinoma, 1 patient (6%) had acinar cell carcinoma, and 2 patients (12%) had intraductal papillary mucinous neoplasm with invasive carcinoma. The alternative diagnoses of 38 controls were: peptic ulcer diseases (n=3), non-ulcerative dyspepsia (n=11), irritable bowel syndrome (n=16), symptomatic cholelithiasis (n=2), and radiating neuropathic pain from spine abnormalities (n=6).
Patient demographics (age and gender distribution), body mass index, history of alcohol use, and prevalence of diabetes mellitus were compared among groups and demonstrated in Table 1. Patients with PC were significantly older compared to patients with CP and normal pancreas with the median of 73, 58, and 49 years, respectively (P<0.001). Gender distribution (P=0.098), body mass index (P=0.925), and history of alcohol use (P=0.997) were similar among groups. Prevalence of diabetes mellitus was significantly different among the 3 groups (P=0.002). Every patient consumed a regular western diet and none was taking zinc supplements. Serum amylase and lipase levels were normal at the time of pancreatic fluid collection. Comparison of zinc concentrations in pancreatic fluid among groups was performed and demonstrated in Figure 1. The median of zinc concentrations in patients with normal pancreas was 0.98 μg/mL (range: 0.26-11.10) compared to 1.02 μg/mL (range: 0.29-3.24) in patients with CP and 1.35 μg/mL (range: 0.52-5.43) in patients with PC. No statistically significant differences were demonstrated among groups (P=0.129). In addition, multinomial logistic regression analysis adjusting for age and prevalence of diabetes mellitus was further performed and confirmed no significant difference of zinc concentration in pancreatic fluid among groups (P=0.678).
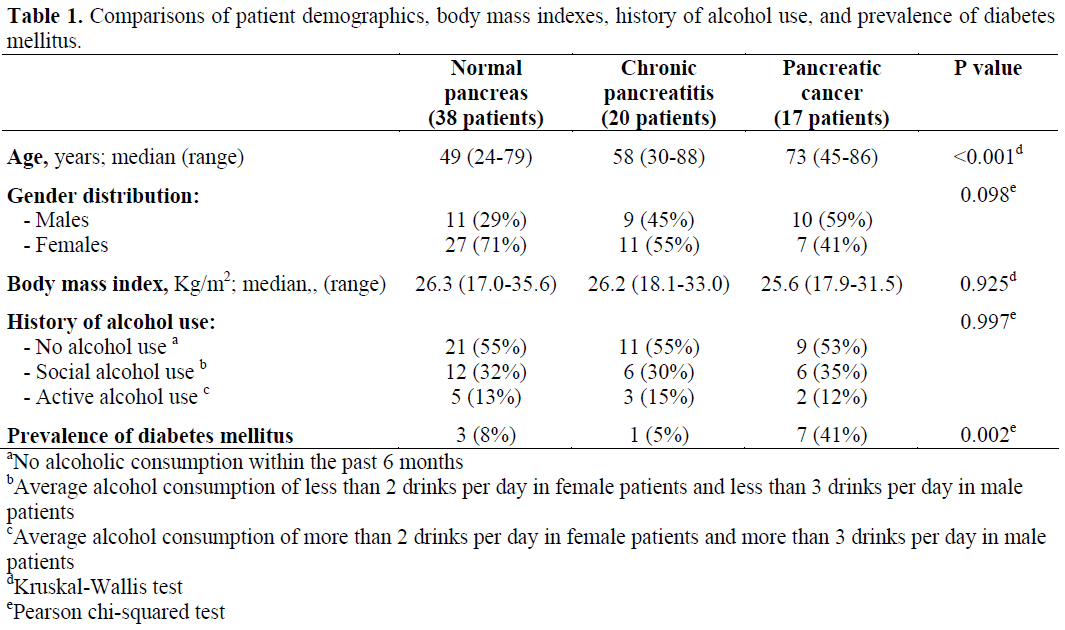
Figure 1. Comparison of zinc concentration in
pancreatic fluid. Data is illustrated in box-and-whisker
plot. Box represents the median and interquartile range.
Whisker line represents the maximal and minimal
distributions of data set. (mcg = μg)
DISCUSSION
Chronic pancreatitis is a well-defined disease based on histopathology, but for clinical purposes, diagnosis is generally not based on a histological examination. It remains challenging especially in the early stage of disease because of an inability to obtain a tissue sample due to a deep-seated retroperitoneal location of pancreas and a high incidence of complications after core tissue biopsy [14]. To date, direct and invasive tests of pancreatic exocrine function using intravenous hormonal stimulants (cholecystokinin and/or secretin) infusion and duodenal drainage analysis are considered the gold standard for diagnosis. Unfortunately, these tests are only available in a selected number of tertiary care referral centers in the United States. Their limitations include the need for a specialized gastroenterology laboratory for fluid analysis, the cumbersome nature of prolonged duodenal intubation (at least 90 minutes) resulting patient’s discomfort and time consumption, and lack of a universal laboratory standard. Thus, the concept of a simple and fast direct pancreatic exocrine function test that can be performed concurrently with an EGD has been proposed in several studies [13, 15, 16, 17]. With the similar concept of using an intravenous hormonal injection to stimulate pancreatic exocrine function for measurement of pancreatic enzymes and/or bicarbonate concentrations in pancreatic fluid, the feasibility of the tests were demonstrated with estimated sensitivity and specificity ranging from 60-92% and 70-95%, respectively [13, 15].
Because of several previous reports confirming possible correlations between antioxidant activities and pathogenesis of pancreatic tissue injury resulting in CP and possibly PC, an idea of identifying the other marker, which is a major component of these antioxidants to accurately diagnose CP and PC was attempted. We have recently reported a lack of correlation of selenium concentration in pancreatic fluid and the presence of chronic pancreatitis [18]. A recently published study demonstrated that pancreatic zinc output following an intravenous infusion of secretin could be accurately used in diagnosis of CP with the sensitivity and specificity of 97% and 91%, respectively [11]. However, this method still requires a prolonged duodenal intubation with a double-lumen tube for 90 minutes that may result in the similar patient’s discomfort and low tolerability, similar to the standard pancreatic exocrine function tests.
In the current study, we report our experience in using an EGD with a 10-minute collection of pancreatic fluid to determine zinc concentration in pancreatic fluid following an intravenous injection of secretin in patients with a suspicion of pancreatic diseases. The results demonstrated that zinc concentration in pancreatic fluid was similar in patients with CP compared to patients with normal pancreas. Thus, it is interesting that the results of our study did not confirm findings from the previous study and zinc concentration in pancreatic fluid cannot be used reliably to support the diagnosis of CP. In addition to CP, our study also demonstrated that there was no significant difference in zinc concentration in pancreatic fluid from patients with PC compared to patients with normal pancreas or CP. Thus, zinc concentration in pancreatic fluid cannot be reliably used to differentiate PC from normal pancreas and CP.
The discrepancy of our results compared to findings from the previous study remained unclear. However, it may probably be explained by significant differences in methodology and patient population being studied. In the previous study, approximately 80% of patients with CP being evaluated had either moderate or severe CP based on bicarbonate output while only 25% and 20% of patients in our study had moderate and severe CP defined by the Cambridge classification at ERCP, respectively. It seems logical that the patients with more severe CP would have higher degree of impaired pancreatic exocrine functions leading to more pronounced difference when compared to patients with normal pancreas. Besides, the methodology of pancreatic fluid collection was also dissimilar. Due to a short duration of pancreatic fluid collection by our method, a total quantification of zinc output cannot be performed and zinc concentration was therefore instead used in our analyses. The zinc concentration of pancreatic fluid may vary over time. Thus, this may be another important factor resulting in the disagreement of our results compared to the previous study. In summary, our study demonstrated that zinc concentration in pancreatic fluid is similar in patients with CP and PC compared to patients with normal pancreas. Using a simple EGD and a 10-minute direct endoscopic collection of pancreatic fluid immediately after an intravenous infusion of secretin, our results did not confirm findings from the previous study. Thus, until proven in a larger, multicenter study, zinc concentration in pancreatic fluid should not be reliably used to differentiate patients with CP and/or PC from those without pancreatic diseases.
References
- Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, et al. Cancer statistics, 2005. CA Cancer J Clin 2005; 55:10-30. [PMID 15661684]
- Ammann RW, Knoblauch M, Mohr P, Deyhle P, Largiader F, Akovbiantz A, et al. High incidence of extrapancreatic carcinoma in chronic pancreatitis. Scand J Gastroenterol 1980; 15:395-99. [PMID 7433900]
- Lowenfels AB, Maisonneuve P, Cavallani G, Ammann RW, Lankisch PG, Andersen JR, et al. Pancreatitis and the risk of cancer. N Engl J Med 1993; 328:1433-7. [PMID 8479461]
- Traverso LW, Kozarek RA, Simpsom T, Galagan KA. Pancreatic duct obstruction as a potential etiology of pancreatic adenocarcinoma: a clue from pancreas divisum. Am J Gastroenterol 1993; 88:117-9. [PMID 8420250]
- Cullen JJ, Mitros FA, Oberley LW. Expression of antioxidant enzymes in diseases of the human pancreas: another link between chronic pancreatitis and pancreatic cancer. Pancreas 2003; 26:23-7. [PMID 12499913]
- Oberley LW, Buettner GR. Role of superoxide dismutase in cancer: a review. Cancer Res 1979; 39:1141-9. [PMID 217531]
- Oberley LW, Oberley TD. Role of antioxidant enzymes in cell immortalization and transformation. Mol Cell Biochem 1988; 84:147-53. [PMID 3068520]
- Cerutti P. Prooxidant states and tumor promotion. Science 1985; 227:375-81. [PMID 2981433]
- Cerutti P, Ghosh R, Oya Y, Amstad P. The role of the cellular antioxidant defense in oxidant carcinogenesis. Environ Health Perspect 1994; 102(Suppl 10):123-9. [PMID 7705286]
- Hausmann DH, Porstmann T, Weber I, Hausmann S, Dummler W, Liebe S, Emmrich J. Cu/Zn-SOD in human pancreatic tissue and pancreatic juice. Int J Pancreatol 1997; 22:207-13. [PMID 9444552]
- Dominguez-Munoz JE, Martinez SM, Leodolter A, Malfertheiner P. Quantification of pancreatic zinc output as pancreatic function test: making the secretincaerulein test applicable to clinical practice. Pancreatology 2004; 4:57-62. [PMID 14988659]
- Raimondo M, Imoto M, DiMagno EP. Rapid endoscopic secretin stimulation test and discrimination of chronic pancreatitis and pancreatic cancer from disease controls. Clin Gastroenterol Hepatol 2003; 1:397-403. [PMID 15017660]
- Axon AT, Classen M, Cotton PB, Cremer M, Freeny PC, Lees WR. Pancreatography in chronic pancreatitis: international definitions. Gut 1984; 25:1107-12. [PMID 6479687]
- Chowdhury RS, Forsmark CE. Pancreatic function testing. Aliment Pharmacol Ther 2003; 17:733-50. [PMID 12641496]
- Conwell DL, Zuccaro G Jr, Vargo JJ, Morrow JB, Obuchowski N, Dumot JA, et al. An endoscopic pancreatic function test with cholecystokininoctapeptide for the diagnosis of chronic pancreatitis. Clin Gastroenterol Hepatol 2003; 1:189-94. [PMID 15017490]
- Conwell DL, Zuccaro G Jr, Vargo JJ, Trolli PA, Vanlente F, Obuchowski N, et al. An endoscopic pancreatic function test with synthetic porcine secretin for the evaluation of chronic abdominal pain and suspected chronic pancreatitis. Gastrointest Endosc 2003; 57:37-40. [PMID 12518128]
- Conwell DL, Zuccaro G, Morrow JB, Van Lente F, Obuchowski N, Vargo JJ, et al. Cholecystokininstimulated peak lipase concentration in duodenal drainage fluid: a new pancreatic function test. Am J Gastroenterol 2002; 97:1392-7. [PMID 12094856]
- Scolapio JS, Raimondo M, Woodward TA, Wallace MB. Selenium concentrations in pancreatic juice of patients with chronic pancreatitis. JPEN J Parenter Enteral Nutr 2004; 28:339-41. [PMID 15449574]


