Keywords
Laparoscopy; Pancreas; Pancreatectomy; Stents
Abbreviations
BMI: body mass index
INTRODUCTION
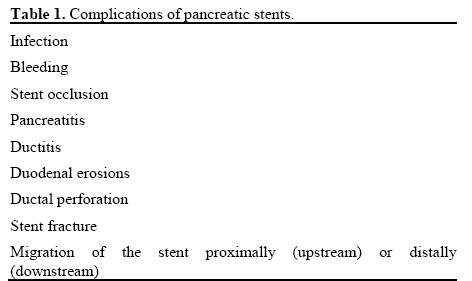
Pancreatic stents are widely used for both benign and malignant biliopancreatic diseases such as strictures or obstruction of the biliary tract, chronic pancreatitis, pancreatic pseudocysts, duct disruption, obstructing stones, and prophylaxis for the prevention of acute pancreatitis after ERCP in high-risk patients [1, 2]. Although usually well tolerated, complications can occur. The most common complications are depicted in Table 1 [1]. Proximally or upstream migration (toward the tail of the pancreas) of the stent occurs in 2% to 5% of cases [1, 2, 3]. Risk factors for proximal migration include chronic pancreatitis, sphincter of Oddi dysfunction, and long pancreatic stents [4, 5]. Migrated stents can cause problems such as occlusion, ductitis, ductal stenosis, infection, pancreatitis, and chronic pain; thus, extraction is desirable. Endoscopic extraction of migrated stents is successful in 75% to 80% of cases using a balloon, polypectomy snare, or endoscopic forceps. Other options include cannulation or the use of endoscopic baskets [1]. Risk factors for failure of an endoscopic approach are distal duct stenosis, stent impaction, duct edema, fragmentation, and the type of stent used (pigtail, flapped stents) [1, 4]. There are some reported cases of treatments for asymptomatic non-complicated impacted pancreatic stents after a follow-up period of up to two years [1, 6]; however, there is not sufficient data to support conservative management. We report a case of a retained impacted proximally migrated pancreatic duct stent extracted through a laparoscopic approach with central pancreatectomy.
CASE REPORT
A 43-year-old female with history of morbid obesity (BMI equal to 45 kg/m2), dietary controlled diabetes mellitus, and depression presented to an outside institution complaining of a three-month history of persistent and worsening vague abdominal pain. She was found to have cholelithiasis by ultrasound as well as a dilated bile duct with abnormal liver enzymes. She underwent ERCP with failure to cannulate the bile duct. After several pancreatograms, a 3 cm long 5 Fr single pigtail pancreatic stent was placed to prevent post ERCP pancreatitis. The pancreatic duct stent was later found to have migrated into the neck of the pancreas, and she subsequently developed moderate pancreatitis after the procedure, requiring a nine day hospitalization. Two subsequent endoscopic attempts to remove the impacted stent were performed on days 5 and 26 after the first ERCP, but these were unsuccessful. The patient continued to have epigastric pain with amylase elevation and was also found to have radiographic evidence of acute cholecystitis. She underwent a reportedly difficult laparoscopic cholecystectomy, which was associated with a prolonged recovery time. The patient was then referred to our institution. A fourth attempt of endoscopic extraction was attempted but unsuccessful due to the inability to pass a guidewire past the embedded stent. This last ERCP revealed a proximally migrated stent into the ventral pancreatic duct at the level of the genu and proximal body of the pancreas (Figure 1). The main duct and side branches were moderately dilated. A computerized tomography scan showed the stent causing proximal pancreatic ductal dilation (Figure 2). The patient was then consulted for surgical management of the impacted stent.
Figure 1. ERCP image of the impacted retained pancreatic duct
(arrow) stent within the genu and proximal body of the pancreas.
Figure 2. Computerized axial tomographic image showing the
impacted retained pancreatic duct stent (arrow).
After reviewing the case, the patient was found to have continued epigastric pain and required narcotics. The stent had been present for three months, causing two episodes of acute pancreatitis and was beginning to cause changes consistent with chronic pancreatitis. Therefore, she was considered a candidate for operative removal of the stent. She was taken to the operating room for a laparoscopic attempt at stent removal. The options considered were a transduodenal ampullary exploration, a subtotal pancreatectomy, a longitudinal pancreatotomy with pancreaticojejunostomy, or a central pancreatectomy with pancreaticogastrostomy. The latter option was chosen due to the difficulty traversing the pancreatic duct within the head of the pancreas for a transduodenal ampullary approach, the significant amount of healthy pancreatic parenchymal removal in a diet controlled diabetic with a large resection, and the difficulties associated with the relatively small size and soft consistency of the pancreas with a longitudinal pancreatotomy respectively.
SURGICAL TECHNIQUE
After accessing the abdomen through a supraumbilical Hasson approach, four additional trocars were placed in a semicircle around the head of the pancreas (three 5 mm and one 12 mm). The stomach was elevated off of the head, neck, and body of the pancreas. An intraoperative ultrasound was performed to find the distal aspect of the impacted stent. Once this was confirmed, the pancreas was circumferentially dissected free from the retroperitoneum and vasculature at this site. Then, using an ultrasonic dissecting device, the pancreas was slowly and methodically transected starting at the inferior border and proceeding from caudal to cranial. As the dissection proceeded, the pancreatic duct was then identified within the pancreatic parenchyma and transected with cold scissors. The pancreatic stent was identified (Figure 3) and removed without difficulty. The parenchyma proximal to this ductotomy site was transected with an endoscopic stapling device with staple line reinforcement using a slow compression technique. The pancreas to the left of the site of division was fully mobilized for approximately 3 cm and aligned to the posterior wall of the stomach. An anterior vertical gastrotomy was made, and a site was chosen for the posterior gastrotomy. A gastrotomy was made on the posterior wall of the stomach corresponding to the size of the distal remnant pancreas, and the pancreas was internalized into the stomach by pulling on the staple line. Then, the division of the partially transected pancreas at the level of the ductotomy was completed, resulting in a 2 cm segment of remnant pancreas invaginated into the stomach (Figure 4). An inner layer of running absorbable suture was used to create the pancreaticogastrostomy (Figure 5). An outer layer of running absorbable suture was placed from the nine o’clock to three o’clock position to further anchor the pancreas to the stomach (Figure 6). A 15F drain was placed in the region of the anastomosis. The patient tolerated the procedure very well, with a total operative time of 250 minutes, and recovered without any complications. The drain was found to have low volume and low amylase drainage on postoperative day six and was removed, and the patient was discharged. The patient noticed an immediate improvement in her epigastric pain, which continued to improve into follow-up.
Figure 3. Pancreatic ductotomy with exposure of the impacted 5 Fr pigtail pancreatic duct stent and subsequent removal with grasper and dissector
devices.
Figure 4. View of the invaginated face of the distal remnant pancreas
with pancreatic duct (arrow) protruding through the posterior wall of
the stomach and seen through the anterior gastrotomy.
Figure 5. Circumferential running suture to create the inner layer for
pancreaticogastrostomy reconstruction.
Figure 6. Partial circumferential running suture to anchor the
pancreaticogastrostomy reconstruction.
DISCUSSION
Retained and embedded proximally migrated pancreatic stents have the potential for causing complications such as occlusion, pain, infection, and pancreatitis among others. When endoscopic retrieval fails, surgical intervention is considered, and consultation with an experienced pancreatic surgeon is advised as an early surgical retrieval of the stent could decrease the risk of the complications mentioned above and others related to multiple failed endoscopic or percutaneous attempts. Surgical options include transduodenal ampullary attempts at stent removal, pancreatotomy with reconstruction, or resection procedures such as distal pancreatectomy. Local anatomic factors, underlying indications for pancreatic duct stent placement, patient age and comorbidities, and location of the retained stent within the pancreas will determine which surgical intervention is best for each patient. For our particular patient, a more distal approach was needed, as they had a tortuous narrowed pancreatic duct within the head of the pancreas and a stent was embedded in the neck and proximal body of the pancreas. Parenchymal salvage was ideal in her case due to her pre-diabetic condition and possible large parenchymal volume loss with distal pancreatectomy. Therefore, a central pancreatectomy with pancreaticogastrostomy reconstruction suited this patient best. Additionally, this patient was also felt likely to benefit from a laparoscopic approach, which has proven safe and effective for other complex pancreatic procedures [7].
First described in 1982 for the treatment of benign and borderline lesions of the neck of the pancreas [8], central pancreatectomy has gained increasing interest among pancreatic surgeons due to its theoretical benefits derived from a reduced parenchyma resection. However, a theoretical increased risk of pancreatic leak due the presence of two cut surfaces have been thought to overcome its potential benefits over distal pancreatectomy [9]. Different studies in the past have shown variable complication rates ranging from 13% to 62% and pancreatic fistula rates ranging from 0% to 62% [10]. The largest single institution series reported to date showed a lower incidence of new onset or worsened diabetes mellitus, with less insulin requirements among patients who underwent a central pancreatectomy compared to those with a distal pancreatectomy. Both groups were matched and showed no difference in mean operating room time, morbidity, mortality, length of stay and blood loss [10]. Overall complication and fistula rate were 41.1% and 20.5%, respectively.
Reports on minimally invasive central pancreatectomy have been relatively rare but have been shown to be technically possible with comparable fistula and complication rates to the open approach [11]. Generally, pancreaticogastrostomy reconstruction was favored among these reports. Pancreaticogastrostomy reconstruction is associated with less operative time, as it is technically simpler than constructing a Roux jejunal limb with pancreaticojejunostomy creation. While pancreaticogastrostomy was shown to have a higher incidence of pancreatic fistula over pancreaticojejunostomy reconstruction after central pancreatectomy in a small French study [12], a thorough meta-analysis of reconstruction techniques after pancreaticoduodenectomy showed no difference in fistula rates depending on the type of anastomosis [13].
CONCLUSION
This report suggests that a laparoscopic approach to central pancreatectomy for the unusual indication of a retained embedded pancreatic stent is a feasible and safe option. Our patient clearly benefitted from a parenchymal sparing, minimally invasive approach to affect removal of the impacted stent and avoidance of continued pancreatitis with the development of chronic pancreatitis.
Disclosure statement
No competing financial interest exist
Financial support
None
References
- Price LH, Brandabur JJ, Kozarek RA, Gluck M, Traverso WL, Irani S. Good stents gone bad: Endoscopic treatment of proximally migrated pancreatic duct stents. Gastrointest Endosc. 2009; 70(1):174-9. [PMID: 19559842].
- Choudhary A, Bechtold ML, Arif M, Szary NM, Puli SR, Othman MO, et al. Pancreatic stents for prophylaxis against post-ERCP pancreatitis: a meta-analysis and systematic review. Gastrointest Endosc. 2011; 73(2):275-82. [PMID: 21295641].
- JohansonJF.,Achmalz MJ. Geenen JE. Incidence and risk factors for biliary and pancreatic stent migration. Gastrointest Endosc. 1992; 38:341-346. [PMID: 1607087].
- Gong B, Sun B, Hao LX, Bie L. Usefulness of an algorithm for endoscopic retrieval of proximally migrated 5Fr and 7Fr pancreatic stents. Hepatobiliary Pancreat Dis Int. 2011; 10(2):196-200. [PMID: 21459728].
- Lucas D, Glaser J, Pearl J. Laparoscopic distal pancreatectomy for retrieval of a proximally migrated pancreatic stent. JSLS 2012; 16:169-172. [PMID: 22906350].
- Lahoti S, Catalano MF, Geenen JE, Schmalz. Endoscopic retrieval of proximally migrated biliary and opancreatic stents: experience of a large referal center. Gastrointest Endosc 1998:50:124-5. [PMID: 9647373].
- Asbun HJ, Stauffer JA. Laparoscopic vs open pancreaticoduodenectomy: Overall outcomes and severity of complications using the accordion severity grading system. J Am Coll Surg. 2012; 215(6):810-9. [PMID: 22999327].
- Dagradi ASG: Pancreatectomia Intermedia. EnciclopediaMedicaItaliana. Firenze, USES Edizioni Scientifiche, 1984, vol XI, pp 850– 851.
- Roggin KK, Rudloff U, Blumgart LH, Brennan MF. Central pancreatectomy revisited. J Gastrointest Surg. 2006;10(6):804-12. [PMID: 16769536].
- DiNorcia J, Ahmed L, Lee MK, Reavey PL, Yakaitis EA, Lee JA, et al. Better preservation of endocrine function after central versus distal pancreatectomy for mid-gland lesions. Surgery. 2010; 148(6):1247-54; discussion 1254-6. [PMID: 21134558].
- Winer J, Can MF, Bartlett DL, Zeh HJ, Zureikat AH. The current state of robotic-assisted pancreatic surgery. Nat Rev Gastroenterol Hepatol. 2012; 9(8):468-76. [PMID: 22733352].
- Venara A, de Franco V, Mucci S, Frampas E, Lermite E, Regenet N, Hamy A. Central pancreatectomy: comparison of results according to the type of anastomosis. J Visc Surg. 2012;149(2):e153- 8. [PMID: 22317930].
- Wente MN, Shrikhande SV, Müller MW, Diener MK, Seiler CM, Friess H, Büchler MW. Pancreaticojejunostomy versus pancreaticogastrostomy: systematic review and meta-analysis. Am J Surg. 2007;193(2):171-83. [PMID: 17236843].







