Mirjam Keßler*, Wolfgang Rottbauer, and Jochen Wöhrle
Department of Cardiology, University Hospital Ulm, Ulm, Germany
*Corresponding Author:
Mirjam Keßler
Department of Cardiology
University Hospital Ulm
Albert-Einstein-Allee 23
89081, Ulm, Germany
Tel:004973150045064, +497315000
E-mail: mirjam.kessler@uniklinik-ulm.de
Received date: Mar 1, 2017; Accepted date: Mar 4, 2017; Published date: Mar 7, 2017
Citation: Kelber M, Rottbauer W, Jochen W. Left Ventricular Perforation in A Patient with Lung Cancer Treated with Bevacizumab. Interv Cardiol J 2017, 3:1. doi:10.21767/2471-8157.100051
Keywords
Acute myocardial infarction; Ventricular perforation; Cardiotoxicity; Cardiac MRI; Bevacizumab
Introduction
Lung cancer is the leading cause of cancer-related death worldwide. Despite several mostly platinum-based chemotherapeutic regimens, a plateau of survival has been reached. In search of new therapeutic strategies, molecular targeted agents emerged for the treatment of non-small-cell lung cancer (NSCLC): Monoclonal antibodies against the epidermal growth factor receptor and vascular endothelial growth factor receptor or tyrosine kinase inhibitors. These targeted therapies do not have the severe systemic adverse effects usually observed with traditional cytotoxic drugs. However, each of these molecular targeted agents features their own spectrum of characteristic adverse effects. The humanized monoclonal antibody against the VEGF-A ligand Bevacizumab binds to its circulating target and thereby inhibits angiogenesis. Since 2004, it has been approved not only for the treatment of NSCLC but also a variety of solid tumors, e.g. ovarian, cervical, breast, renal cell, and colorectal cancer [1-3].
The characteristic toxicities of Bevacizumab include hemorrhage, wound healing complications, gastrointestinal perforation, arterial thromboembolism, congestive heart failure, hypertension, and infusion-related hypersensitivity reactions [4]. Due to wound healing complications, discontinuation of Bevacizumab treatment at least 28 days before and after surgery is recommended by the manufacturer in a black box warning [4]. However, the full spectrum of the side effects of bevacizumab has not been discovered, yet.
In this report, we present a unique case of a myocardial infarction of the posterior wall complicated by a left ventricular free wall perforation associated with the treatment of NSCLC with Bevacizumab.
Case Report
A 62-year-old man presented with dyspnea at moderate exercise classified as NYHA II. The patient had a history of NSCLC at the stage cT4 cN0 cM1 (brain) with the histological features of an adenocarcinoma. After initial resection of the occipital brain metastasis and first-line chemotherapy containing Cisplatin and Gemcitabine, partial remission was achieved. 3 months later, the chemotherapy protocol was changed to Bevacizumab as second-line treatment due to renal toxicity of Cisplatin, which was applied for 8 months and resulted in stable disease.
Acute ST-segment elevation myocardial infarction of the posterior wall occurred, which was, in accordance with current cardiology guidelines, immediately treated with angioplasty and implantation of drug-eluting stents and antiplatelet medical therapy. The last administration of Bevacizumab was only a few hours prior to the onset of myocardial infarction.
At admission, initial transthoracic echocardiography showed pericardial effusion. After coronary revascularization, a cardiac magnetic resonance imaging (MRI) was performed. MRI, by late gadolinium enhancement, demonstrated the formation of a scar of the posterior and lateral wall of the left ventricle after myocardial infarction (Figure 1). In addition, a perforation of the basal lateral ventricular wall of 29 mm diameter was detected (Figure 2).
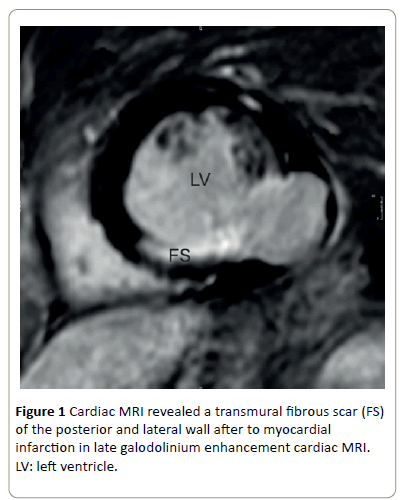
Figure 1: Cardiac MRI revealed a transmural fibrous scar (FS) of the posterior and lateral wall after to myocardial infarction in late galodolinium enhancement cardiac MRI.LV: left ventricle.
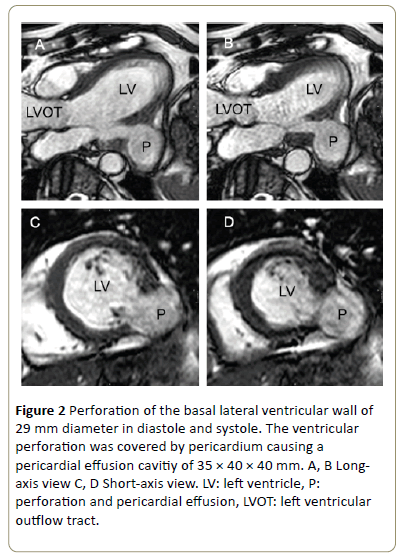
Figure 2: Perforation of the basal lateral ventricular wall of 29 mm diameter in diastole and systole. The ventricular perforation was covered by pericardium causing a pericardial effusion cavitiy of 35 × 40 × 40 mm. A, B Longaxis view C, D Short-axis view. LV: left ventricle, P:perforation and pericardial effusion, LVOT: left ventricular outflow tract.
The ventricular perforation was covered by pericardium causing a pericardial effusion. Due to high operative risk for cardiac surgery and stable circulatory condition, we discussed with the patient a conservative management. The patient was monitored for 1 week and antiplatelet therapy was continued regularly. Second-line chemotherapy containing Bevacizumab was discontinued.
2 months after initial admission, the patient was readmitted for follow-up cardiac magnetic imaging (Figure 3). He had neither chest pain, nor dyspnea. Long-term follow-up cMRI revealed a minimal regression of the ventricular perforation to 25 mm diameter and stable pericardial effusion. The patient had been asymptomatic for 6 months.
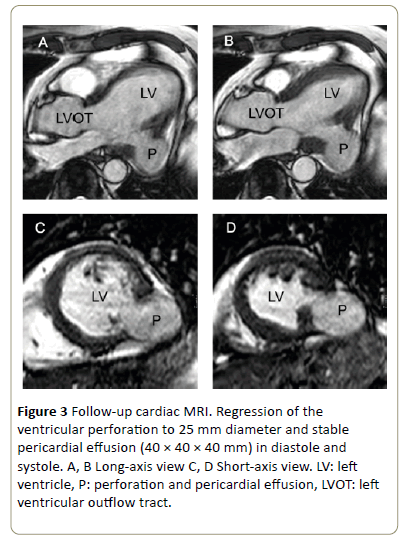
Figure 3: Follow-up cardiac MRI. Regression of the ventricular perforation to 25 mm diameter and stable pericardial effusion (40 × 40 × 40 mm) in diastole and systole. A, B Long-axis view C, D Short-axis view. LV: left ventricle, P: perforation and pericardial effusion, LVOT: left ventricular outflow tract.
Discussion
Ventricular perforation is a rare complication of myocardial infarction. The incidence ranges 0.93% to 2.7% and appears to decrease in the era of modern percutaneous coronary intervention. Acute ventricular perforation often results in fatal outcome due to cardiac rupture with pericardial tamponade and cardiogenic shock [5,6]. Sub-acute ventricular perforations have a more favourable outcome: A small number of patients survives this fatal complication with surgical, interventional, or conservative management [5].
Risk factors for sub-acute ventricular perforation are lateral or anterior myocardial infarction, delayed reperfusion strategy or hospitalization and peak creatine kinase-MB (CK-MB) above 150 IU/l. Other reported risk factors are female sex, age, and arterial hypertension [6]. Our patient obtained no relevant risk factors for ventricular perforation after myocardial infarction: Reperfusion of the right coronary artery causing the myocardial infraction of the posterior wall was achieved immediately without delay, peak CK-MB level was 56 IU/l. The arterial hypertension was well-controlled. However, myocardial infarction occurred after the administration of Bevacizumab for treatment of his NSCLC.
Combined treatment with Bevacizumab and chemotherapy is associated with an increased risk of arterial thromboembolism at a relative risk of 0.595-31.56 (p=0.35) [7,2] compared to controls. Risk factors for arterial thromboembolic events are age >65 years and history of arterial thromboembolic events. Furthermore, cardiac ischemia occurs at a relative risk of 1.12-4.65 during treatment with angiogenesis.
Inhibitors compared to routine care [7-9]. After arterial thromboembolic events Bevacizumab treatment has to be discontinued immediately [5]. Our patient had no risk factors for arterial thromboembolic events. Bevacizumab was administered prior to the myocardial infarction and Bevacizumab treatment was discontinued afterwards. However, myocardial infarction was predominantly based on atherosclerosis and no embolic event. Importantly, Bevacizumab therapy is also associated with wound-healing complications occurring in up to 15% of all patients [5]. Due to the estimated half-life of Bevacizumab of 20 days, the manufacturer recommends Bevacizumab to be suspended for 28 days prior to elective surgery and should not be initiated at least 28 days following surgery and must not be administered before the wound is fully healed [5]. In the present case, Bevacizumab was administered only a few hours prior to the myocardial infarction and hence was at effective blood levels during myocardial infarction and its healing process, suggesting that Bevazicumab is the major risk factor for myocardial wound-healing leading to ventricular perforation after myocardial infarction in our patient.
Moreover, perforation of the gastrointestinal tract is associated with treatment with Bevacizumab especially in patients with colorectal cancer. According to the manufacturer’s prescribing information, the FDA’s black box warning, and several studies, gastrointestinal perforations occur in 0.3% to 2.4% [4]. Perforations of other internal organs, in particular of the heart, have not been reported, yet. In this report, we present a unique case of a myocardial infarction of the posterior wall in a patient receiving treatment with Bevacizumab for NSCLC immediately before myocardial infarction. As a late complication of myocardial infarction, a subacute left ventricular free wall perforation occurred. Bevazicumab is known to cause wound-healing disturbances and hence contributed to ventricular perforation in our patient.
Conclusion
The humanized monoclonal antibody against the VEGF-A ligand, Bevacizumab inhibits angiogenesis. The characteristic toxicities of Bevacizumab include hemorrhage, wound healing complications, gastrointestinal perforation, arterial thromboembolism, congestive heart failure, hypertension, and infusion-related hypersensitivity reactions. Administration of Bevacizumab in NSCLC was associated with a sub-acute left ventricular free wall perforation after myocardial infarction of the posterior wall. Longterm cardiac MRI follow-up showed a minimal regression of the ventricular perforation.
References
- Di Costanzo F, Mazzoni F, Micol Mela M, Antonuzzo L, Checcacci D, et al. (2008) Bevacizumab in non-small cell lung cancer. Drugs 68:737-746.
- Lai XX, Xu RA, Yu-Ping L, Yang H (2016) Risk of adverse events with bevacizumab addition to therapy in advanced non-small-cell lung cancer: A meta-analysis of randomized controlled trials. Onco Targets Ther 9:2421-2428.
- Zustovich F, Ferro A, Lombardi G, Farina P, Zagonel V (2014) Bevacizumab-based therapy for patients with brain metastases from non-small-cell lung cancer: Preliminary results. Chemotherapy 60: 294-299.
- Genentech I (2009) U.S. BL 125085/169 Amendment: Bevacizumab-Genentech, In:Genentech, Inc. USA.
- Che J, Li G, Chen K, Liu T (2016) Post-mi free wall rupture syndrome. Case report, literature review, and new terminology. Clin Case Rep 4: 576-583.
- Vervaeke H, Becaus N, Penicka M, Vanderheyden M (2014) Self-limiting left ventricular wall rupture following myocardial infarction: A case report and literature review. Acta Cardiol 69: 209-212.
- Economopoulou P, Kotsakis A, Kapiris I, Kentepozidis N (2015) Cancer therapy and cardiovascular risk: Focus on bevacizumab. Cancer Manag Res 7: 133-143.
- Abdel-Qadir H, Ethier JL, Lee DS, Thavendiranathan P, Amir E (2016) Cardiovascular toxicity of angiogenesis inhibitors in treatment of malignancy: A systematic review and meta-analysis. Cancer Treat Rev 53: 120-127.
- Tanaka K, Sato N, Yasutake M, Takeda S, Takano T, et al. (2002)Clinical course, timing of rupture and relationship with coronary recanalizationtherapy in 77 patients with ventricular free wall rupture following acutemyocardial infarction. J Nippon Med Sch 69:481-488.

