Keywords
Meningeal Carcinomatosis; Pancreatic Neoplasms
Abbreviation
PF Pancreatic fistula
INTRODUCTION
Pancreatic adenocarcinoma is an almost uniformly fatal malignancy, which usually presents in its advanced stages. It is estimated that about 5-10% of pancreatic carcinoma is associated with a family history of the disease [1, 2]. Of those, mutations in the BRCA2 gene are the most prevalent occurring, in various series, in anywhere from 5-27% of cases [3, 4].
Leptomeningeal carcinomatosis (LC) is a late manifestation of many types of solid tumors and is exceedingly rare in pancreatic cancer. We present the only case in the literature of a patient with metastatic BRCA2-associated pancreatic cancer who developed LC while undergoing treatment with a PARP inhibitor. We also present a case of BRCA1-mutationassociated pancreatic cancer with CNS metastasis that developed after treatment with cisplatin. These cases suggest the possibility that BRCA-associated pancreatic cancer, like BRCA-mutation-associated breast and ovarian cancer, may have a different natural history from sporadic cases, which may be further perturbed by treatment with DNA damaging agents, such as PARP inhibitors or platinums.
CASE REPORTS
Case #1
A forty-two-year-old woman was diagnosed in August 2012 with T2N0M0 head of pancreas adenocarcinoma, after she presented with back pain and liver function test abnormalities. Her preoperative CA19-9 was elevated to 533 ng/mL. She underwent pancreaticoduodenectomy and had an uncomplicated post-operative course, her CA19-9 declined to 16 ng/mL, and she began adjuvant treatment with gemcitabine.
She transitioned her care to our institution midway through her adjuvant treatment course. Due to her young age at the time of diagnosis and family history of a mother with breast cancer diagnosed at age 34, we referred her to our Cancer Risk Clinic for genetic counseling and BRCA1 and BRCA2 testing. She was found to have a germline, deleterious BRCA2 9631delC mutation. She completed adjuvant treatment with gemcitabine and a post-treatment CT scan showed no evidence of disease. Two months later, a follow up CT scan revealed 3 hepatic metastases and stable post-surgical changes in the pancreatic bed. Her CA 19-9 also rose and peaked at over 17,000 ng/mL before she began treatment for metastatic disease.
She refused further cytotoxic chemotherapy and began treatment on a clinical trial of a PARP inhibitor in September 2013. She initially had a favorable response to treatment with a decrease in the size of hepatic lesions and retroperitoneal adenopathy on CT imaging, and a decline in CA 19-9 to 166 ng/mL. By late February 2014, her disease progressed again in the liver and pancreatic bed.
In early March 2014 she developed headache and neck pain. A contrast-enhanced Magnetic Resonance Imaging (MRI) scan of the brain was obtained and revealed abnormal enhancement between the cerebellar folia, consistent with meningeal infiltration involving the posterior fossa (Figure 1). Lumbar puncture revealed malignant cells consistent with metastatic carcinoma. Symptoms of increased intracranial pressure rapidly progressed and palliative whole brain radiation therapy (WBRT) and high-dose steroids were initiated. She had additional clinical progression after receiving only 9 Gy of a planned 30 Gy of WBRT. She was transitioned to hospice and died on April 10, 2014 (Table 1).
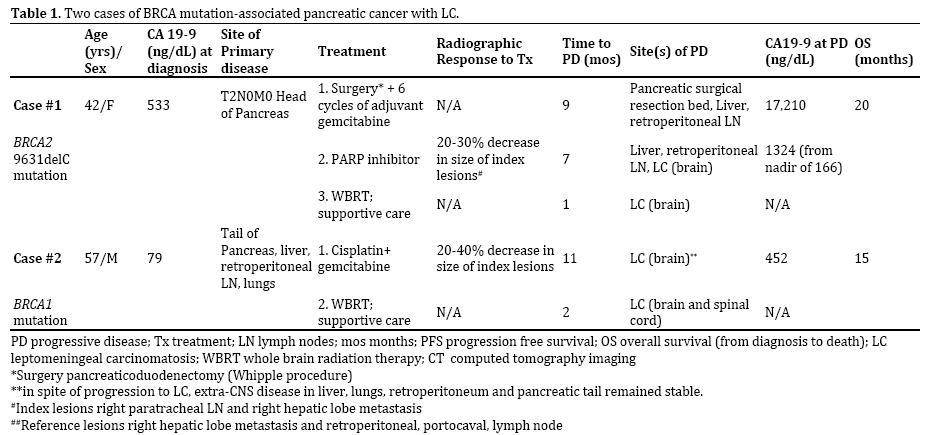
Figure 1. Axial T1 post-contrast MRI. There is notable linear enhancement
between the cerebellar folia bilaterally (white arrow).
Case #2
A fifty-seven-year-old man with known BRCA1 mutation was diagnosed with a tail of pancreas adenocarcinoma in December 2013 after presenting with persistent abdominal pain. A CT scan revealed bilobar hepatic metastasis, mesenteric and retroperitoneal adenopathy as well as small bilateral pulmonary infiltrates suspicious for metastatic disease. Biopsy of one of the hepatic lesions confirmed metastatic pancreatic adenocarcinoma. In January 2014 he began treatment with cisplatin and gemcitabine at an outside institution. Interval CT scans during the first 3 months of treatment showed disease response with decrease in size of the pancreatic tail mass, hepatic metastases, and the retroperitoneal adenopathy.
The patient completed 6 cycles of treatment and then transferred his care to our institution where he received his 7th cycle in mid-June, 2014. His disease remained stable on imaging until November 2014 when he presented with 4 days of progressive headaches. An MRI brain revealed a right temporal lobe parenchymal metastasis as well as enhancement within the cerebrospinal fluid space consistent with leptomeningeal carcinomatosis (Figure 2). Extra-CNS restaging CT scans revealed stable disease. He completed 30 Gy of WBRT in December 2014 with improvement in his headaches.
Figure 2. Axial T1 post-contrast MRI revealing a right temporal ring enhancing lesion with surrounding edema (A, white arrow) consistent with a parenchymal
brain metastasis, and linear enhancement between the cerebellar folia (B, white arrow) demonstrating disease in the cerebrospinal fluid space.
His headaches recurred in early 2015 prompting multiple Emergency Department visits and hospitalizations. In early February 2015 he complained of back pain and underwent a contrast-enhanced MRI of the cervical, thoracic and lumbosacral spine, which revealed bulky leptomeningeal disease involving his spinal cord particularly in the cervical and thoracic regions. He was transitioned to hospice care and died on March 18, 2015 (Table 1).
DISCUSSION
Leptomeningeal carcinomatosis from solid tumors is typically a late finding, but as patients live longer, it is a scenario clinicians may encounter more often. Breast cancer is the most common solid tumor associated with LC [5]. The frequency of LC from pancreatic cancer is exceedingly rare. A very limited number of cases have been reported in the literature since 1939 (Table 2). To our knowledge, these are the first reported cases of pancreatic LC in patients having known BRCA mutations.
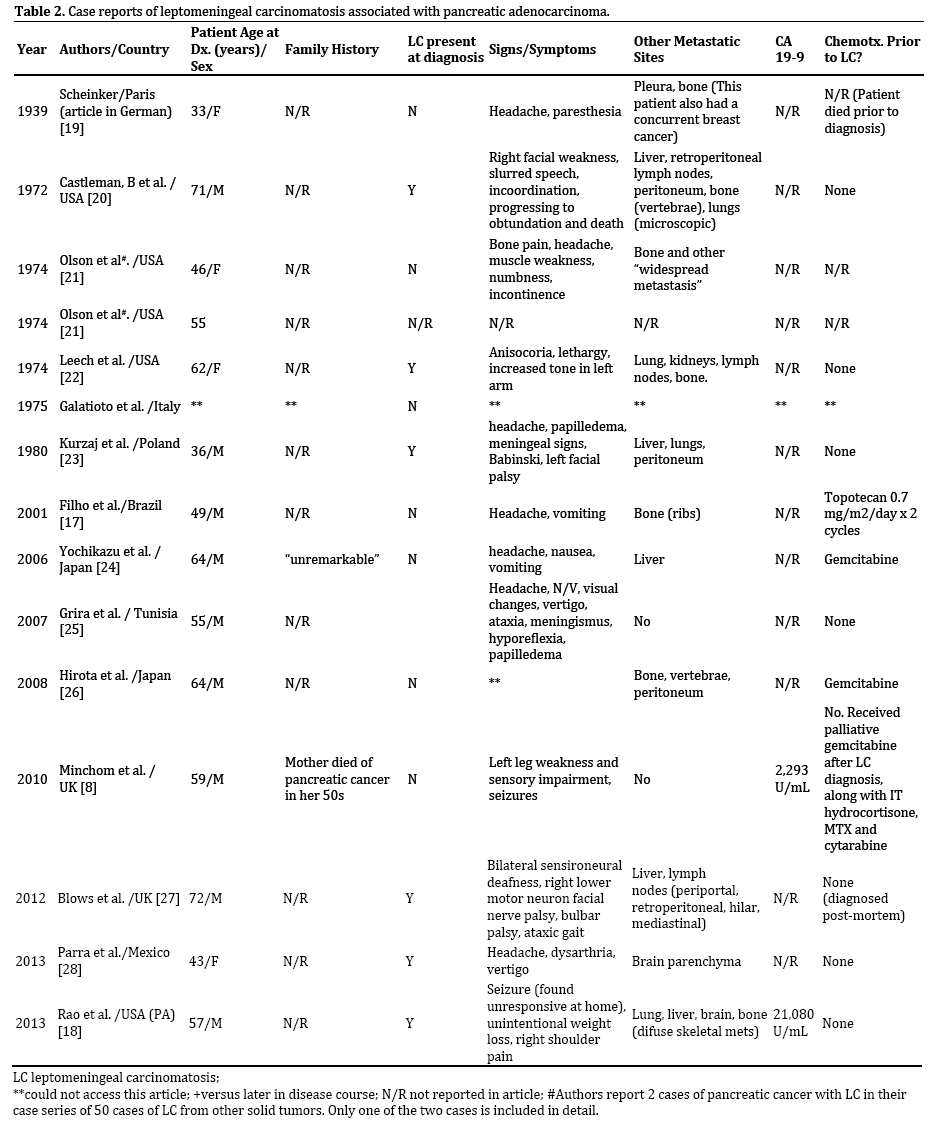
Mutations in the BRCA2 gene are the most frequently found genetic mutations associated with hereditary pancreatic cancer syndromes [2, 3, 6]. The majority of the cases of LC reported in the literature have occurred in patients under the age of 60 years, whereas the median age at diagnosis of sporadic pancreatic cancer is 71 years [7]. Where family history was reported, one patient had a first-degree relative who developed pancreatic cancer at a young age [8]. These features are strongly suggestive of an underlying hereditary syndrome however no further information about genetic testing was reported.
One possibility is that pancreatic cancer associated with a hereditary cancer risk syndrome behaves differently-has a different natural history-than sporadic cases. In breast cancer, we know that patients with deleterious BRCA1 or BRCA2 mutations tend to develop cancer at younger ages, their disease is often ER, PR, and Her2-neu negative (triple negative) and is, in some cases, faster growing [9]. One series from Scotland, investigating patterns of metastasis in ovarian cancer, found that BRCA1/2 mutationassociated ovarian cancer seemed to be associated with more visceral (as opposed to peritoneal) metastasis than sporadic ovarian cancer cases [10]. We do not yet know whether BRCA1- and BRCA2-associated pancreatic cancer will demonstrate a different biology and natural history than sporadic cases; this is an area in need of further investigation.
What many of the BRCA mutation-associated solid tumors have in common is their sensitivity to DNA damaging agents (e.g. methylating agents, topoisomerase inhibitors, platinum agents, alkylating agents and ionizing radiation). BRCA1, through phosphorylation by the ataxia telangiectasia mutated (ATM) kinase, is required for S- and G2/M-phase cell cycle arrest in response to DNA damage. It has also been shown to interact with other DNA repair proteins (e.g. RAD51, RAD50/MRE11/Nibrin complex etc.) and has a role in transcriptional regulation and cell proliferation through interactions with other proteins including the estrogen receptor (ER) [11]. BRCA2 interacts directly with RAD51 and, together with BRCA1 they form a multi-protein complex that is involved in homologous recombination and repair of double-strand DNA breaks [12]. Clinical studies have suggested that DNA crosslinks caused by platinum salts require homologous recombination (HR) to repair the DNA damage. Cancer cells that are deficient in BRCA1 or BRCA2 lack the ability to effectively repair DNA damage by this mechanism. These cells will therefore be more susceptible to agents that cause DNA crosslinks, such as platinum salts [11].
PARP-1 is an enzyme that is usually involved in gene regulation, apoptosis, DNA repair, signaling DNA damage, controlling telomere length and chromosome stability [13]. PARP inhibition prevents malignant cells from repairing damaged DNA and this class of drugs has been used both as a single agent and in combination with cytotoxic agents and ionizing radiation in an effort to enhance their activity. Because of the pronounced susceptibility of BRCA1/2- mutant tumors to PARP inhibitors, the presence of a BRCA1 or BRCA2 mutation can be used as a predictive biomarker for response to this class of drugs [5].
Given the rarity of LC from pancreatic cancer and the relative newness of PARP inhibitor use in this setting, we wondered, if the level of the PARP inhibitor that reached the CNS in Case #1 might have been inadequate to control the disease in that space. Since the patient in Case #1 had disease progression in her liver and lymph nodes concurrently with the development of LC, this is less likely. A study of the pharmacokinetics of the PARP inhibitor veliparib (ABT-888) in non-human primates found that CSF penetration was ~57% after oral administration of the drug and that CSF concentrations were within a range that would be considered therapeutic in humans [14].
Assuming adequate CSF penetration of the PARP inhibitor in Case #1, an alternate possibility is that the use of this drug changed the natural history of the disease. This is difficult to assess and is confounded by the fact that BRCA2 mutation-associated pancreatic cancer may have a different natural history, with potentially a greater propensity for CNS metastases, than sporadic cases. There is no data in the literature to suggest what biological changes may be taking place in the tumor that would change the natural history of disease. One might postulate the occurrence epigenetic changes or a secondary BRCA2 mutation developing in the tumor, which either change the natural history of the cancer or promote resistance to PARP inhibition. For example, in a study from Washington University, Norquist et al. assessed primary and recurrent ovarian carcinomas with BRCA1/2 mutations, to determine the frequency of secondary mutations in patients who had developed resistance to platinum chemotherapy and PARP inhibitors. Secondary mutations restoring BRCA1/2 function occurred in 28.3% (13/46) of their patients with recurrent carcinomas and were found in 50% (3/6) patients with platinum-resistant recurrent ovarian carcinoma who were treated with PARP inhibitors [15]. No further biopsies were performed in Case #1 after her disease progression, so such an assessment could not be made.
Skeletal metastasis is another rare finding in pancreatic cancer, occurring from 2-20% of cases in the literature [16]. It is intriguing that in two case reports of pancreatic cancer patients with CNS metastasis, bone metastases were also present in addition to other visceral sites (liver, lung, lymph nodes) [17, 18]. The finding of two rare, late findings in these small case series suggests that the biology of the disease in these patients might be different from other cases of pancreatic adenocarcinoma, which tend to travel to liver, lung, and peritoneum. Such a difference might be attributable to the genetics of the disease-supported by the young age of the patients (in most cases)-and, occasionally, but not in all cases, longer survival due to better chemotherapy and supportive care.
CONCLUSION
Leptomeningeal carcinomatosis from pancreatic cancer is rare. As a late finding, it is possible that it will become more common if patients with pancreatic cancer live longer as we develop better therapies for metastatic disease. It is striking that many of the cases in the literature occurred in patients under age 60 years, suggesting the possibility of an underlying hereditary cancer susceptibility syndrome. With time and further investigation we may begin to understand more about the natural history of BRCA mutation-associated pancreatic cancer. Further study will also elucidate how to integrate therapy with PARP inhibitors and other DNA-damaging agents into our treatment strategy to optimize outcomes.
Conflict of Interest
The authors declare that they have no competing interests.
References
- Hidalgo, M. Pancreatic Cancer. NEJM 2010; 362(17):1605-17. [PMID: 20427809]
- Alsina, J and Thayer, P. Hereditary Pancreatic Cancer. In D.C. Chung and D.A. Haber (eds.) Principles of Clinical Cancer Genetics: A Handbook from the Massachusetts General Hospital. 2010; ch. 7. P. 89-96
- Habbe N, Langer P, Sina-Frey M, Bartsch D. Familial Pancreatic Cancer Syndromes. Endocrinol Metab Clin N Am 2006; 35:417-430. [PMID: 16632103]
- Hall M, Dignam J, Olopade O. Family History of Pancreatic Cancer in a High-Risk Cancer Clinic: Implications for Risk Assessment. J Genet Counsel 2008; 17:365-372. [PMID: 18581219]
- Kak M, Nanda R, Ramsdale EE, Lukas RV. J Clin Neurosci 2015; 22:632-637. [PMID: 25677875]
- O’Sullivan C, Mooh D, Kohn E and Lee J. Beyond breast and ovarian cancers: PARP inhibitors for BRCA mutation-associated and BRCA-like solid tumors. Front Oncol 2014; 4(42):1-13. [PMID:24616882]
- SEER Stat Fact Sheets: Pancreas Cancer https://seer.cancer.gov/statfacts/html/pancreas.html
- Minchom A, Chan S, Melia W, Shah R. An Unusual Case of Pancreatic Cancer with Leptomeningeal Infiltration. J Gastrointest Canc 2010; 41:107-109. [PMID: 20069465]
- Heijnsdijk E, Warner E, Gilbert F, Tilanus-Linthorst MM, Evans G, Causer PA, et.al. Differences in Natural History between Breast Cancers in BRCA1 and BRCA2 Mutation Carriers Effects of MRI Screening-MRISC, MARIBS, and Canadian Studies Combined. Cancer Epidemiol Biomarkers Prev 2012; 21(9):1458-1468. [PMID: 22744338]
- Gourley C, Michie C, Roxburg P, Yap TA, Harden S, Paul J, et. al. Increased Incidence of Visceral Metastasis in Scottish Patients with BRCA1/2-Defective Ovarian Cancer: An Extension of the Ovarian BRC Aness Phenotype. JCO 2010; 28(15):2505-11. [PMID: 20406939]
- Bayraktar, S and Gluck, S. Systemic therapy options in BRCA mutation-associated breast cancer. Breast Cancer Res Treat 2012; 135:355-366. [PMID: 22791366]
- Zhang, H, Tombline, G and Weber, B. BRCA1, BRCA2 and DNA Damage Response: Collision or Collusion? Cell 1998; 92:433-436. [PMID:9491884]
- Lee J, Lederman J and Kohn E. PARP Inhibitors for BRCA1/2 mutation-associated and BRCA-like malignancies. Annals of Oncol 2014; 25(1):32-40. [PMID:24225019]
- Muscal J, Thompson P, Giranda V, Dayton BD, Bauch J, Horton T, et.al. Plasma and cerebrospinal fluid pharmacokinetics of ABT-888 after oral administration in non-human primates. Cancer Chemother Pharmacol 2010; 65:419-425. [PMID: 19526240]
- Norquist B, Wurz K, Pennil C, Garcia R, Gross J, Sakai W, et. al. Secondary Somatic Mutations Restoring BRCA1/2 Predict Chemothearpy Resistance in Hereditary Ovarian Carcinomas. JCO 2011; 29(22):3008-15. [PMID: 21709188]
- Borad M, Saadati H, Lakshmipathy A, Campbell E, Hopper P, Jameson G, et.al. Skeletal Metastases in Pancreatic Cancer: A Retrospective Study and Review of the Literature. Yale Journal of Biology and Medicine 2009; 82-1-6. [PMID: 19325940]
- Filho A, Cardoso F, Leo A, Awada A, da Silva VD, Tovar RB, et. al. Carcinomatous Meningitis as a Clinical Manifestation of Pancreatic Carcinoma. Annals of Oncology 2001; 12:1757-59. [PMID: 11843255]
- Rao R, Sadashiv S, Goday S and Monga D. An Extremely Rare Case of Pancreatic Cancer Presenting With LeptomeningealCarcinomatosis and Synchronous Intraparenchymal Brain Metastasis.IntSoc of Gastrointest Oncol 2013; 6(3):90-92. [PMID: 23936550]
- Scheinker, I. ZurPathologie und klinischenSymptomatologie der diffusenKarzinomatose der Meningen. Mschr Psychiat Neurol 1939; 101:275-290.
- Castleman, B., Scully R.E., McNeely B.V. Case 12-1972-Chest Pain with Abnormal Brain and Liver Isotope Scans. Case Records of the Massachusetts General Hospital. Weekly Clinicopathological exercises. NEJM 1972; 286:650-656.
- Olson M, Chernik N, Posner J. Infiltration of the Leptomeninges by Systemic Cancer: A clinical and Pathologic Study. Arch Neurol 1974; 30:122-137. [PMID: 4405841].
- Leech R, Welch F, Ojemann G. Subdural Hematoma Secondary to Metastatic Dural Carcinomatosis. J Neurosurg. 1974; 41:610-613. [PMID: 4425200]
- Kurzaj E, Kopczynski S, Barowska-Lehman J, Ludwiczak R, et.al. Subdural Haematoma associated with Dural Carcinomatosis in a Patient with Primary Carcinoma of the Pancreas. Neurochirurgia 1980; 23:13-17. [PMID: 7352044]
- Yagi Y, Nishimura Y, Nakatsugawa S, Fukuoka T, Hirota M, Okamoto K, et al. A case of meningeal carcinomatosis from pancreatic cancer during chemotherapy using gemcitabine. Jpn J Gastroenterol Surg 2006; 39:1683-88.
- Grira M, Jemaa H, Lammouchi T, and Benammou S. Meningitis Revealing Pancreatic Carcinoma. Neurosciences 2007; 12(3):256-258. [PMID: 21857581].
- Hirota, M, Yagi, Y, Yamashita, K, Okamoto, K, Sato, T, Ichihara, T. [A long survival case of unresectable pancreatic cancer by chemotherapy with gemcitabine as the key drug] (Article translated from Japanese). GanTo Kagaku Ryko 2008; 35:2413-16. [PMID: 19098414]
- Blows S, Morgan R, Dhariwal U, Petts G, Roncaroli F, et.al. Pancreatic Adenocarcinoma Presenting with Sudden Onset Bilateral Deafness Secondary to Metastatic Leptomeningeal Infiltration. Age and Ageing 2012; 0:1-2. [PMID: 22743150]
- Parra V, Agudelo N, Calderon M. [Pancreatic ductal adenocarcinoma with brain metastases]. Acata Neurol Colomb 2013; 29:118-123.



