Pollo-Flores P1*, Cásseres DL1, Zampier L1, Adnet GCFS1, Shiroma ME1,Padua L1, Delvaux N2,Villar LM2 and Porto LC3
1Fluminense’s Federal University, Internal Medicine Division, Rio de Janeiro, Rio de Janeiro, Brazil
2Oswaldo Cruz’s Foundation, FIOCRUZ,Brazil
3Rio de Janeiro’s State University, HLA Laboratory, Brazil
Corresponding Author:
Priscila Pollo-Flores
Fluminense’s Federal University, Internal Medicine Division, Rio de Janeiro, Rio de Janeiro, Brazil.
E-mail: priscilapollo96@gmail.com
Received date: December 30, 2015; Accepted date: January 02, 2016; Published date: January 11,2016
Citation: Pollo-Flores P, Cásseres DL, Zampier L, et al. Lipid Metabolism and Interleukin 28B Polymorphism in Hepatitis C. J Infec Dis Treat. 2016, 2:1. doi: 10.21767/2472-1093.10007
Keywords
Hepatitis C; Lipid Metabolism; Interleukin 28B polymorphisms
Introduction
Approximately 170 million people, 3% of the world population, have infection with hepatitis C virus (WHO) [1] . Liver cirrhosis and hepatocellular carcinoma are the most important complications of this infection. Thus, early diagnosis and treatment are the best strategy to avoid these consequences. The polymorphism of IL- 28B was recognized as a powerful host predictor of the therapeutic response. Likewise, the cholesterol level is associated with the polymorphism of IL28B and is related to the treatment sucess [2], evidenced by Fabrics [3]. The gene that encodes interleukin 28B, also known as Type III Interferon Lambda (IFN-λ3) also constitutes a chemical messenger of immune reactions and has antiviral activity (related to the cytokine interferon alpha. In the vicinity of this gene were found some single nucleotide polymorphisms (SNP) [4] which constitute the naturally occurring genetic alterations in the population and are statistically significantly correlated with interpersonal differences with regard to different aspects of the phenotype, such as, e.g. in response to a therapeutic measure. Recently, a genome-wide association study (GWAS) [4] evaluated more than 1,600 individuals chronically infected with hepatitis C treated with pegylated interferon alpha and ribavirin. The clinical trial identified the rs12979860, a SNP (SNP) on chromosome 19q13, which was strongly associated with sustained virologic response (SVR) to treatment with interferon and ribavirin.
The SNP are the exchange of a base in well located points of our DNA. Different SNP in this region of chromosome 19 is located where the polymorphism of IL28B are under investigation and show promise in its relationship with therapeutic response of HCV infection and even spontaneous clearance, in patients who achieve healing without treatment, especially in acute hepatitis. There are three genotypes well characterized for gene IL28B rs12979860 C/C, C/T and T/T. It is well established that when a person has the C/C genotype in that position in the genome, has a greater chance of spontaneous clearance of the virus when compared to individuals C/T and T/T [4]. Most striking differences were observed in an analysis of genotype frequencies by Thomas et al. [5] where patients with the C/C genotype were three times more likely to eliminate the HCV genotypes patients compared to C/T and T/T combined. The proportion of subjects C/T or T/T, which cleared the virus (28% when combined the two genotypes), was similar to "general public", since the elimination of HCV occurs in approximately 30% of the general population [6]. In contrast, the elimination of HCV was seen more frequently than in the general population ratio when the C/C group was considered, reaching 53% [6]. Recently, Everhart et al. [7] demonstrated that GGT levels are strongly associated with rs12979860 polymorphism. Patients with at least one copy of the T allele had a poorer virological response with increased GGT. These results point to the existence of different predictors of virologic response, besides those already studied in patients with different rs12979860 genotypes.
Lipoproteins regulates mechanism of viral entry into hepatocytes as well as replication and secretion. Furthermore, the HCV circulates in the blood combined with lipoproteins, which possibly camouflages the virus from the host immune response, and may in turn promote viral entry into hepatocytes. The LDL receptor (LDLr) is a membrane glycoprotein that controls the main pathway through which cholesterol enters cells [8]. This contains a single copy of apolipoprotein B-100 (ApoB100) and transports 65-70% of plasma cholesterol. The hepatitis C virus (HCV) interacts with these lipid receptors for entry into cells. More recent studies suggest that LDL receptor pathway involves non-productive HCV entry into the cell, and then the virus is degraded. On the other hand, another SRB1 lipoprotein receptor participates in virus entry into the cell via a pathway that favors viral replication. HDL favors virus entry into the cell and oxidized LDL inhibits [8,9].
The cholesterol levels, metabolic derrangements and anti oxidants substances like resveratrol are envolved in liver fibrosis and hepatitis C process. Resveratrol may enhance lipid metabolism and reduce LDL oxidation [10] like zinc and functional food elements, other scavenger molecules. The nutraceuticals can develop role in differents biochemicals pathways of lipid metabolism and even overcome genetic variabilities in the future [11].
The only genetic predictor of cholesterol and triglycerides levels with genotype 1 chronic hepatitis C is the interleukin 28B polymorphisms [12]. This is true in context of pre treatment but not after treatment in responders. In this way, is clear that hepatitis C virus has a role in lipid metabolism [12]. The LDL-c is more associated with response when the genotype for IL 28 B is heterozygous. The low triglyceride level and high LDL level were associated with therapy response [13]. Results showed that in vitro [8] HCV infection induces expression of lipid metabolism genes depending on the viral genotype. These results demonstrate that the IL28B genotype influences the lipid metabolism in patients with HCV, but not in uninfected individuals and appears to be mediated by the viral genotype. The LDL-C serum higher was significantly associated with SVR in patients heterozygous for the IL 28B (p<0.001) in study and was not associated in homozygotes [3]. Moreover, more recent studies have pointed out that the level of cholesterol can also be a non-invasive marker of liver fibrosis [3] and help to evaluate pretreatment therapeutic response chance. The liver fibrosis markers are related to the stage of cirrhosis and can predict standard treatment sucess for hepatitis C.Nowadays, the advent of new drugs in the armamentarium of hepatitis C places pegylated IFN and ribavirin in secondary roles for the treatment of the infection. However, new schemes are costly, are not available worldwide for all patients and the prospect of individualized treatment is essential. Furthermore, extrahepatic manifestations of viral infection and associations with other diseases such as fatty liver and diabetes mellitus need to be better understood.
Materials and Methods
This is a prospective study of patients with chronic hepatitis C, genotype 1. Patients were invited to participate in the study in the clinic of the University Hospital Antônio Pedro (HUAP) of the Federal Fluminense University (UFF) in Niterói, Rio de Janeiro, from August 2012 to March 2013. The study was conducted in accordance with the Declaration of Helsinki (2001) and after approval by the local Ethics Committee. All patients signed the informed consent. Inclusion criteria were (1) PCR-RNA hepatitis C virus positive through sensitive method (>15 UI/ml) for viral quantification (COBAS Taqman assay, USA), (2) aged between 18 and 75 years. Exclusion criteria were (1) Cirrhosis Child-Pugh B and C, decompensated cirrhosis, presence of changed laboratory parameters like albumin, prothrombin time and bilirrubin; (2) Use of statins in the last year; (3) Pregnancy; (4) co-infection with HIV and disagreement with the informed consent.
Patients underwent blood sampling in State of Rio de janeiro universitary’s hospital (HLA-UERJ) or at Antônio Pedro’s Federal Universitary Hospital (forwarded for the Oswaldo Cruz’s Institute of research), after fasting for DNA extraction from peripheral blood and genotyped by specific primers (PCR). The single nucleotide polymorphism rs 12979860 (SNP) was studied. Blood samples for total cholesterol and LDL-cholesterol dosage was held in the biochemistry laboratory of Antônio Pedro’s Federal Universitary Hospital by enzymatic/colorimetric method.
Statistical analysis
Graphs were plotted using Graphpad Prism software 5.0 (GraphPad Software, Inc., La Jolla, California, USA) using one-way Anova test with Bonferroni post test. Qualitative analyses were made by Fischer’s test. Multivariate analyses were not undertaken because the relatively small number of cases. Statistical significance level adopted was 0.05. P value was 2-sided evaluated.
Results and Discussion
Fifty-three patients underwent the examination of polymorphism of IL 28B. 15 male (28%) and 38 female (72%). Fifteen patients had liver biopsy in the last year from the study. The baseline characteristics are exposed in Table 1. The mean age was 53 years (± 11 years) (Table 1). The distribution of the polymorphism performed according to the given Figure 3.
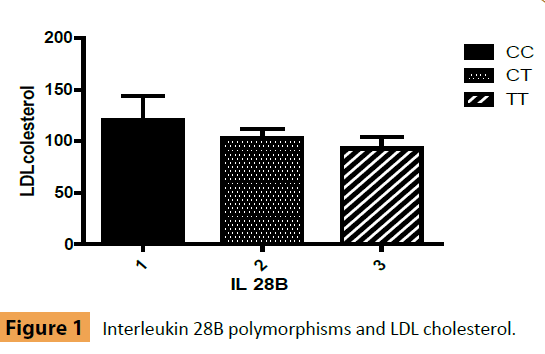
Figure 1: Interleukin 28B polymorphisms and LDL cholesterol.
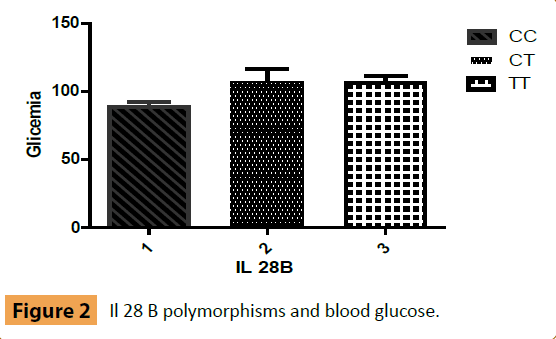
Figure 2: Il 28 B polymorphisms and blood glucose.
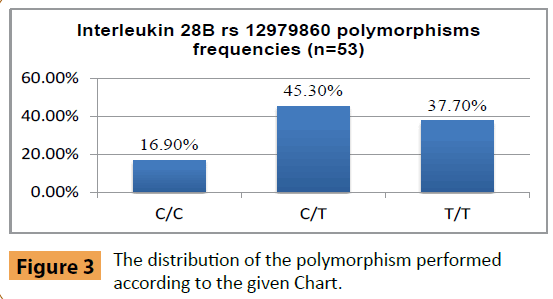
Figure 3: The distribution of the polymorphism performed according to the given Chart.
| Number |
53 |
| Age(med ± SD)-years |
54(±12) |
| Sex (% male) |
15(28%) |
| Glycemia (med ± SD)-mg/dl |
102 (±21) |
| LDL Cholesterol (med ± SD) - mg/dl |
100 (±31) |
Significative Fibrosis
(Metavir Score F2) n |
9 |
Advanced Fibrosis
(Metavir Score F3) n |
6 |
| Viral load (U/ml) >600.000 n(%) |
9(17%) |
| GGT(gama-glutamiltranspeptidase) median(min/máx) – U/L |
90(19/3775) |
| The mean age was 53 years (±11 years). |
Table 1: Baseline characteristics of patients enrolled.
The mean LDL-cholesterol was 121 (± 46) mg/dl for the polymorphism group with C/C; 104 (± 24) mg/dl in the polymorphism group with C/T and 93 (± 33) mg/dl in T/T group. There was no statistical significance between the groups (p=0.38). Regarding the level of LDL pre treatment in these patients, the data of 26 patients (n=26) were analyzed, 17 (65.4%) LDL <110 (44-117) and 9 (34.6%) LDL ≥ 110 (117-154). The figure below shows the correlation between the rs12979860 polymorphism of IL 28B and LDL-C levels (Figure 1). The average blood glucose was 88 (± 10) mg/dl for patients with polymorphism of IL 28B CC; 109 (± 24) mg/dl for patients with IL 28B CT and 106 (± 14) mg/dl in patients Il 28B polymorphism with TT (Figure 2). The p was found to be 0.07.
Studies show that the polymorphism of rs12979860 IL28B, previously associated with response to treatment of hepatitis C, also has a dramatic impact on the natural elimination vírus [4]. He is now a priority to determine the mechanisms by which the IL28B promotes viral host defense. Also, determine the range of the virus possibly affected by these mechanisms. In our sample, the results indicated a higher prevalence of C/T genotype relative to T/T and C/C of interleukin 28B, constituting, at most, weak responders to treatment with pegylated interferon and ribavirin. The lower levels of LDL-C in genotypes C/T and T/T when correlated with C/C genotype did not acquired statistical significance. LDL-C is an HCV marker of the envolvement on lipid metabolism mediated by host mechanisms. In the literature, the best performance for LDL-C as a predictor of response in hepatitis C therapy is the heterozygous genotype for IL28B [3]. There was a significant increase in cholesterol after treatment in sustained virologic responders and there was no difference in non responders [14]. The comprehension of the relationship between lipoproteins and viral kinetics can help to better tailor treatment in the future.
The arrival of protease and polymerase inhibitors increased greatly the response rate in hepatitis C liver cirrhosis but 10% of patients develops this final complication despite treatment with more fibrosis and cirrhosis decompensation needing liver transplantation. Thus, cholesterol levels could be useful to detect, in conjunction with other tests, the best drug for each case. The interleukin 28B also increases valuable information in the 3D regimen in cirrhotic that include paritaprevir/r/ombistavir/ dasabuvir [15]. The Il 28 B TT results in negative predictive value of sustained virologic response [16].
The advent of new treatments without interferon is a revolution in the treatment of viral hepatitis C but also put into perspective a new group of difficult to treat patients, which have genotype 3 infection. In genotype 3 the steatosis doesn’t interfere with response but with viral load [14]. This is precisely the one in which lipid metabolism is most prominently changed. New drugs is still needed for this patients with genotype 3 hepatitis C cirrhosis [15].
The steatosis could be one of the factors responsible for lower performance of direct antiviral drugs in hepatitis C in genotypes 1, 2, 4, 5 and 6 [9]. This is one of the limitations of our study because we didn’t study others genotypes like genotype 3 hepatitis C patients. Probably, in hepatitis C genotype 3 patients the mechanism of steatosis is different since the serum cholesterol level is lower and the viral load is frequently higher than in genotype 1. In sustained virologic responders, with genotype 3, the steatosis decreases or disappears and the lower serum cholesterol is corrected for baseline level [14]. The mechanism of steatosis is viral dependent. In genotype 1, the metabolic factors are responsible for steatosis in the majority of cases [14]. The treatment now allows more than 90% of response in genotype 1 but the lenght of treatment is not completely defined for cirrhotic patients [15]. In this way, steatosis may be a point to be considered. Similarly, drug resistance and genotypic characteristics should be further considered.
Hepatitis C was associated in a study with atherosclerotic disease through chronic inflammation and liver fibrosis. The endothelial dysfunction is a starting point to many hepatitis C consequences like fibrosis. Therefore, this issue deserves more researchs [17-19]. Another point to be considered in our study is the sample size. The small sample size does not allow definitive conclusions and should be taken in consideration for further studies.
The infection of hepatitis C has characteristically extrahepatic manifestations and association with diseases such as nonalcoholic fatty liver and diabetes mellitus type 2, which are prevalent, characterizing the fast fibrosing patients and deserve in-depth studies on the relationship with this virus and evolution of liver fibrosis.
Conclusion
In conclusion, the managing of patients with hepatitis C infection can be improved with the better understanding of factors related with steatosis and lipid metabolism.
References
- Lavanchy D (2011) Evolving epidemiology of hepatitis C virus. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases17:107-15.
- McCarthy JJ, Li JH, Thompson A(2010)Replicated association between an IL28B gene variant and a sustained response to pegylated interferon and ribavirin. Gastroenterology 138:2307-14.
- Fabris C, Falleti E, Cussigh A (2012) The interleukin 28B rs12979860 C/T polymorphism and serum cholesterol as predictors of fibrosis progression in patients with chronic hepatitis C and persistently normal transaminases. Journal of medical virology84:747-55.
- Ge D, Fellay J, Thompsaon AJ(2009) Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature461:399-401.
- Thomas DL, Thio CL, Martin MP(2009) Genetic variation in IL28B and spontaneous clearance of hepatitis C virus. Nature461:798-801.
- Tillmann HL, Thompson AJ, Patel K(2010) A polymorphism near IL28B is associated with spontaneous clearance of acute hepatitis C virus and jaundice. Gastroenterology139:1586-92, 92 e1.
- Everhart JE, Wright EC (2013) Association of gamma-glutamyltransferase (GGT) activity with treatment and clinical outcomes in chronic hepatitis C (HCV). Hepatology57:1725-33.
- Rojas A, del Campo JA, Maraver M(2014) Hepatitis C virus infection alters lipid metabolism depending on IL28B polymorphism and viral genotype and modulates gene expression in vivo and in vitro. Journal of viral hepatitis21:19-24.
- Barth H, Liang TJ, Baumert TF (2006) Hepatitis C virus entry: molecular biology and clinical implications. Hepatology 44:527–535.
- Chen Q, Wang E, Ma L (2012) Dietary resveratrol increases the expression of hepatic 7alpha-hydroxylase and ameliorates hypercholesterolemia in high-fat fed C57BL/6J mice. Lipids in Health and Disease 11: 56.
- Scicchitano P, Cameli M, Ciccone MM (2014) Nutraceuticals and dyslipidaemia: Beyond the common therapeutics. Journal of functional foods 6: 11-32.
- Clarck PJ, Thompson AJ, Zhu M(2012) Interleukin 28B polymorphisms are the only common genetic variants associated with low-density lipoprotein cholesterol (LDL-C) in genotype-1 chronic hepatitis C and determine the association between LDL-C and treatment response. J Viral Hepat 19: 332-340.
- Ramcharran D, Wahed AS, Conjeevaram HS(2010) Associations between serum lipids and hepatitisC antiviral treatment efficacy. Hepatology52: 854-863.
- Poynard T, Ratziu V, McHutchison J(2003) Effect of treatment with peginterferon or interferon alfa-2b and ribavirin on steatosis in patients infected with hepatitis C. Hepatology 38:75-85.
- Ferenci P, Kozbial K, Mandorfer M, Hofer H (2015) HCV targeting of patients with cirrhosis. Journal of Hepatology 63: 1015-22.
- Harrison SA, Rossaro L, Hu KQ(2010) Serum cholesterol and statin use predict virological response to peginterferon and ribavirin therapy. Hepatology52:864-874.
- Fried MW, Forns X, Reau N, Wedemeyer H, Shiffman ML(2014) TURQUOISE-II: regimens of ABT450/r/ombitasvir and dasabuvir with ribavirinachieve high SVR12 rates in HCV GT1 infected patients with cirrhosis,regardless of baseline characteristics. Hepatology60:238A.
- Barone M, Vigiiani MT, Scicchitano P, Ciccone MM(2015) Endothelial Dysfunction Correlate s with Liver Fibrosis in chronic HCV infection. Gastroenterol Res Pract68: 2174.
- Patton HM, Patel K, Behling C(2004) The impact of steatosis on disease progression and early and sustained treatment response in chronic hepatitis C patients. Journal of Hepatology40:484-90.

