Keywords
Coronary artery disease; Lipoprotein(a); Meta-analysis; Prognostic value; Cardiovascular risk factors
Abbreviations
ASCVD: Arteriosclerosis Cardiovascular Disease; AIS: Acute Ischemic Stroke; CAD: Coronary Artery Disease; CI: Confidence Interval; CVD: Cardiovascular Diseases; HDL-C: Low Level High-density Lipoprotein Cholesterol; HR: Hazard Ratio; LDL-C: Low-density Lipoprotein Cholesterol; Lp(a): Lipoprotein (a); OxPL: Oxidized Phospholipids; SE: Standard Error; TC: Triglycerides
Introduction
Lipid disorders are always divided into 4 categories: elevated level low-density lipoprotein cholesterol (LDL-C), low level highdensity lipoprotein cholesterol (HDL-C), elevated triglycerides (TC), and elevated lipoprotein(a) [Lp(a)]. Elevated Lp(a) in the 4 types’ lipid disorders was rarely studied in the past decades. However, Lp(a) was an emerging marker for assessing the residual risk of cardiovascular diseases in recent year. Precious studies had proved Lp(a) was a risk factor for ischemic stroke [1-3], but the predictive value remained controversial in CAD prognosis.
In 1963, Berg firstly found Lp(a) in human plasma. Lp(a) is composed of an LDL-like particle in which Apo(B) is covalently bound by a single disulfide bond to apolipoprotein(a), and is highly homologous to plasminogen. There is extensive Apo(A) protein size heterogeneity, with >40 different isoforms, and >40 different sizes of Lp(a) particles, which is a unique occurrence unlike other circulating proteins [4].
Circulating Lp(a) levels primarily depend on the LPA gene locus, and is not affected by diet and environment. The site of Lp(a) production has not been confirmed, and may be synthesized in hepatocytes, disse space or plasma compartment [5]. The steps contain that Apo(A) dock to LDL, and then form a covalent disul?de bond between KIV-9 of Apo(A) and Apo(B) of LDL. Lp(a) metabolism is different from LDL which stays longer in plasma than LDL. But the mechanisms which Lp(a) is cleared from plasma remain controversial, maybe relate to the numbers of LDLR.
Lp(a) lacks of sufficient evidence for physiological effects, presumable physiological effects including: repairing damaged vascular system and negative regulation of angiogenesis. In pathological condition, Lp(a) carries LDL particles with all of risk of atherosclerosis, including their propensity to oxidize after entry into the vessel wall, creating highly immunogenic and oxidized LDL. Apo(A) potentiates athero-thrombosis through other mechanisms, and potential anti-?brinolytic effects by inhibiting plasminogen activation [6].
Elevated Lp(a) mediates myocardial infarction (MI), stroke, and peripheral arterial disease (PAD). In the last decade, the role in the underlying pathophysiology of arteriosclerosis cardiovascular disease (ASCVD) has been fully studied. Zhang et al. [7] conducted a clinical trial and aimed to analysis the relationship between acute ischemic stroke (AIS) and Lp(a) levels, and to determine the prognosis value for predicting the functional outcome. The results showed that there was an increased risk of unfavorable outcome associated with Lp(a) levels 300 mg/L, and Lp(a) could be considered as an independent short-term prognostic marker. It also found that there was a relatively relationship between Lp(a) and ischemic stroke in children [8]. But the role of Lp(a) in CAD remained uncertain [9,10]. Therefore, this meta-analysis summarized current evidence on Lp(a) and CAD, and further analyzed the effect of age and detection methods.
Materials and Methods
Literature search and selection of studies
The electronic databases of PubMed and ScienceDirect were searched systematically in August 2018 without time limitation. The search strategy was performed by two independent readers (Yang Lan and Xiaoxiao Zhao), using the following keywords (“lipoprotein a” OR “lipoproteins “AND “coronary artery disease”).
Studies were eligible if they met the following criteria: (1) The study determined the relationship between Lp(a) levels and CAD events; (2) All studies must be prospective study and provide hazard ratio (HR) and 95% confidence interval (CI); (3) The sample size of each study was greater than 100; (4) Including either subjects chosen from the general population, with established cardiovascular disease (CHD, cerebrovascular or carotid disease, or peripheral artery disease) or hyperlipidemia; (5) The studies must be published in English with full-text paper available.
Data extraction
The papers selection and data extraction were accomplished independently by two reviewers. If the results provided are analyzed by both univariate and multivariate methods, we chose the latter. The extracted data included: Year of publication; first author; the journal of publication; following-up periods; sample size; number of CHD events; age and sex; technique of Lp(a) measurement; hazard ratio;95% confidence interval.
Assessment of study quality
We used the standard Newcastle-Ottawa quality assessment scale to assess the Quality of all the studies. Newcastle-Ottawa scale [11] consisted of 3 factors: patient selection, comparability of the study groups, and assessment of outcome. Numbers from 0 to 9 (labeled as stars) represent different quality of each article. Cohort studies achieving 6 or more stars were considered to be of high quality.
Statistical analysis
In the study, the data was extracted into the EXCEL form, and then we used the stata version 12.0 ?12.0 for Win, Stata Corp, College Station, TX, USA?to analyze. We extracted HR and 95% CI for each study, and HR was logarithmically transformed. Log HR was used to evaluate the relationship between Lp (a) and CAD events. We hypothesized that the heterogeneous maybe represent, and used random effects model for analysis. Random effects model was better suitable for a higher degree of heterogeneity. The prediction interval helped to estimate the range of real therapeutic effects in heterogeneous environments [12]. According to the Cochrane Handbook, Q and I2 statistical indicators were used to analyze literature heterogeneity [13]. When p >0.05 or I2 <50%, the fixed effect model could be performed, otherwise, using the random effects model. If there was significant heterogeneity in the given analysis, we adjusted for the type of literature and sample size to research for the source of heterogeneity. Finally, Egger test was used to analyze the potential publication bias.
Results
Search results
The selected studies were researched in two electronic databases (Figure 1). According to the prior search strategy, 1077 literatures were researched on PubMed, and 1202 literitures were searched in ScienceDirect. After reading the literature titles and abstracts, a total of 51 articles were selected for further study. We excluded 43 articles after reviewing the full text, the reasons including: duplicates; case report or cross-sectional study; the results without hazard ratios; the small sample size; study population repeatedly. Finally, 8 studies with 86808 patients met our inclusion criteria, and were performed for meta-analysis [4,14-20]. The mean follow-up period of all eligible studies ranged from 2 years to 20 years, and the quality of the studies assessed by the Newcastle- Ottawa quality assessment scale was about 6 scores?the detailed characteristics of all studies were summarized in Table 1.
| Time |
First Author |
Follow-up Period (year) |
Numbers (CHD/total) |
Male/female |
Age |
Measurement of Lp(a) |
| 2006 |
Danik |
10 |
934/27791 |
0/27791 |
54.2 ± 7.1 |
immunoturbidimetric assay |
| 2009 |
Kamstrup |
16 |
599/8637 |
3335/5302 |
55 ± 17 |
-------------- |
| 2010 |
Florance |
10 |
635/9711 |
------- |
55.3 ± 2.93 |
double-antibody enzyme-linked immunosorbent assay technique |
| 2011 |
Lamon-Fava |
12.3 |
145/2890 |
1328/1562 |
------- |
immunoturbidimetric assay |
| 2012 |
Viranic |
20 |
1292/5777 |
5777/13318 |
53 |
double-antibody enzyme-linked immunosorbent assay technique |
| 2012 |
Viranic |
20 |
753/7541 |
7541/13318 |
54 |
double-antibody enzyme-linked immunosorbent assay technique |
| 2012 |
Gurdasani |
15 |
2365/18720 |
8381/10339 |
59.2 ± 9.2 |
immunoturbidimetric assay |
| 2018 |
Dai |
3.3 |
166/1602 |
1077/522 |
62.4 ± 10.6 |
Immunoturbidimetric assay |
| 2018 |
Gregory |
2.4 |
1146/4139 |
3328/811 |
63 ± 10/60 ± 9 |
Immunoturbidimetric assay |
Table 1: Clinical basic characteristics of the eligible articles.
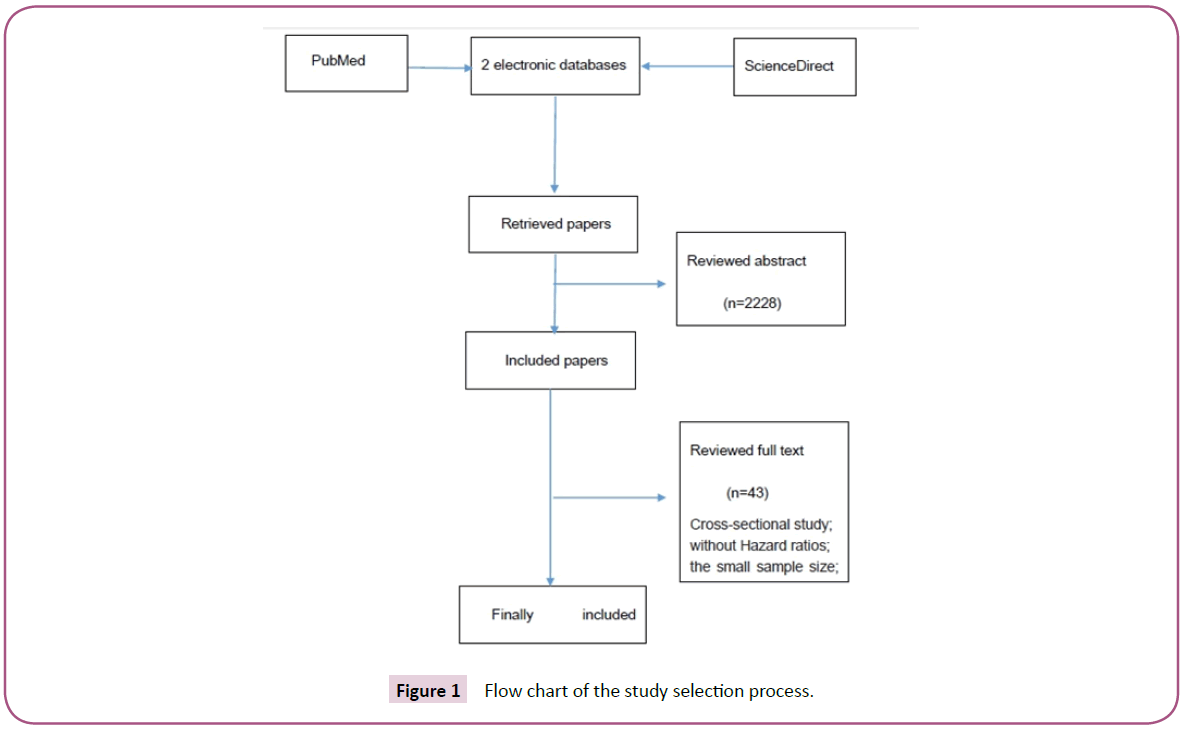
Figure 1: Flow chart of the study selection process.
Prospective cohort studies
A total of 86808 participants and 8180 subjects with CAD in 8 prospective cohort studies were eligible for final analysis. These studies included different large scale populations, and the research methods were different. Six in eight studies reported that Lp(a) levels are closely related to CAD events. The metaanalysis results showed that the elevated Lp(a), the greater the CAD risk, and the pooled adjusted HR was 1.132 (95% CI, 1.063- 1.204, p=0.000; (Figure 2). We created a funnel plot Figure 3 and performed an Egger test with a regression intercept of 3.19 (p=0.015), indicating potential publication bias in the meta-analysis. High heterogeneity was also observed (Q=25.74; I2=68.9%; p=0.001). Then we conducted a subgroup analysis to explore factors that affect heterogeneity.
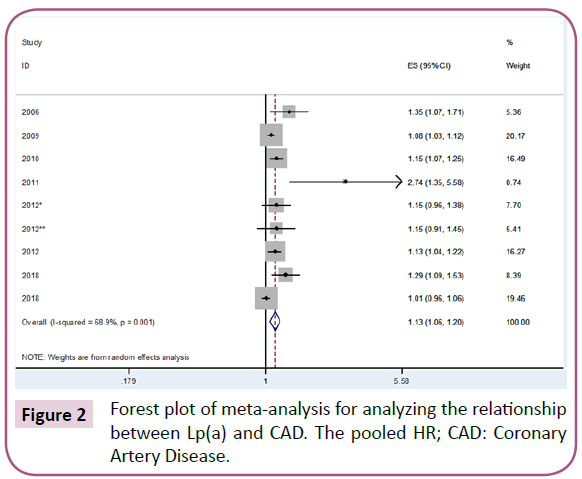
Figure 2: Forest plot of meta-analysis for analyzing the relationship between Lp(a) and CAD. The pooled HR; CAD: Coronary Artery Disease.
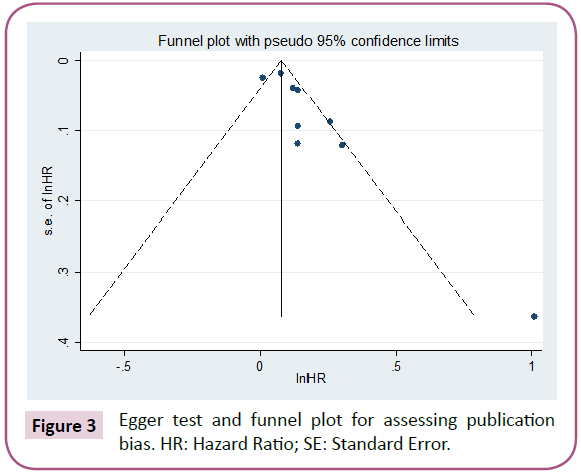
Figure 3: Egger test and funnel plot for assessing publication bias. HR: Hazard Ratio; SE: Standard Error.
Subgroup Analysis
Age
These prospective studies with mean age <55 years followed a similar trend. The pooled studies showed that Lp(a) was a risk factor for CAD both in the young and elderly participants. However, in the CAD patients with elevated Lp(a), younger patients had higher HR (the pooled HR 1.275; 95%CI 1.051-1.546; p=0.014), compared to the elderly (the pooled HR 1.120; 95% CI 1.022-1.227; P=0.015; Figure 4).
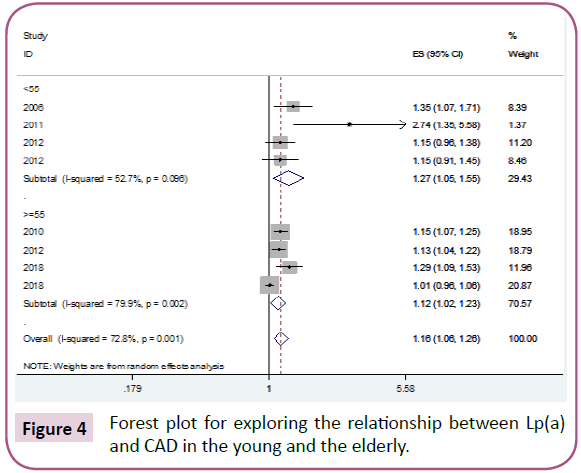
Figure 4: Forest plot for exploring the relationship between Lp(a) and CAD in the young and the elderly.
Detection measurement for Lp(a)
We screened the detection measurement for Lp(a) in the eligible literatures. In our meta-analysis, immunoturbidimetric assay were used in 4 studies, double-antibody enzyme-linked immunosorbent assay were used in 3 studies, and the remaining one did not provide the measurement. The different detection measurements didn’t modify the relationship between Lp(a) and CAD (immunoturbidimetric assay: the pooled HR: 1.191; 95%CI 1.039-1.365; double-antibody enzyme-linked immunosorbent assay technique: the pooled HR:1.150; 95%CI 1.074-1.231; (Figure 5).
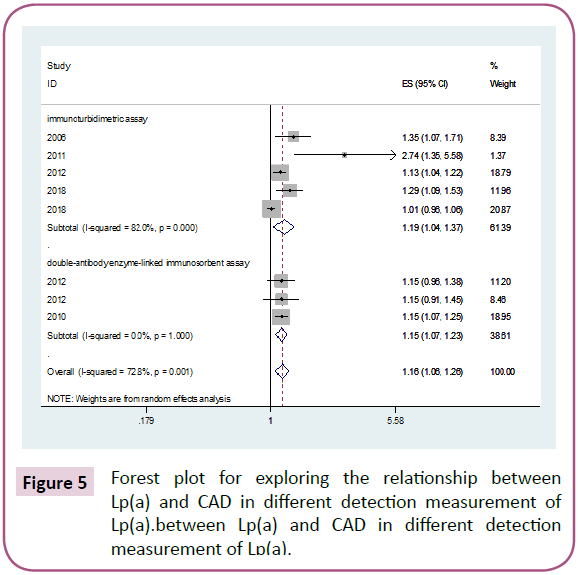
Figure 5: Forest plot for exploring the relationship between Lp(a) and CAD in different detection measurement of Lp(a).between Lp(a) and CAD in different detection measurement of Lp(a).
Discussion
Cardiovascular diseases (CVD) are the leading killer in chronic diseases. Early detection of risk factors and prevention could reduce future CVD events. In the past decade, researchers were not optimistic about the emerging maker due to the detection measurements and medications. In recent years, researchers have gained a new understanding of Lp(a). Although Lp(a) lacks of sufficient evidence for physiological effects, it has widely proved that Lp(a) was closely related to the atherosclerotic cardiovascular disease (ASCVD) and may be related to its ability to transport oxidized phospholipids (OxPL). Covalent binding of OxPL to Apo(A) mediated the development inflammation [21]. In addition, Lp(a) could directly enter and accumulate, causing inflammation and calcification in the intima of artery or aortic valve leaflets [6]. It also reported that Lp(a) was considered to be an independent and genetic risk factor, which causing cardiovascular events. Supporting evidence for the atherosclerosis of Lp(a) comes from Mendelian randomized studies [22], which showed that lifelong exposure to altered Lp(a) levels due to LPA gene variants could lead to changes in cardiovascular risk. It also proved that Apo(a) could promote atherosclerosis. The inflammatory process is now extensively studied in arteries.
In the large-scale prospective population study with 18,720 participants [17], it found that Lp(a) levels were associated with future risk of hospitalization and death in peripheral arterial disease (PAD). It confirmed the positive correlation between Lp(a) and CAD risk. Multiple studies in different populations and ethnic groups also confirmed the value of Lp(a) in the occurrence and prognosis of stroke [23-25]. These findings supported our conclusions and suggested that Lp(a) was a risk factor for vascular diseases. A previous meta-analysis has confirmed that elevated Lp(a) is an independent risk factor for ischemic stroke and may be particularly relevant for young stroke patients [26]. In the early family history of CVD, Lp(a) should be detected. The 2016 ESC/EAS guidelines recommended measurement of Lp(a) in selected cases at high risk or in patients with a family history of premature CVD [27]. However, a recent study showed that Lp(a) concentration was not associated with adverse cardiovascular outcomes in patients with recent ACS who are treated with statins. These findings called into question whether treatment specifically targeted to reduce Lp(a) levels would thereby lower the risk for ischemic cardiovascular events after ACS [19].
We conducted this meta-analysis with 8 prospective studies containing a total of 86,808 subjects with a follow-up period of 2 to 20 years, and 8180 subjects eventually developed CAD. The results showed that Lp(a) was significantly associated with CAD (the pooled HR: 1.132; 95% CI, 1.063-1.204; p=0.000), but the heterogeneity was high enough (Q=25.74; I2=68.9%; p=0.001). We found that the two studies mainly caused heterogeneity [19,20]. We removed the two studies and further analyzed. The results were shown in Figure 6. Lp(a) still independently predicted CAD prognosis, and the pooled HR was: 1.161 (95% CI: 1.106-1.219; p=0.000).
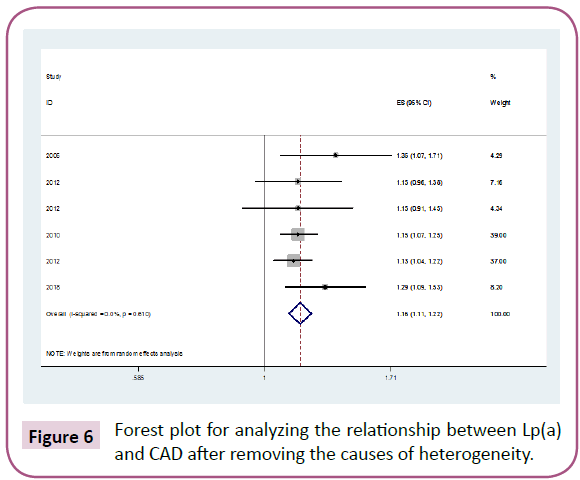
Figure 6: Forest plot for analyzing the relationship between Lp(a) and CAD after removing the causes of heterogeneity.
We performed a subgroup analysis to explore whether age and measurement methods could modify the relationship between Lp(a) and CAD. Subgroup analysis found that Lp(a) was more valuable in the young population than in the elderly, so we advocated early detection of Lp(a) in high risk population. The Lp (a) detection measurements had little effect on the relationship between Lp(a) and CAD. In recent years, it has been proposed that the amount-of-substance concentration of Lp(a) (nmol/L) is superior to the mass concentration (mg/L). Therefore, we still advocated the selection of more accurate measurement methods.
There are a number of limitations in this meta-analysis which should be discussed seriously. The 8 articles are from large-scale clinical trials. Newcastle-Ottawa scale were used to assess the qualities of literatures, and the results show that the score for each article≥6. However, we only research from two electronic databases, and the literatures are not comprehensive enough. There is also a high level of heterogeneity in the literature. We speculate that analytical data with high contrast and low contrast may be a source of heterogeneity, and we have not further analyzed it.
Conclusion
In conclusion, our meta-analysis emphasized the importance of high Lp(a) as an independent but modest risk factor in coronary artery diseases, and it became especially evident in younger populations.
Acknowledgement
This study was funded by the National Key R&D Program “Highly Trustworthy and Intelligent Brain and Cerebrovascular Disease Diagnosis and Treatment Service Mode Solution” (Project No. 2017YFC0113000) and “Community-based treatment and rehabilitation model of integrated Chinese and Western medicine for heart and vascular diseases” (Project No. SGYYZ201610).
Statement of Ethics
The authors have no ethical conflicts to disclose.
Disclosure Statement
The authors have no conflicts of interest to declare
Author Contributions
Yang Lan and Xiaoxiao Zhao respectively screen the literature from two electronic databases based on inclusion and exclusion criteria. When the two reviewers have disagreement, Yingyi Zhang, a third person, makes further judgments; Xiaofei Wang and Zhuangzhuang Zhang discuss statistical methods; Xincheng Song and Jia Chen revises the article.
References
- Ma L, Wu J, Niu D, Yu R, Song J, et al. (2014) Serum lipoprotein(a) complexes with beta2-glycoprotein I levels in patients with ischemic stroke. Clin Chim Acta 429: 163-167.
- Chakraborty B, Vishnoi G, Goswami B, Gowda SH, Chowdhury D, et al. (2013) Lipoprotein(a), ferritin, and albumin in acute phase reaction predicts severity and mortality of acute ischemic stroke in North Indian patients. J Stroke Cerebrovasc Dis 22: e159-e167.
- Virani SS, Brautbar A, Davis BC, Nambi V, Hoogeveen RC, et al. (2012) Associations between lipoprotein(a) levels and cardiovascular outcomes in black and white subjects: the atherosclerosis risk in communities (ARIC) study. Circulation 125: 241-249.
- Tsimikas SA (2017) Lipoprotein(a): Diagnosis, prognosis, controversies, and emerging therapies. Jou of the Amer Col of Cardiology 69: 692-711.
- Kronenberg F, Utermann G (2013) Lipoprotein(a): Resurrected by genetics. J Intern Med 273: 6-30.
- Teinberg D, Witztum JL (2010) Oxidized low-density lipoprotein and atherosclerosis. Arterioscler Thromb Vasc Biol 30: 2311-2316.
- Zhang W, Zhang XA (2014) Prognostic value of serum lipoprotein(a) levels in patients with acute ischemic stroke. Neuroreport 25: 2622-2666.
- Sultan SM, Schupf N, Dowling MM, Deveber GA, Kirton A, et al. (2014) Review of lipid and lipoprotein(a) abnormalities in childhood arterial ischemic stroke. Int J Stroke 9: 79-87.
- Virani SS, Brautbar A, Davis BC (2012) Associations between lipoprotein(a) levels and cardiovascular outcomes in black and white subjects: The Atherosclerosis Risk in Communities (ARIC) Study. Circulation 125: 241.
- Clarke R, Peden JF, Hopewell JC (2009) PROCARDIS Consortium. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med 361: 2518-2528.
- Stang A (2010) Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25: 603-605.
- Egger M, Smith GD, Phillips AN (1997) Meta-analysis: Principles and procedures. BMJ 315: 1533-1537.
- Riley RD, Higgins JPT, Deeks JJ (2011) Interpretation of random effects meta-analyses. BMJ 342: d549-d549.
- Suk DJ, Rifai N, Buring JE (2007) Lipoprotein(a), measured with an assay independent of apolipoprotein(a) isoform size, and risk of future cardiovascular events among initially healthy women. Dig of the World Core Med Jou 296: 1363-1370.
- Kamstrup PR, Tybjærghansen A, Steffensen R (2009) Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. Jama 301: 2331-2339.
- Canoui PF, Luc GBard JM, Ferrieres J (2010) Relative contribution of lipids and apolipoproteins to incident coronary heart disease and ischemic stroke: the PRIME Study. Cerebrovasc Dis 30: 252-259.
- Gurdasani D, Sjouke B, Tsimikas S (2012) Lipoprotein(a) and Risk of Coronary, Cerebrovascular, and Peripheral Artery Disease The EPIC-Norfolk Prospective Population Study[J]. Arterioscler Thromb Vasc Biol 32: 3058-3065.
- Dai W, Long J, Cheng Y (2018) Elevated plasma lipoprotein(a) levels were associated with increased risk of cardiovascular events in Chinese patients with stable coronary artery disease. Sci Rep 8: 7726.
- Schwartz GG, Ballantyne CM, Barter PJ (2018) Association of Lipoprotein(a) With Risk of Recurrent Ischemic Events Following Acute Coronary Syndrome: Analysis of the dal-Outcomes Randomized Clinical Trial. Jama Card 3: 164-168.
- Lamon-Fava S, Marcovina SM, Albers JJ (2011) Lipoprotein(a) levels, apo(a) isoform size, and coronary heart disease risk in the Framingham Offspring Study. Journal of Lip Res 52: 1181-1187.
- Tsimikas S, Mallat Z, Talmud PJ, Kastelein JJ, Wareham NJ, et al. (2010) Oxidation-specific biomarkers, lipoprotein(a), and risk of fatal and nonfatal coronary events. Jou of the Amer Col of Card 56: 946-995.
- Clarke R, Peden JF, Hopewell JC, Kyriakou T, Goel A, et al. (2009) Genetic variants associated with lp(a) lipoprotein level and coronary disease. The New England Jou of Med 361: 2518-2528.
- Li SY, Gao Y, Ma WN, Wang HC, Zhou G, et al. (2014) The relationship between serum lipoprotein (a) levels and ischemic stroke risk: A cohort study in the Chinese population. In?ammation 37: 686-693.
- Chakraborty B, Vishnoi G, Goswami B, Gowda SH, Chowdhury D, et al. (2013) Lipoprotein(a), ferritin, and albumin in acute phase reaction predicts severity and mortality of acute ischemic stroke in North Indian patients. J Stroke Cerebrovasc Dis 22: e159-e167.
- Nave AH, Lange KS, Leonards CO (2015) Lipoprotein (a) as a risk factor for ischemic stroke: A meta-analysis[J]. Atherosclerosis 242: 496-503.
- Catapano AL, Graham I, De Backer G (2016) ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J 37: 2999-3058.
- Konerman M, Kulkarni K, Toth PP (2012) Lipoprotein(a) particle concentration and lipoprotein(a) cholesterol assays yield discordant classification of patients into four physiologically discrete groups. Jou of Clin Lipidology 6: 368-373.

