Juliana Silveira Lima de Castro1, Jerusa Santos dos Reis2, Juan Pablo Ramon Serrano1, Samuel Galante Romanini1, Isabela Trindade Torres1, Facundo Galetti1, José Celso Ardengh1
1Endoscopy Unit, 9 de Julho Hospital, São Paulo, Brazil
2Department of Gastrointestinal Endoscopy, Hospital Universitario PresidenteDutra , Sao Luiz, Maranhão, Brazil
- Corresponding Author:
- Juliana Silveira Lima de Castro
Endoscopy Unit, Hospital Nove de Julho
Rua Peixoto Gomide, 545
Cerqueira César - CEP: 01409-001 - São Paulo, SP – Brazil
Tel: +55-11-3147-9999
E-mail: julianasilveira_@hotmail.com
Received Date: May 02nd, 2021; Accepted Date: May 20th, 2021
Autoimmune pancreatitis (AIP) is a recurrent, infiltrative, inflammatory disease, which is not limited to pancreatic involvement and has a multiform clinical presentation.Morphological changes lead to irreversible destruction of the exocrine and endocrine glands with consequent pancreatic insufficiency. Interest in AIP has increased due to the recognition of radiological features such as irregular narrowing of the main pancreatic duct (MPD), pancreatic parenchyma alterations, IgG4 elevation, and lymphoplasmacytic infiltrate with abundant plasma cells. The diagnosis is made in patients with painless obstructive jaundice secondary to an inflammatory mass involving the biliary tract, accompanied by abdominal pain, weight loss, and increased levels of carbohydrate antigen 19-9 (CA19-9), mimicking pancreatic carcinoma. Tissue procurement is considered the “gold standard” for the diagnosis of AIP5. We report a case of IgG4 syndrome with a significant increase in CA19-9 level, acute pancreatitis, and enlargement of the pancreatic gland mimicking pancreatic carcinoma. An accurate diagnosis was obtained by EUS-FNA, and steroid treatment avoided unnecessary surgery.
Keywords
Autoimmune pancreatitis; Endoscopic ultrasound; Fine
needle biopsy; Immunoglobulin G4-Related Diseases; Follow-Up
INTRODUCTION
Autoimmune pancreatitis (AIP) is a recurrent,
infiltrative, inflammatory disease, which is not limited
to pancreatic involvement and has a multiform clinical
presentation [1]. Morphological changes lead to irreversible
destruction of the exocrine and endocrine glands with
consequent pancreatic insufficiency [2]. Interest in AIP has
increased due to the recognition of radiological features
such as irregular narrowing of the main pancreatic duct
(MPD), pancreatic parenchyma alterations, IgG4 elevation,
and lymphoplasmacytic infiltrate with abundant plasma
cells [3]. The diagnosis is made in patients with painless
obstructive jaundice secondary to an inflammatory mass
involving the biliary tract, accompanied by abdominal pain,
weight loss, and increased levels of carbohydrate antigen
19-9 (CA19-9), mimicking pancreatic carcinoma [4]. Tissue
procurement is considered the “gold standard” for the
diagnosis of AIP [5]. We report a case of IgG4 syndrome with
a significant increase in CA19-9 level, acute pancreatitis, and
enlargement of the pancreatic gland mimicking pancreatic
carcinoma. An accurate diagnosis was obtained by EUS-FNA,
and steroid treatment avoided unnecessary surgery
CASE REPORT
A 65-year-old man presented with recurrent upper
abdominal pain and back irradiation for 30 days. The
symptoms improved with oral analgesia and fasting.
He reported unmeasured weight loss and asthenia
and denied alcoholism. There was a history of type 2
diabetes mellitus 1 year previously, hypothyroidism,
and dyslipidemia. Additional findings were CA19-
9 250 mg/dL; carcinoembryonic antigen (CEA),
normal; antinuclear factor negative; and IgG4 3430
IU/L. Computed tomography (CT) showed diffuse and
uncharacteristic enlargement of the pancreatic head.
Magnetic resonance cholangiopancreatography (MRCP)
detected a heterogeneous, enlarged, "sausage" pancreas
(Figures 1). The main pancreatic duct (MPD) was
irregular, with dilated and stenosed areas. Endoscopic
ultrasound showed a diffusely enlarged, heterogeneous
pancreas, with hypoechogenic images on the head and
tail. The MPD was irregular, and we detected the presence
of inflammatory peripancreatic lymph nodes (Figures
2). Microhistological examination showed chronic AIP
with marked acinar atrophy, plasmacytic epithelial
permeation, eosinophilic exudate, and IgG4 positivity
(Figures 3). Based on the diagnosis, corticosteroid therapy
was initiated with prednisone 40 mg/day, systematically
reduced by 5 mg every 2 weeks, resulting in significant
clinical improvement, weight gain, disposition, and drop in
laboratory test levels during the first 2 months. However,
with the reduction of the medication dose, the patient
developed new abdominal pain and altered laboratory test results. As the diabetes mellitus was difficult to control
and was significantly altered in the bone densitometry
examination, azathioprine 5 mg/kg was started in an
attempt to maintain low doses of corticosteroids. The
patient started with complaints of dry mouth, discomfort,
and palpable lymph nodes in the cervical region and changes in urination. Specific examinations, such as submandibular
gland scintigraphy, cervical ultrasound, and urological
examination, detected submandibular gland insufficiency,
autoimmune cervical lymphadenopathy, and prostatitis.
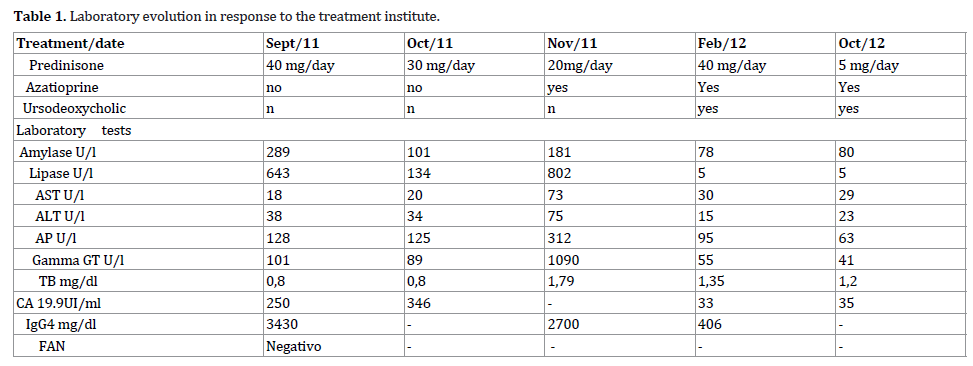
In control laboratory tests, pancreatic enzyme levels were
normal, but transaminases, cholestatic enzymes, and tumor markers increased (Table 1). Repeated MRCP revealed
symmetrical dilatation of the intrahepatic biliary tract with
reduction in caliber near the confluence of the main ducts.
With the improvement, it was decided to adjust the doses
of corticosteroids and azathioprine. After 3 months, the
patient had a complete clinical and laboratory remission.
With the complete action of the immunosuppressant, a
slow and gradual reduction of corticosteroid dosage was
achieved, resulting in 3 years of follow-up without relapse
(Table 1). In the current follow-up, 8 years after diagnosis
there is an evident sign of mild pancreatic insufficiency.
MRCP shows MPD dilatation and tortuosity, associated
with parenchymal atrophy, with a diagnosis of chronic
calcifying pancreatitis.
Figure 1: Abdominal MRI. Pancreas repaired in its body (A) and tail portion (B) with “sausage” aspect.
Figure 2: EUS imaging. (A) Endoscopic ultrasound image of hypoechoic area, inaccurate and heterogeneous boundaries. It looks like pancreatic cancer. (B) 22G needle aspiration puncture.
Figure 3: (A) Storiform fibrosis around the small pancreatic duct (hematoxylin and eosin, 20x). (B) Severe acinar atrophy, plasmacytic epithelial permeation, eosinophilic exudate, IgG4 positive (hematoxylin and eosin, 20x).
DISCUSSION
In North America, about 2.5% of patients undergoing
Whipple surgery for probable pancreatic carcinoma are
later diagnosed with AIP, and 20% of cases of Whipple
procedures for benign conditions can now be considered
as AIP [6]. Before the diagnosis of AIP, our patient was
indicated for surgical treatment due to a pancreatic head
mass, weight loss, and elevated CA19-9. AIP is one of a
group of diseases that are associated with high levels
of IgG4 and are capable of being the etiology of acute or
chronic pancreatitis of unknown cause. EUS-FNA was
critical for the diagnosis and initiation of treatment in our
patient. Examination showed either a diffusely enlarged,
hypoechogenic pancreas or a solitary mass in the pancreas
[7]. In these patients, fine-needle aspiration reveals IgG4-
positive lymphoplasmacytic infiltrates, as occurred in our
patient [8]. Because it is a relatively recently recognized
condition, the diagnosis of AIP is often not made, which
may result in delayed clinical treatment or unnecessary
surgical procedures. We should investigate for the
presence of AIP (IgG4 syndrome) in patients, mainly men
over 50 years old, who have acute or chronic pancreatitis
of unknown cause and a mass in the head of the pancreas. EUS-FNA avoided unnecessary Whipple surgery and
determined the best treatment for the pancreatic mass
identified by imaging methods.
Conflicts of Interest
All named authors hereby declare that they have no
conflicts of interest to disclose.
References
- Hart PA, Zen Y, Chari ST. Recent advances in autoimmune pancreatitis. Gastroenterol 2015; 149:39-51. [PMID: 25770706].
- Otsuki M. Autoimmune pancreatitis: A message from Japan. J
gastroenterol 2007; 18:1-5. [PMID: 17520215].
- Brito-Zeron P, Bosch X, Ramos-Casals M, Stone JH. IgG4- related disease: Advances in the diagnosis and treatment. Best
Pract Res Clin Rheumatol 2016; 30:261-78. [PMID: 27886799].
- Van Heerde MJ, Buijs J, Hansen BE, Waart M, Eijck CHJ, Kazemier G, et al. Serum level of Ca 19-9 increases ability of IgG4 test to distinguish patients with autoimmune pancreatitis from those with pancreatic carcinoma. Dig Dis Sci 2014; 59:1322-
9. [PMID: 24385012].
- Deshpande V, Zen Y, Chan JK. Consensus statement on the pathology of IgG4-related disease. Modern pathology 2012;
25:1181-92.
- Hardacre JM, Iacobuzio-Donahue CA, Sohn TA, Abraham SC, Yeo CJ, Lillemoe KD, et al. Results of pancreaticoduodenectomy for lymphoplasmacytic sclerosing pancreatitis. Ann Surg 2003;
237:853-8. [PMID: 12796582].
- Kanno A, Masamune A, Fujishima F, Iwashita T, Kodama Y, Katanuma A, et al. Diagnosis of autoimmune pancreatitis by EUSguided FNA using a 22-gauge needle: A prospective multicenter study. Gastrointestinal endoscopy 2016; 84:797-804. [PMID:
27068878].
- Farrell JJ, Garber J, Sahani D, Brugge WR. EUS findings in patients with autoimmune pancreatitis. Gastrointest Endos
2004; 60:927-36. [PMID: 15605008].




