Keywords
Bone and Bones; Diphosphonates; Jaw; Mandibular Diseases; Maxilla; Osteonecrosis; pamidronate; Surgery, Oral; zoledronic acid
Abbreviations
BRONJ: bisphosphonate-related osteonecrosis of the jaw
Dear Sir:
Erkan M, et al. commented on our publication of the first case of a patient with advanced pancreatic cancer and bone metastases who developed bisphosphonaterelated osteonecrosis of the jaw (BRONJ) [1, 2]. Erkan M, et al. also present a potential role of hyperbaric oxygen therapy in these patients [1].
According to a package insert in a special mailing by Merck Pharmaceuticals (Merck & Co., Inc., Whitehouse Station, NJ, USA), the estimated incidence of BRONJ is 0.7 per 100,000 persons per year [3, 4]. Several recent studies of patients with multiple myeloma and patients with breast cancer who received intravenous aminobisphosphonate therapy for metastatic bone lesions demonstrated 6-11% of the patients developed BRONJ. The incidence of BRONJ has been strongly correlated with the aminobisphosphonate pamidronate (Aredia®, Novartis, East Hanover, NJ, USA) and zoledronic acid (Zometa®, Novartis, East Hanover, NJ, USA) and is even higher in patients who have had recent dental extractions [5, 6].
Bisphosphonates are believed to bind to osteoclasts and interfere with bone remodeling. They interfere with the cholesterol biosynthesis pathway by inhibition of farnesyl diphosphate synthase. In time, the cytoskeleton of the osteoclast becomes dysfunctional and the ruffled border needed for bone resorption is unable to form. Aminobisphosphonates have also been shown to have antiangiogenic properties. The overall effect is a decrease in bone turnover and inhibition of the bone’s reparative ability [7, 8]. Injury to the bone in these patients via tooth extraction, dental surgery, or mechanical trauma is thought to initiate BRONJ.
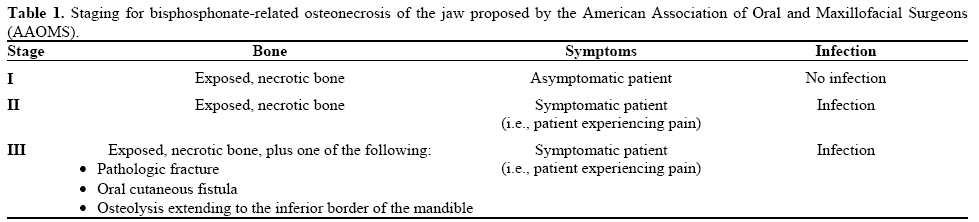
The American Association of Oral and Maxillofacial Surgeons (AAOMS) has proposed a staging system (Table 1) [1]. In addition to discontinuation of bisphosphonate therapy, medical management of BRONJ consists of antimicrobial rinses, systemic antibiotics, and systemic or topical antifungals. It is important to avoid dental therapy or perform minimally invasive dental therapy (i.e., root canal therapy instead of extraction). Surgical intervention for BRONJ remains limited because of the impaired ability of the bone to heal.
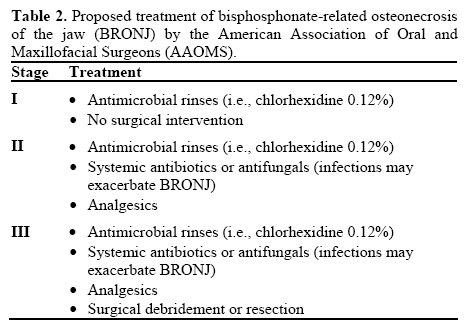
The treatment of BRONJ based on the consensus of a panel discussion from AAOMS, is described in Table 2. The role of adjunctive procedures (i.e., hyperbaric oxygen) and vascularized tissue transfers in the reconstructive management of BRONJ have yet to be elucidated. Hyperbaric oxygen therapy is a way of treatment which increases the oxygen content of the blood and, consequently, the amount of oxygen delivered to tissues. Hyperbaric oxygen therapy has been used in the treatment and prevention of osteoradionecrosis of the jaw for more than 30 years [9]. There is some data suggesting the role of hyperbaric oxygen therapy in the management of BRONJ [9, 10, 11, 12]. There are two ongoing randomized controlled trials which are testing the effectiveness of adjunctive hyperbaric oxygen therapy in the management of BRONJ [13] and final results are pending.
One controversy lies about the fear that hyperbaric oxygen may have a cancer-promoting effect or may lead to metastatic growth. Feldmeierr et al. reviewed all available literature and showed that there is no evidence to support this concern [14].
We agree with Erkan M, et al. [1] that a multidisciplinary approach is fundamental for achieving a favorable outcome in patients with BRONJ. The wide use of oral BRONJ have yet to be completely determined. Long-term studies identifying the patients who are at risk for this disease process are still pending.
Conflict of interest The author has no potential conflicts of interest
References
- Erkan M, et al. Bisphosphonate Related Osteonecrosis of the Jaw in Cancer Patients and Hyperbaric Oxygen Therapy. JOP. J Pancreas (Online) 2009; 10(2):212-214.
- Smith A, Kressley A, Saif MW. Oral osteonecrosis associated with the use of zoledronic acid: first case of a patient with advanced pancreatic cancer and bone metastases. JOP. J Pancreas 2009; 10(2):212-4.
- American Dental Association. Report of the Council of Scientific Affairs. Expert panel recommendations: Dental management of patients on oral bisphosphonate therapy. American Dental Association. June 2006.
- AAOMS. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg. Mar 2007;65(3):369-76.
- Bamias A, Kastritis E, Bamia C, et al. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol. Dec 1 2005;23(34):8580-7.
- Mavrokokki T, Cheng A, Stein B, et al. Nature and frequency of bisphosphonate-associated osteonecrosis of the jaws in Australia. J Oral Maxillofac Surg. Mar 2007;65(3):415-23.
- Khan AA, Sandor GK, Dore E, Morrison AD, Alsahli M, Amin F, et al. Bisphosphonate associated osteonecrosis of the jaw. J Rheumatol. Mar 2009;36(3):478-90.
- Fisher JE, Rogers MJ, Halasy JM, et al. Alendronate mechanism of action: geranylgeraniol, an intermediate in the mevalonate pathway, prevents inhibition of osteoclast formation, bone resorption, and kinase activation in vitro. Proc Natl Acad Sci U S A. Jan 5 1999;96(1):133-8.
- Feldmeier JJ, Hampson NB. A systematic review of the literature reporting the application of hyperbaric oxygen prevention and treatment of delayed radiation injuries: an evidence based approach. Undersea Hyperb Med. 2002; 29(1):4-30.
- Freiberger J, Padila-Burgos R, Chhoeu AH, Kraft KH, Boneta O, Moon RE, Piantodosi CA. Hyperbaric oxygen treatment and bisphosphonate-induced osteonecrosis of the jaw: A case series. J Oral Maxillofac Surg 2007; 65(7):1321-7.
- Shimura K, Shimazaki C, Taniguchi K, Akamatsu S, Okamoto M, Uchida R, et al. Hyperbaric oxygen in addition to antibiotic therapy is effective for bisphosphonate-induced osteonecrosis of the jaw in a patient with multiple myeloma. Int J Hematol 2006; 84(4):343-5.
- Freiberger JJ. Utility of hyperbaric oxygen in treatment of bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg. 2009; 67(5 Suppl):96-106.
- Feldmeier JJ, Heimbach RD, Davolt DA, Brakora MJ. Hyperbaric oxygen and the cancer patient: a survey of practice patterns. Undersea Hyperb Med. 1993; 20(4):337-45.
- Feldmeier J, Carl U, Hartmann K, Sminia P. Hyperbaric oxygen: does it promote growth or recurrence of malignancy? Undersea Hyperb Med. 2003; 30(1):1-18.

