Keywords
Pancreaticoduodenectomy; Radiology, Interventional
Abbreviations
PD: pancreaticoduodenectomy; PPPD: pylorus preserving proximal pancreaticoduodenectomy
INTRODUCTION
Over the past two decades, mortality and morbidity after pancreaticoduodenectomy (PD) have improved significantly from a shift of care to higher volume centers which has allowed for improved surgical experience and technique, better surgical intensive care and critical care, better antibiotic and infectious disease services, better and faster crosssectional imaging with interventional radiology establishing a crucial role in the management of the complications following PD [1, 2, 3, 4].
Delayed arterial hemorrhage is an uncommon complication (incidence 2-4%) but carries a high mortality, with up to a third of patients dying as a consequence [5]. Because delayed arterial hemorrhage post PD is rare, its management remains unclear. Interventional radiology has become more sophisticated over the past two decades, consequently delayed arterial hemorrhage is increasingly managed by this approach, rather than surgery. The present paper discusses our experience in the management of delayed arterial hemorrhage post PD and the role of angiograms, endoscopy and laparotomy in its management.
METHODS
Between 1993 and 2007, 317 head of pancreas resections were performed at our institution. For this analysis, delayed arterial hemorrhage was defined as bleeding greater than 48 hours after PD, presenting either as revealed blood loss: via the abdominal drain or the gastrointestinal tract as hematemesis or melena, or as concealed blood loss: in the form of cardiovascular collapse or a post operative drop in hemoglobin necessitating blood transfusion. On retrospective analysis, five cases of delayed arterial hemorrhage post PD (frequency 1.6%) were identified.
ETHICS
The principles of the Declaration of Helsinki were adhered to throughout this review.
CASE REPORTS
Case 1
A 70-year-old male underwent a pylorus preserving proximal pancreaticoduodenectomy (PPPD) for a distal common bile duct cholangiocarcinoma. On the 14th postoperative day, the patient collapsed after an episode of melena, followed by two bouts of hematemesis. In view of the patient being hemodynamically unstable, the decision was made to proceed straight to laparotomy. Operative findings were disruption of the pancreaticojejunal anastomosis, with fresh blood in the proximal jejunum. No active bleeding point was able to be identified. Technically, it was not possible to reconstruct a new pancreaticojejunostomy because the pancreatic stump was grossly oedematous and pancreatic duct non-dilated. Completion pancreatectomy, with spleen preservation and over sewing of the jejunum was performed. The patient continued to bleed on the intensive care unit and 24 hours later, the patient returned to the operating room, where a distal gastrectomy, proximal jejunal resection and refashioning of bilioenteric and gastrojejunal anastomoses was done. The patient became septic and then died of multiorgan failure twenty days post-operatively.
Case 2
A 56-year-old man underwent a PPPD and right nephrectomy for biliary papillomatosis and renal cell carcinoma. On post-operative day 21, he had an episode of hematemesis but remained hemodynamically stable. Upper endoscopy demonstrated an ulcer at the duodenojejunal anastomosis which was not actively bleeding, so no therapeutic procedure was performed. However, a subsequent visceral angiogram did demonstrate active bleeding from the distal branches of the third jejunal artery, at the site of the duodenojejunal anastomosis. The vessel was selectively catheterized with a coaxial 3 French catheter (FasTracker-18MX, Boston Scientific, Natick, MA, USA) and embolization performed with a small amount of polyvinyl alcohol (Contour, Boston Scientific, Natick, MA, USA), initially with a particle size of 150-250 μm and then 355-500 μm (Figure 1ab). Complete hemostasis was achieved and the patient was discharged one week later.
Figure 1. a. More selective study demonstrating
extravasation is from the 3rd jejunal branch (arrow). b. Following particle embolization active hemorrhage has
ceased.
Case 3
A 57-year-old male underwent a PPPD for pancreatic adenocarcinoma, arising from an intraductal papillary mucinous tumour. He was discharged on post-operative day 19. Nineteen days after discharge the patient collapsed with hematemesis and was admitted to his local hospital. Upper endoscopy and CT were both unremarkable. He received a blood transfusion and was about to be discharged after an inpatient stay of seven days, when he had a further episode of hematemesis. Repeat upper endoscopy demonstrated a large clot at the duodenojejunal anastomosis, no therapeutic procedure was undertaken and the patient was transferred back to our institution. On arrival a visceral angiogram was performed which demonstrated a pseudoaneurysm of the splenic artery. The splenic artery was catheterized, with a 7 French sidewinder catheter (Cordis Corporation, Miami, FL, USA), to a point beyond the pseudoaneurysm and MR compatible platinum coils (William Cook Europe, Bjaeverskov, Denmark) were placed on either side of the pseudoaneurysm neck (Figure 2ab). The patient remained well and was discharged seven days later.
Figure 2. a. Coeliac axis angiogram demonstrating
pseudoaneurysm of proximal splenic artery (arrow). b. Post embolization of proximal artery with multiple
coils (arrow). Distal splenic artery filled via the short
gastric arteries.
Case 4
A 63-year-old female had a PPPD for pancreatic adenocarcinoma. On the 12th day after surgery she collapsed with a massive hematemesis. Upper endoscopy in the operating room found a stomach full of blood but the bleeding point was unable to be identified, a subsequent laparotomy also failed to localise a bleeding point. A day later on the intensive care unit, the patient had further bleeding, manifested by fresh blood in the nasogastric tube and per rectum. Visceral angiogram was performed but again no active bleeding point could be localised. The patient had no further episodes of bleeding but became progressively septic and died of multi-organ failure 25 days after PPPD.
Case 5
A 55-year-old male had a Whipple procedure for pancreatic adenocarcinoma. On the 4th post-operative day, the abdominal drain was found to contain 400 mL of blood. He was hemodynamically stable but a drop in hemoglobin necessitated a four unit blood transfusion. Visceral angiogram was performed and a 2.5 cm diameter pseudoaneurysm arising from the transverse branch of the dorsal pancreatic artery was found. The transverse pancreatic artery and an epiploic branch vessel, beyond the pseudoaneurysm were selectively catheterized with a coaxial 3 French (FasTracker-18MX, Boston Scientific, Natick, MA, USA) and embolized with platinum microcoils (Boston Scientific, Natick, MA, USA). Further platinum microcoils were then deployed proximal to the arterial defect (Figure 3ab). After embolization, the patient had a swinging temperature with raised inflammatory markers. CT was performed which demonstrated a small collection in the gastrosplenic ligament which was managed with antibiotics. The patient otherwise had an uneventful course and was discharged on the 18th post-operative day.
Figure 3. a. Angiogram performed with catheter tip in
origin of dorsal pancreatic artery (black arrow)
demonstrating pseudoaneurysm of transverse
pancreatic artery (white arrows). b. Coeliac axis
angiogram post embolization demonstrating
pseudoaneurysm to be excluded from the circulation by
multiple platinum coils (white arrows).
DISCUSSION
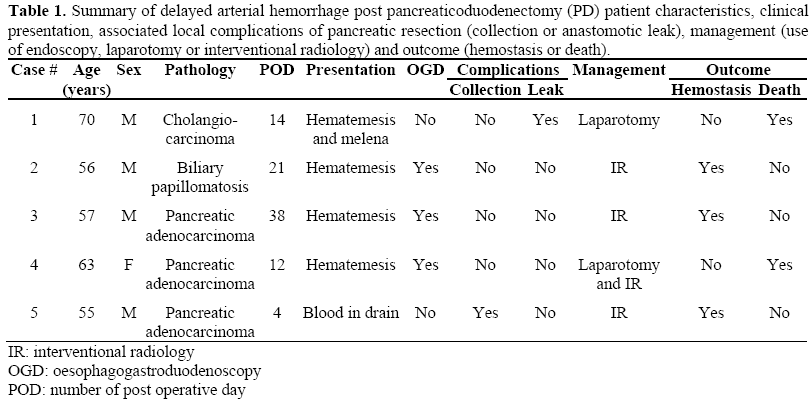
On retrospective review, of 317 head of pancreas resections between 1993 and 2007, five cases of delayed arterial hemorrhage were identified. Details of patient characteristics, clinical presentation, management and outcome are summarised in Table 1. Delayed arterial hemorrhage post PD occurs in 2-4% of cases and our experience is comparable with a frequency of 1.6%. Based on the timing of bleed, hemorrhagic complications after PD maybe divided into early or delayed. Early hemorrhage occurs within the first 48 hours after surgery and is generally caused by technical failure which normally requires immediate laparotomy for resolution [6], whereas delayed arterial hemorrhage is any bleeding after this time period. The timing of delayed arterial hemorrhage presentation is variable. In our series, delayed arterial hemorrhage on average occurred on the 18th post operative day (range: 4-38 days), with one case presenting after discharge (Case 3), highlighting the need for awareness of the clinical presentations of delayed arterial hemorrhage in the post operative PD patient, in order to facilitate prompt and appropriate transfer, to a specialist unit where all facilities, interventional radiology and surgical, are available as required.
Multiple factors have been suggested to contribute or predispose to the development of delayed arterial hemorrhage post PD, such as in the regional lymphadenectomy and skeletonization of the vasculature leaving the vessels vulnerable to damage from local sepsis arising from pancreatic fistula, anastomotic leakage or abscess formation [7]. In the published delayed arterial hemorrhage post PD case series, approximately two thirds of reported delayed arterial hemorrhage cases are found to have an underlying collection or anastomotic leak, with pseudoaneurysm formation identified in approximately a third of cases. In this series, local complications potentially contributed to the development of delayed arterial hemorrhage in 4 patients: one (Case 1) from a disruption of the pancreaticojejunal anastomosis; another one (Case 2) from a disruption of duodenojejunal anastomosis secondary to ulceration through tissue ischemia; the third (Case 5) from intraabdominal sepsis and the fourth (Case 3) remained unclear but most likely related to an extensive surgical dissection weakening the advential wall of the artery. Emphasising that when present, contributing local complications of pancreatic resection should be identified and managed appropriately, in addition to targeted delayed arterial hemorrhage therapy.
Delayed arterial hemorrhage post PD has been reported to occur into the gastrointestinal tract or more commonly, the abdominal cavity [8]. Though in our clinical experience, the most common presentation of delayed arterial hemorrhage was as an upper gastrointestinal bleed (Table 1). Endoscopy, which is the standard first line of investigation for upper gastrointestinal bleeding, may fail to be therapeutic in the post PD scenario through difficulties in localizing the site of hemorrhage. Our experience illustrates this point and other reports in the literature have given accounts of “positive” endoscopic findings being misleading and as a consequence delay definitive intervention or lead to death in the worst case [9, 10, 11]. Therefore, endoscopy has no role in the initial management of delayed arterial hemorrhage post PD.
Historically, laparotomy has been the first choice of treatment for delayed arterial hemorrhage post PD [9, 12]. Laparotomy allows hemostasis by ligation or under running of vessels/pseudoaneurysms to be combined with treatment of contributing factors to delayed arterial hemorrhage such as anastomotic disruption or intra-abdominal collections. From the published cases, laparotomy and interventional radiology appear to be equally effective in arresting hemorrhage. Though in our institute’s experience, the two cases where laparotomy was performed (Cases 1 and 4), the site of bleeding was not localised, with one patient continuing to bleed post operatively and the other rebleeding in the subsequent 24 hours. Whereas, in all the cases where interventional radiology was used as the first line management of delayed arterial hemorrhage post PD, definitive hemostasis was achieved in all cases.
A higher morbidity and mortality is reported in the literature for patients managed by laparotomy compared to interventional radiology. In our experience, admission to intensive care was required for the two patients (Cases 1 and 4) initially managed by laparotomy and both of them eventually died (Table 1). In contrast, when delayed arterial hemorrhage post PD was treated initially by interventional radiology, no intensive care admission was required and the patients were discharged, on average 9 days later. The higher morbidity and mortality of laparotomy is not unexpected on two counts. Firstly, patients selected for immediate laparotomy often have a greater degree of hemodynamic compromise, compared with patients where interventional radiology has been used as first line management. Secondly, an operative approach is an invasive strategy, in patients potentially debilitated by complications relating to the original PD, such as sepsis or anastomotic breakdown which may have predisposed to the development of delayed arterial hemorrhage initially.
Selective visceral angiography of the celiac and superior mesenteric arteries is probably the most valuable initial examination to identify the site of bleed post PD when clinical parameters allow for a more measured evaluation [13]. However, angiography also has its limitations like surgery and endoscopy, when the bleed is venous, diffuse or intermittent [14], which may then lead to interventional radiology diagnostic failure which happened in one patient (Case 4). Trans-catheter arterial embolization is emerging, as a safe and effective option for the first line treatment of delayed arterial hemorrhage post PD. In addition, our institute’s experience of interventional radiology also found it to be efficacious, with minimal morbidity and no mortality, though recognised drawbacks of interventional radiology can be the accidental or intentional occlusion of the hepatic artery, which can lead to cholangitis, hepatic abscess or fatal liver failure. The recent utilization of covered stents may prove to be a solution to this issue, establishing further the role of interventional radiology in the management of delayed arterial hemorrhage post PD [15, 16].
Deciding on the optimal management of this life threatening complication is difficult. Currently, there is no high quality evidence defining the standard management of delayed arterial hemorrhage post PD. As interventional radiology becomes more sophisticated, it will increasingly be used as the first line of diagnosis and therapy in this complex group of patients. Though ultimately, the final decision of which delayed arterial hemorrhage management pathway is selected will be dictated by the clinical status of the patient and institution preference. A meta-analysis or a multi-institutional analysis would provide more data to provide more information on this difficult problem, as a prospective study is impractical and no single institution will acquire enough patients to reach any conclusion.
Conflict of interest
The authors have no potential conflicts of interest
References
- Yeo CJ, Cameron JL, Sohn TA, Lillemoe KD, Pitt HA, Talamini MA, et al. Six hundred fifty consecutive pancreaticoduodenectomies in the 1990s: pathology, complications, and outcomes. Ann Surg 1997; 226:248-57. [PMID 9339931]
- Schafer M, Mullhaupt B, Clavien P. Evidencebased pancreatic head resection for pancreatic cancer and chronic pancreatitis. Ann Surg 2002; 236:137-48. [PMID 12170018]
- DeOliveira ML, Winter JM, Schafer M, Cunningham SC, Cameron JL, Yeo CJ, Clavien PA. Assessment of complications after pancreatic surgery: A novel grading system applied to 633 patients undergoing pancreaticoduodenectomy. Ann Surg 2006; 244:931-7. [PMID 17122618]
- Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon volume and operative mortality in the United States. N Engl J Med 2003; 349:2117-27. [PMID 14645640]
- de Castro SM, Kuhlmann KF, Busch OR, van Delden OM, Laméris JS, van Gulik TM, et al. Delayed massive hemorrhage after pancreatic and biliary surgery: embolization or surgery? Ann Surg 2005; 241:85-91. [PMID 15621995]
- Jordan GL Jr. Pancreatic resection for pancreatic cancer. Surg Clin North Am 1989; 69:569-97. [PMID 2658164]
- Reber PU, Baer HU, Patel AG, Triller J, Büchler MW. Life-threatening upper gastrointestinal tract bleeding caused by ruptured extrahepatic pseudoaneurysm after pancreatoduodenectomy. Surgery 1998; 124:114-5. [PMID 9663263]
- Aranha GV, O'Neil S, Borge MA. Successful nonoperative management of bleeding hepatic artery pseudoaneurysm following pancreaticoduodenectomy. Dig Surg 1999; 16:528-30. [PMID 10805557]
- Brodsky JT, Turnbull AD. Arterial hemorrhage after pancreatoduodenectomy. The 'sentinel bleed'. Arch Surg 1991; 126:1037-40. [PMID 1863209]
- Sato N, Yamaguchi K, Shimizu S, Morisaki T, Yokohata K, Chijiiwa K, Tanaka M. Coil embolization of bleeding visceral pseudoaneurysms following pancreatectomy: the importance of early angiography. Arch Surg 1998; 133:1099-102. [PMID 9790208]
- Okuno A, Miyazaki M, Ito H, Ambiru S, Yoshidome H, Shimizu H, et al. Nonsurgical management of ruptured pseudoaneurysm in patients with hepatobiliary pancreatic diseases. Am J Gastroenterol 2001; 96:1067-71. [PMID 11316148]
- van Berge Henegouwen MI, Allema JH, van Gulik TM, Verbeek PC, Obertop H, Gouma DJ. Delayed massive haemorrhage after pancreatic and biliary surgery. Br J Surg 1995; 82:1527-31. [PMID 8535810]
- Mandel SR, Jaques PF, Sanofsky S, Mauro MA. Nonoperative management of peripancreatic arterial aneurysms. A 10-year experience. Ann Surg 1987; 205:126-8. [PMID 3492972]
- Cahow CE, Gusberg RJ, Gottlieb LJ. Gastrointestinal hemorrhage from pseudoaneurysms in pancreatic pseudocysts. Am J Surg 1983; 145:534-41. [PMID 6601464]
- Mansueto G, D'Onofrio M, Iacono C, Rozzanigo U, Serio G, Procacci C. Gastroduodenal artery stump haemorrhage following pylorus-sparing Whipple procedure: treatment with covered stents. Dig Surg 2002; 19:237-40. [PMID 12119528]
- Zealley IA, Tait IS, Polignano FM. Delayed massive hemorrhage after pancreatic and biliary surgery: embolization or surgery? Ann Surg 2006; 243:138-9. [PMID 16371750]




