Keywords
Delirium; Elderly; Prevention; Management
Introduction
The Diagnostic and Statistical Manual of Mental Disorders 5 (DSM- 5) identifies delirium as a condition associated with a disturbance in attention, awareness and cognition [1]. If a diagnosis of delirium is indicated, these symptoms should not occur due to an underlying neurocognitive disorder or in conjunction with a severely reduced level of arousal as in a state of coma. Additionally, the changes in attention, awareness and cognition should develop over a short period of time (usually hours to days) and represent a change from baseline and fluctuate in severity during the course of the day. Evidence from history, physical examination or laboratory findings should indicate that these symptoms are caused by the direct physiological consequences of another medical condition, substance intoxication or withdrawal.
Although the rates of delirium are low in the elderly individuals living in the community at 1% to 2%, their prevalence increases significantly in the hospital setting [2,3]. During admission to hospitals, the incidence rates for delirium increase to between 11% and 42%. The incidence of delirium during a hospital stay rises to over 50% [3,4]. In the intensive care units (ICU), the incidence of delirium in the elderly is greater than 70% [2,3] Postoperative delirium is very common in the elderly with an incidence rate that varies between 15% and 60% [2,3]. It is currently estimated that in the United States between one-tenth and one-half of all individuals ≥ 65 years in age who require hospitalization are affected by delirium [5].
Delirium develops in the elderly due to the interaction between the different predisposing and precipitating factors [2,3] Increasing age and pre-existing cognitive deficits appear to be common predisposing factors for delirium in the elderly. Additional predisposing factors include the impairment of vision, presence of severe illness and renal disease [6]. Frequently identified precipitating factors for delirium include the use of physical restraints, malnutrition, greater than three medications added to the treatment regimen at a time, the use of urinary catheters and any type of iatrogenic event including medication adverse effects, hospital acquired infection, dehydration and falls [3,6,7] Common drug classes that may precipitate delirium in older adults include anticholinergics, antihistamines, benzodiazepines, chemotherapeutic agents, dopamine agonists, opioid analgesics, psychostimulants and steroids [8].
Method
We searched PubMed and Medline using search terms ‘delirium’, ‘prevention’, ‘management’ and ‘elderly’. Only English language studies published between January 1, 1995 and December 31, 2014 that evaluated the prevention or management delirium in adults who were ≥ 60 years in age were included in the final review. Studies that evaluated the prevention and management of delirium in adults ≤ 60 years in age were used as comparison to studies involving individuals ≥ 60 years in age in certain sections of this review.
Outcomes
The presence of delirium is associated with poorer patient outcomes including a worsening of the nutritional status and the development of; pressure ulcers, aspiration pneumonia and pulmonary emboli [3]. It has been noted that some individuals who develop delirium never return their premorbid level of cognitive functioning [3] Delirium also results in greater burden of care on the nursing staff, longer lengths of hospital stay and greater cost of hospitalization [7,9]. Delirium increases the risk for dementia, hospitalization, institutionalization and death [3,9-11]. The average medical care cost for individuals with delirium is more than two-and-a half times the cost for individuals without delirium [12]. The annual expenditure borne by United States Medicare for hospital stay due to delirium is approximately $7 billion whereas the total cost to healthcare from delirium ranges between $38 billion and $152 billion every year [3,13].
Assessment
It is noted that despite advances in medical care approximately one-third of the cases of delirium in the elderly goes undiagnosed [9]. Common reasons for this error in diagnosis are poor awareness of the individual’s premorbid cognitive functioning and an ageist attitude towards the elderly where the expectation is that all older adults are generally confused [2]. Limited awareness of the clinical features of delirium, its common co-occurrence with dementia and the lack of formal screening for cognitive impairment during regular medical appointments in the elderly add to the reasons for the under or mis-diagnosis [2].
A clinical diagnosis of delirium requires evaluation of all available clinical information, behavioral assessments and cognitive assessments [3,14]. A clinical history evaluates the symptom onset, identifies underlying medical/neurological disorders and the medications and/or drug effects causing delirium. Cognitive evaluation describes the type and extent of cognitive deficits. A physical examination and laboratory data identify possible medical, neurological or surgical disorders as causes for delirium [2,3,15].
Current evidence indicates that rating scales are useful in detecting delirium and assessing its severity [14]. Among the available screening tools, Confusion Assessment Method (CAM) has the most robust evidence in support of its use as a bedside screening instrument [13]. For the identification of delirium cognitive screening tools like the Mini Mental State Examination (MMSE) has been found to be least useful. In addition to the CAM, the Confusion Assessment Method for the ICU (CAM-ICU), the Nursing Delirium Screening Scale (Nu-DESC) and the Delirium Detection Score (DDS) are other useful screening instruments for delirium [16]. Scales that rate the severity of an episode of delirium include the Delirium Assessment Scale (DAS), Delirium Index (DI), Delirium Rating Scale (DRS), Delirium Rating Scale- Revised-98 (The DRS-R-98), Delirium Severity Scale (DSS), Delirium-O-Meter (DOM) and the Memorial Delirium Assessment Scale (MDAS) [17].
Due to the acute and often fluctuant presentation of its symptoms, diagnosing delirium using only the clinical information may result in the condition being missed [18]. It is most prudent to make a diagnosis of delirium by consensus or by utilizing an experienced clinician who screens for delirium using a reliable screening instrument like the CAM and has access to reliable clinical information from multiple observation points. A diagnosis of delirium can be confirmed by using standardized diagnostic criteria like the Diagnostic and Statistical Manual of Mental Disorders 5 (DSM 5) [1].
Prevention
It has been noted in the literature that more than one-third of the cases of delirium may be preventable [3]. Both nonpharmacological and pharmacological interventions have shown benefit in the prevention of delirium in the elderly [19]. In this section, we only included studies on the prevention of delirium that were specifically conducted in older individuals and were either pivotal trial, randomized controlled trials (RCTs), systematic reviews or meta-analyses.
Non-pharmacological
In a landmark study, Inouye et al compared the efficacy of multicomponent targeted risk factor intervention (MTI) strategy versus usual care (UC) in individuals who were 70 years or older in age [20]. The individuals in the MTI group received a standardized protocol for the management of six major risk factors for delirium including cognitive deficits, sleep impairment, ambulatory difficulties, visual deficits, hearing problems and dehydration. Usual care involved standard hospital services that were provided by physicians, nurses and the support staff on the medical units. Individuals in the MTI group were found to have lower incidence of delirium, odds ratio (OR) of 0.60, 95% confidence interval (CI), 0.39 to 0.92, less total number of days with delirium (105 vs. 161, P=0.02) and lower total number of episodes of delirium (62 vs. 90, P=0.03) when compared to the UC group. However, the severity of delirium and the recurrence rates were not significantly different between the two groups. Furthermore, there were short-term and long-term cost savings of $831 per hospitalization and approximately $10,000 per year in the intervention group when compared to the UC group [21,22].
In an RCT of individuals ≥ 65 years in age who had surgical repair for hip fracture, the investigators found that the incidence of delirium in the group receiving proactive geriatric consultation (PGC) was 32% when compared to 50% in the UC group, a relative risk (RR) of 0.64, 95% CI, 0.37 to 0.98 [23]. The proactive geriatric consultation also prevented one case of delirium for every 5.6 patients evaluated.
In a trial by Caplan et al, older adults who were referred for geriatric rehabilitation were randomized to two groups [24]. One group received home rehabilitation whereas the other group received rehabilitation at a hospital ward. The investigators found that the group receiving rehabilitation at home had lower odds of developing delirium during rehabilitation, OR, 0.17, 95% CI, 0.03 to 0.65; shorter duration of rehabilitation, 15.97 days vs. 23.09 day, P=0.0164 and used less hospital bed days, 20.31 versus 40.09, P ≤ 0.0001 when compared to the hospital group. Additionally, patient satisfaction was greater in the home group when compared to the hospital group, P=0.0057.
In a systematic review by Milisen et al that included data from three controlled studies and one a before-after study, the investigators found that prevention strategies reduced the incidence of delirium in both surgical and medical patients [25]. In addition these strategies reduced the duration and severity of delirium and improved functional status. The investigators concluded that non-pharmacological interventions to prevent delirium are effective and should be implemented via the synergistic cooperation between the various healthcare disciplines.
In a meta-analysis evaluating the effectiveness of interventions for the prevention of delirium in older individuals in long term care (LTC), the investigators found only one RCT that met the inclusion criteria [26]. In this study, a computerized system was used to identify medications that may contribute to risk of delirium. This identification triggered a pharmacist-led medication review following which these medications were discontinued. The discontinuation of potentially harmful medications led to a reduction in incidence of delirium, hazard ratio (HR), 0.42, 95% CI, 0.34 to 0.51.
In a meta-analysis that included data from seven studies found that multicomponent interventions reduce the incidence of delirium, RR, 0.73, 95% CI, 0.63 to 0.85, P<0.001 in older adults [27]. Additionally, the investigators found that multicomponent interventions reduced the duration of delirium, the length of hospital stay and mortality rates although these effects did not reach statistical significance.
The data from these six studies indicate that non-pharmacological management strategies appear to reduce the incidence, duration and severity of delirium in older adults. These strategies appear to be well tolerated in older adults. Possible mechanisms for efficacy include the early identification and management risk factors for delirium and early rehabilitation of individuals resulting in favorable outcomes [20-27] (Table 1).
Pharmacological
Antipsychotics
A meta-analysis that obtained data from five trials found that prophylaxis with antipsychotics reduces the incidence of delirium in older individuals receiving surgical procedures by about 50% when compared to placebo, RR, 0.51, 95% CI, 0.33 to 0.79, P<0.01 [28]. Data from four of the five studies indicated that prophylaxis with antipsychotic medications resulted in a reduction in the incidence of delirium; number needed to treat (NNT), 4.00 to 12.6. Information from this study suggests that the short-term use of antipsychotic medications to prevent delirium appears to be safe with none of the studies reporting any serious adverse effect.
In a meta-analysis by Fok et al the investigators included a total of 6 RCTs that evaluated the efficacy of antipsychotic medications in the prevention of delirium in older adults. These studies recruited a total of 1710 subjects with a mean age ranging from 60.7 to 86.4 years [29]. The investigators found that the weighted odds of individuals who were treated with antipsychotics developing delirium were 0.44 when compared to the individuals who were treated with placebo with a NNT of 7. The investigators calculated the break-even point for baseline delirium risk below which treatment with antipsychotic medications can become potentially harmful as being 18% delirium risk. One of the two studies that evaluated delirium severity and duration indicated that treatment with haloperidol did not reduce the incidence of postoperative delirium but reduced the severity and duration of delirium. Five of the six studies were also included in the metaanalysis by Teslyar et al. [28].
Available data from these two meta-analyses indicates that antipsychotics may be beneficial in the prevention of delirium in the elderly especially among post-operative cases. These medications also appear to be well tolerated in older adults. Possible mechanisms by which antipsychotic medications prevent delirium are a modulation of dopaminergic and serotonergic activity [28,29]. In addition, their use may reduce agitation/ aggression in these individuals whereby decreasing the need for physical restraints and additional pharmacological management strategies.
Cholinesterase inhibitors
No meta-analysis evaluating the use of cholinesterase inhibitors for the prevention of delirium in the elderly were noted in our review of the literature. However, we found five RCTs that evaluated the effectiveness of cholinesterase inhibitors in the prevention of delirium in older adults. The studies are arranged in this section in ascending order of the year of publication.
In a double-blind, placebo-controlled trial eighty individuals (mean age, 67.2 years) were randomized to receive donepezil or placebo for 14 days prior to surgery and 14 days post-surgery [30]. The investigators found that 18.8% of subjects met the DSM-IV criteria for delirium on at least 1 postoperative day. There were no significant differences noted between the donepezil and placebo groups on the incidence of delirium, P=0.69. Subsyndromal delirium was identified on at least 1 postoperative day for 68.8% of subjects and when it occurred, it lasted for ≤ 2 days. There was no difference between the two groups for the incidence of subsyndromal delirium, P=0.57. Additionally, there was no difference noted in the rates of discontinuation of the study medication between the groups where approximately onefourth of individuals in each group stopped the study medication after randomization.
In a double blind, placebo controlled and parallel group trial, thirtythree individuals with a mean age of 67 years were randomized to receive either donepezil 5 mg or placebo immediately following elective total hip replacement surgery and every 24 hours for a further three days [31]. The investigators found that the incidence of delirium was 9.5% in the donepezil group when compared to 35.7% in the placebo group, relative risk (RR), 0.29, 95% CI, 0.06 to 1.30. Donepezil was well tolerated in this study with no statistically significant differences in the rates of adverse effects between the two groups.
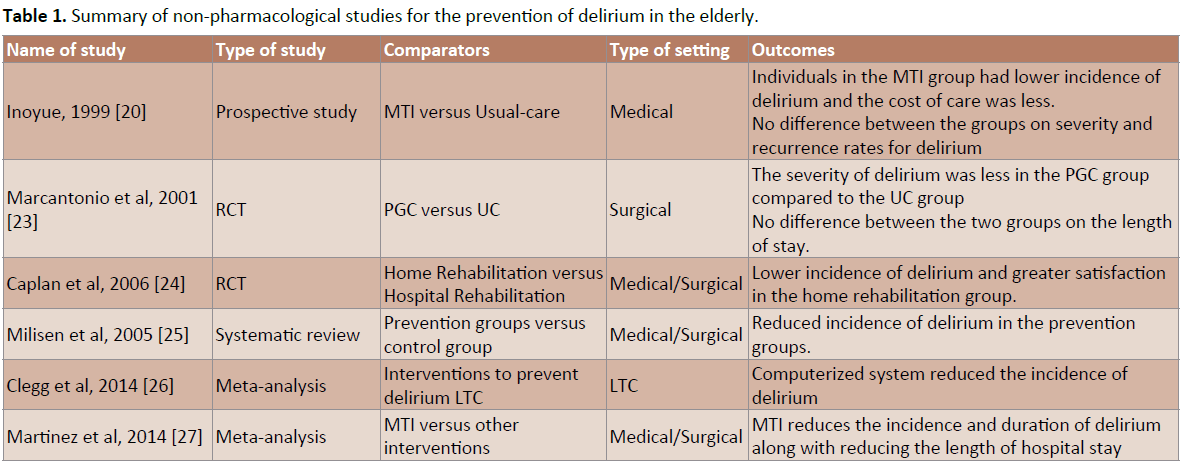
Table 1: Summary of non-pharmacological studies for the prevention of delirium in the elderly.
In a double-blind, randomized, placebo-controlled trial, one hundred twenty individuals ≥ 65 years in age who were undergoing elective cardiac surgery were randomized to receive either 3 doses of 1.5 mg of oral rivastigmine per day or placebo starting the evening prior to surgery and to continue treatments until the evening of the sixth postoperative day [32]. The investigators found that the incidence of delirium was 32% in the rivastigmine group when compared to 30% in the placebo group, P=0.8. The investigators found no treatment effect on the time course on the Mini-Mental State Examination scores (P=0.40) and on the clock drawing test (CDT, P=0.80). Additionally, side-effects were greater in the rivastigmine groups when compared to the placebo group but were not statistical significant.
Marcantonio et al completed a double-masked placebo-controlled trial where they included sixteen individuals ≥ 70 years in age who had hip fracture [33]. The participants were randomized to receive either donepezil 5 mg a day or placebo within 24 hours of surgery, preoperatively or postoperatively. The investigators continued the treatment for 30 days or until side effects or the clinical situation required termination from the study protocol. All participants were reassessed on each postoperative hospital day and then at 2, 4 and 6 weeks after their enrollment in the study. The investigators found that the incidence of delirium was no different between the donepezil and the placebo groups during the hospital stay or at weeks 2, 4 and 6 of follow-up. They also found that donepezil was less well tolerated than placebo in terms of total number of side effects (P=0.04), insomnia (P=0.04) and diarrhea (P=0.06).
In an RCT, individuals who were ≥ 65 years in age and awaiting elective surgery were randomized to receive either rivastigmine 5-cm2 transdermal patch or a placebo patch [34]. A total of twentyeight individuals completed the study: 11 in the rivastigmine group and 17 in the placebo group. There was no difference noted in the incidence of delirium between the two groups, P=0.78. The study was stopped prematurely due to a warning letter by the manufacturer of rivastigmine indicating the possibility of increased mortality with the oral administration of the drug in critically ill patients. Cognitive functioning as evaluated by the MMSE scores was higher in the rivastigmine group when compared to the placebo group on postoperative days one and two.
A summary of five RCTs of cholinesterase inhibitors indicates that in four of the studies, the investigators did not find benefit for the active drug when compared to placebo for the prevention of delirium. The study by Sampson et al showed a trend towards benefit for the donepezil group when compared to the placebo group on the incidence of delirium and the length of hospital stay but both outcomes did not attain statistical significance [31].
Melatonin and melatonin agonist
Chakraborti et al in their systematic review concluded that melatonin use may prevent the onset of delirium in older adults [35]. Additionally the investigators also found that ramelteon- a melatonin agonist was found to reduce the incidence of delirium in one study [35]. They also found that that both melatonin and ramelteon were well tolerated in these studies. Both melatonin and ramelteon assist in resetting the circadian rhythm disturbance thereby preventing the development of delirium in vulnerable older adults [35].
Additional study
In a structured-analysis of prevention strategies for delirium in the elderly, the investigators found a total of sixteen-relevant studies of which ten were RCTs [36]. The investigators found no difference in the effectiveness between the pharmacological interventions versus multi-component interventions versus onecomponent interventions: OR, 0.58, 95% CI, 0.39 to 0.87 versus OR, 0.59, 95% CI, 0.38 to 0.92 versus OR, 1.05, 95% CI, 0.09 to 11.57 in the prevention of delirium. The interventions were as effective in non-surgical cases as in surgical cases, OR, 0.59, 95% CI, 0.40 to 0.89 versus OR, 0.65, 95% CI, 0.41 to 1.04. The investigators found that the interventions were more effective in studies with a high incidence of delirium in the control group (>30%) than with a low incidence of delirium (<30%), OR, 0.34, 95% CI, 0.16 to 0.71 versus OR, 0.76, 95% CI, 0.60 to 0.97.
A summary of available evidence indicates that nonpharmacological and pharmacological strategies to prevent delirium have shown benefit in older individuals. These strategies appear to be well tolerated by the older adults. Additionally, proactive geriatric consultation and home rehabilitation show benefit in preventing delirium in older adults. Furthermore, these interventions may reduce the duration of delirium and the length of hospital stay (Table 2).
Treatments
The first-line of management for older adults with delirium are non-pharmacological strategies [3,15]. Common strategies that have shown benefit include the making eye contact and the use of clear verbal instructions when communicating with the individuals with delirium. Additionally, frequent reorientation and touch decreases confusion and anxiety in the individuals [3]. Visual and hearing loss should be minimized by use of assistive devices. Care should be provided in a non-stimulating environment which is quiet and has adequate but soft lighting [18]. In addition, the room and staff changes should be minimized. The use of physical restraints for behavioral symptoms should be limited [6]. Similar to the prevention section, we only included data from studies that were specifically conducted in older individuals and were either pivotal trials, RCTs, systematic reviews or meta-analyses.
Non-pharmacological
A review of literature found three RCTs and one systematic review that included data from these three RCT evaluating the efficacy of non-pharmacological interventions for the treatment of delirium in the elderly.
In an RCT, Cole et al found that geriatric psychiatry consultation (GPC) was superior to usual care in reducing the severity of delirium over an eight week period [37]. Additionally, more individuals in the control than in the treatment group cases were discharged after 4 and 8 weeks and the number of cases discharged home were twice as many in the treatment group when compared to the control group.
In a follow-up RCT, Cole et al found that consultation by a geriatrician or a psychiatrist and follow-up by a liaison nurse was superior to usual care in improving the level of confusion in individuals with delirium [38]. In addition, individuals in the treatment group had greater improvements in behavioral symptoms when compared to the control group. However, the investigators did not find any difference between the treatment and the control groups in the use of restraints, the length of hospital stay, discharge to a supervised care setting and mortality rates.
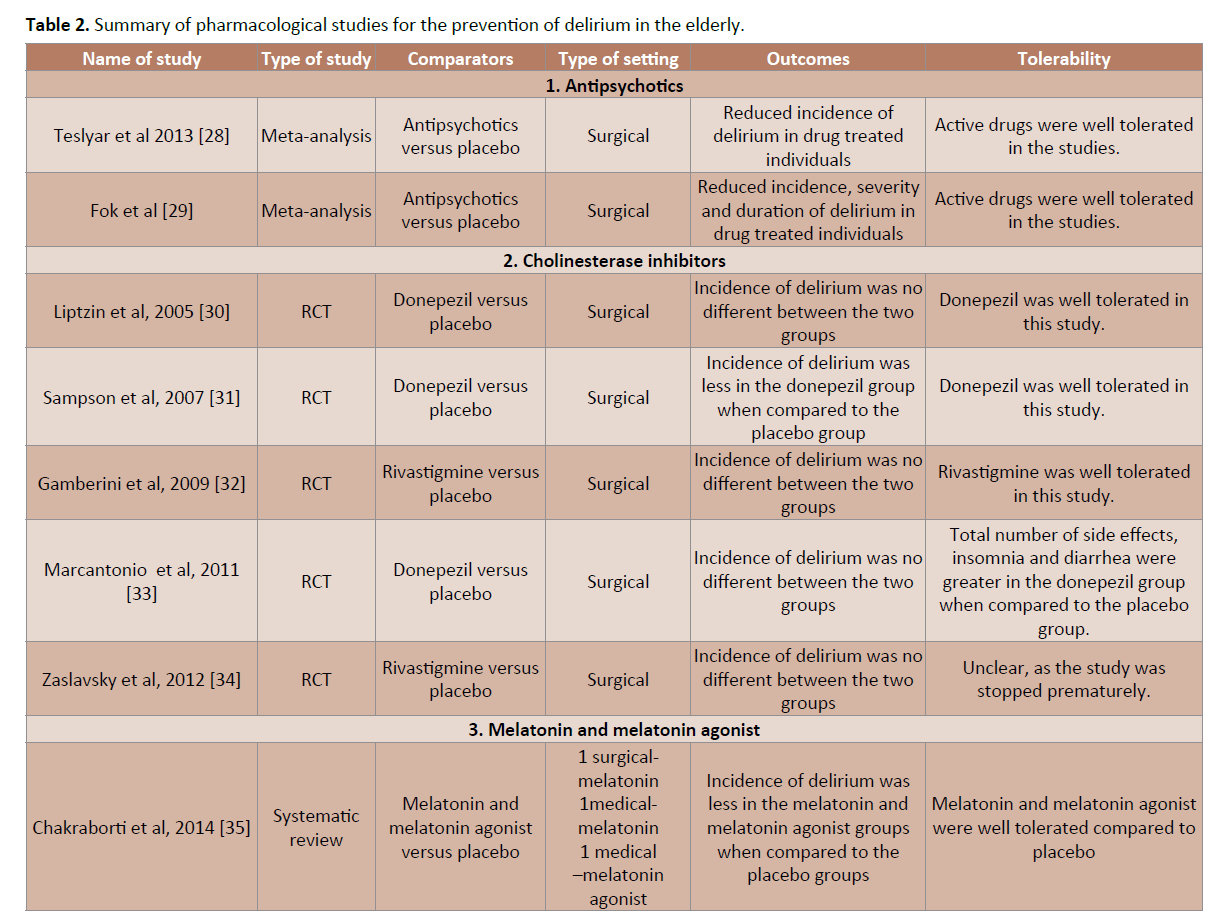
Table 2:Summary of pharmacological studies for the prevention of delirium in the elderly.
In a longitudinal prospective study to evaluate the benefits of a nurse-led interdisciplinary intervention program for delirium in individuals with hip-fracture, the investigators found a shorter duration of delirium (P=0.03) and a decrease in severity of delirium (P=0.0049) in the intervention group when compared to the control group [39]. Also, there was higher cognitive functioning and a trend toward decrease in length of stay postoperatively among delirious patients in the intervention group when compared to the control group. However, there was no benefit for the interventions on the incidence of delirium, activities of daily living (ADL) rehabilitation or the risk of mortality when compared to the control group.
In the trial by Marcantonio et al where individuals ≥ 65 years in age who had surgical repair for hip fracture, received either proactive geriatrics consultation (PGC) or usual care (UC), the investigators found that the percentage of cases of severe delirium was greater in the UC group when compared to the PGC group, 29% vs. 12%, RR of 0.40, 95% CI, 0.18 to 0.89 [40]. A subgroup analysis indicated that the consultation was most effective in reducing delirium in individuals without preexisting dementia or functional impairments.
In a trial by Cole et al, the investigators randomized older adults with delirium admitted to general medical units to an intervention group where they received follow-up by a geriatric specialist and an intervention nurse who was involved in liaison work with the consulting team, physicians, nurses and the patients family or to care as usual group [41]. No significant differences were noted between the two groups on the following outcomes: time to symptom improvement, the rate of improvement of delirium severity, functional outcomes, length of hospital stay, the rate of discharge, living arrangements after discharge from hospital and survival rate within 8 weeks after enrolment in the study.
In a systematic review by Milisen et al, the investigators included data from three randomized controlled trials (mentioned earlier) for the treatment of delirium [25]. Based on the review of the data, the investigators concluded that strategies to treat delirium were ineffective in older adults admitted to medical services. But in older individuals admitted for surgery, treatments reduced the duration and severity of the delirium episode. However, none of intervention strategies produced beneficial effects on the length of hospital stay or mortality rates. The investigators concluded that non-pharmacological interventions to prevent delirium are more effective than treatments and should be implemented via the synergistic cooperation between the various healthcare disciplines.
The data from these four studies indicate that nonpharmacological management strategies appear to reduce the severity and duration of delirium in older adults. They appear to be well tolerated in older adults. Possible mechanisms for efficacy include the early identification and management risk factors for delirium and early rehabilitation of individuals resulting in these favorable outcomes (Table 3).
Pharmacological
The use of pharmacotherapy in individuals with delirium targets the treatment of its underlying causes [1]. Pharmacotherapy may also be used in cases where the non-pharmacological interventions have failed [3]. Medications are usually prescribed when individuals with delirium exhibit agitation, aggression, paranoia and hallucinations that place them and their caregivers at risk of imminent harm [3]. We have only used data from RCTs, systematic reviews and meta-analysis to evaluate the efficacy of pharmacotherapy for the treatment of delirium in the elderly.
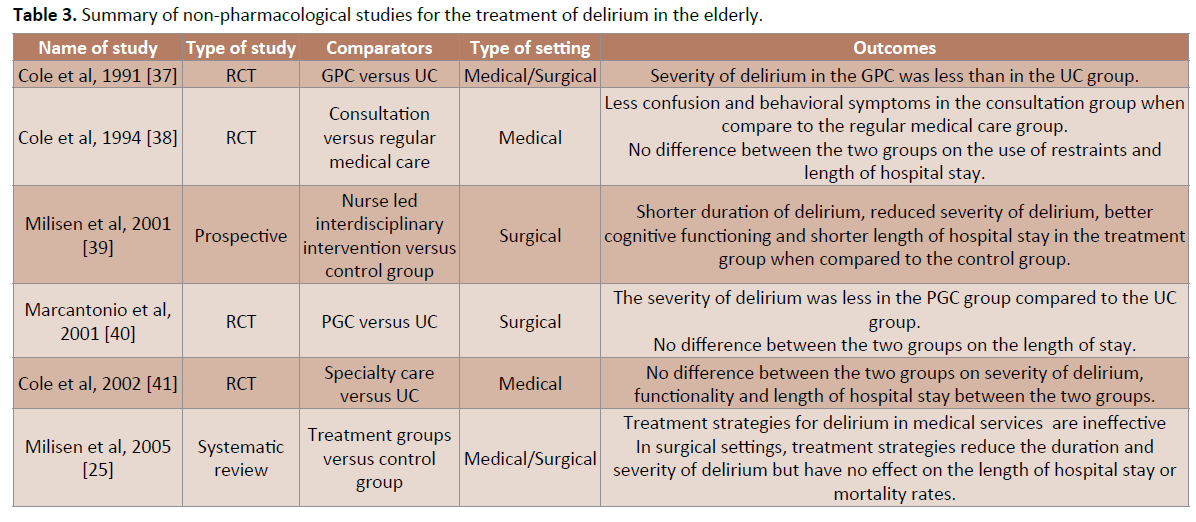
Table 3:Summary of non-pharmacological studies for the treatment of delirium in the elderly.
Antipsychotics
A review of the literature indicated that there are four RCTs evaluating the effectiveness of antipsychotics in the treatment of delirium in older adults. Additionally, we found one meta-analysis and one systematic review on the use of antipsychotics to treat delirium in older individuals.
In a double blind trial, twenty-four individuals with delirium and a mean age of 66 years were randomly assigned to receive a flexible dose regimen of haloperidol or risperidone for seven days [42]. At the end of the study, the mean doses of haloperidol and risperidone were 1.71 mg a day and 1.02 mg a day respectively. The severity of delirium (MDAS scores) were significantly reduced in both groups by the end of the study, P<0.05 but there were no significant differences noted between the two groups, P=0.51. Additionally, the group-by-time effect was not significant, P=0.14. Furthermore, no significant differences in the frequency of response to the drugs in either group was noted, P=0.11. Haloperidol was well tolerated in the study with none of the subjects presenting any clinically significant adverse effects.
In a randomized, placebo controlled trial one hundred and seventy five individuals with an average age of 74 years were randomized to receive olanzapine (1.25 mg to 2.0 mg a day), haloperidol (2.5 mg to 10.0 mg a day) or placebo for seven days [43]. A decrease in delirium severity (DRS scores) by 7th day was noted in all three groups at the end of the study period when compared to baseline, P<0.01. Additionally, the DRS scores in the olanzapine and haloperidol groups were reduced by 72.2% and 70.4% respectively when compared to 24.7% in the placebo group, P<0.05 & P<0.01 respectively by Day 7. The DRS scores reduced significantly after 2.78 ± 1.85 days of treatment in the olanzapine group when compared to 3.40 ± 1.62 days of treatment in the haloperidol group and 5.18 ± 1.54 days in the placebo group, P<0.001 & P<0.01 respectively. The investigators found that 18.9% of the individuals in the olanzapine group had drowsiness when compared to 22.2% in the haloperidol group, P>0.05. Additionally, dry mouth was noted in 2.7% of the individuals in the olanzapine group when compared to 16.7% in the haloperidol group, P<0.01. Dystonia was noted in 2.7% of the individuals in the olanzapine group when compared to 31.9% of the individuals in the haloperidol group, P<0.01. A total of one individual dropped out from the olanzapine group when compared to 3 individuals in the haloperidol group, P>0.05.
In a randomized, double-blind, placebo-controlled trial 430 individuals ≥ 70 years in age and awaiting hip-surgery were randomized to receive haloperidol 1.5 mg a day or placebo preoperatively (at admission) and continued for up to 3 days postoperativel [44]. The investigators noted that the overall incidence of postoperative delirium in the study to be 15.8%. They also found that postoperative delirium occurred in 15.1% of the individuals in the haloperidol group when compared to 16.5% of the individuals in the placebo group, relative risk (RR), 0.91, 95% CI, 0.6 to 1.3. Additionally, they investigators found that the severity of delirium in the haloperidol group to be less than in the placebo group, P<0.001. The duration of delirium was 5.4 days in the haloperidol group when compared to 11.8 days in the placebo group, P<0.001. Furthermore, the mean number of days in the hospital for individuals in the haloperidol group was 17.1 ± 11.1 when compared to 22.6 ± 16.7 for the placebo group, P<0.001. The investigators did not identify any medication-related side effects during the study period including akathisia or sedation. This study had been included in the meta-analysis by Teslyar et al [28] as it involved a component of prevention of delirium in addition to its treatment.
Maneeton et al completed a double-blind trial in fifty-two individuals subjects (35 males and 17 females) who were randomized to receive 25 mg to 100 mg a day of quetiapine (n=24) or 0.5 mg to 2.0 mg a day of haloperidol (n=28) for a total of seven days [45]. The investigators found that during the study period, delirium severity scores were not significantly different between the quetiapine or haloperidol groups (P=0.59). Additionally, they did not find any significant difference between the response (P=0.97) or remission rates (P=0.96) between the groups. The times to first response of delirium was not significantly different between groups, P=0.61. The mean time to remission was also not significantly different between the two groups P=0.14. The time to first remission of delirium was not significantly different between two groups, P=0.68. The total sleep time (P=0.74) and the scores on the Modified (nine-item) Simpson–Angus scale (assessing extrapyramidal symptoms) (P=0.51) were also not significantly different between groups.
In the meta-analysis by Lonergan et al, the investigators compared the efficacy and adverse effects of haloperidol to risperidone, olanzapine, quetiapine and placebo in the treatment of delirium [46]. They included data from three trials all of which were done in the older adults [40-42]. They found that the reduction in delirium scores were not significantly different when comparing the effect of low dose haloperidol (<3.0 mg per day) with olanzapine and risperidone, odds ratio, 0.63, 95% CI, 1.029- 1.38, P=0.25. Low dose haloperidol did not have a higher incidence of adverse effects when compared to the atypical antipsychotics. High dose haloperidol (>4.5 mg per day) in one study was associated with greater incidence of extrapyramidal adverse effects when compared with olanzapine. In one study, low dose haloperidol decreased the severity and duration of delirium in post-operative patients, although the incidence of delirium did not differ. There were no controlled trials that compared quetiapine to haloperidol for the treatment of delirium.
In a systematic review by Ozbolt et al, the investigators evaluated the efficacy of atypical antipsychotics for the treatment of delirium in the elderly [47]. The investigators found that risperidone and olanzapine were effective in treating episodes of delirium in over 70% of the cases in a dosage range of 0.5 to 4 mg daily and 2.5 to 11.6 mg daily respectively. They opined that despite limited number of studies for quetiapine, this medication appears to be safe and effective for the treatment of cases of delirium and as an alternative to other atypical antipsychotic medications. Atypical antipsychotic medications were also better tolerated than haloperidol in these trials. The investigators concluded that atypical antipsychotic medications have similar efficacy as haloperidol for the treatment of delirium in the elderly and are better tolerated.
Available data from these studies indicate that antipsychotics appear to reduce the severity and the duration of delirium in older adults. These medications also appear to be well tolerated in this population. Possible mechanisms by which antipsychotic medications prevent delirium are a modulation of dopaminergic and serotonergic activity [28,29]. In addition, their use may reduce agitation/aggression in these individuals whereby decreasing the need for physical restraints and additional pharmacological management strategies.
Cholinesterase inhibitors
A review of evidence indicates that there are six RCTs that have evaluated the efficacy of cholinesterase inhibitors in the treatment of delirium in older adults. Four of the studies also included prevention of delirium as an outcome measure. These four studies have been described earlier in this article.
In the study by Liptzin et al, the investigators found that when delirium was present in the participants, it lasted only 1 day and there was no difference between the donepezil and the placebo treated groups, P=0.12 [30]. Also, there was no difference between the two groups for the duration of subsyndromal delirium, P=0.28. There were no difference between the groups on the length of hospital stay, P=0.09 and the proportion of individuals who were discharged from the hospital.
In the study by Sampson et al, the investigators found that the mean length of stay was 9.9 days in the donepezil group when compared to 12.1 days in the placebo group, difference in means -2.19 days, 95% CI, -0.39 to 4.78 [31]. The severity of delirium as measured on the DSI was mild in both the groups.
In the study by Gamberini et al the investigators found that there was no significant difference between the length of hospital stay between the two groups, P=0.30 [32]. Additionally, there was no significant difference in the number of patients receiving haloperidol P=0.90 or lorazepam P=0.60 in either groups.
In a double-blind, placebo-controlled individuals ≥ 65 years in age identified as having delirium using the Confusion Assessment Method (CAM) were randomized to receive oral rivastigmine 1.5 mg once a day and then increasing to 1.5 mg twice a day after seven days or identical placebo [48]. The maximum length of the study period was twenty-eight days. The primary outcome was duration of delirium as evaluated by the CAM. Other measures were the length of hospital stay and the discharge destination. At the end of the study period all the individuals in the rivastigmine did not meet the criteria for delirium on the CAM whereas three individuals in the placebo group met the criteria for delirium. The investigators found no significant difference between the two groups in the duration of delirium, P=0.5. Rivastigmine was well tolerated in the study with none of the individuals in the active drug treatment group reporting any adverse events.
Van Eijk et al conducted an RCT in individuals aged ≥ 18 years (mean age, 69 years) who were admitted to intensive care units [49]. The participants were randomized to receive increasing doses of rivastigmine or placebo, starting at 1·5 mg rivastigmine twice daily and then increased to 6 mg of rivastigmine twice daily from day 10 onwards or placebo as an adjunct to usual care with haloperidol [47]. The investigators found that the mean duration of delirium was not different between the two groups in the study, P=0.06. The severity of delirium was less in the placebo group when compared to the rivastigmine group, P=0·0040. The length of stay in the ICU was less in the placebo group when compared to the rivastigmine group, P<0·0001. However, the length of stay in the hospital was not significantly different between the two groups, P=0.06. Three times more individuals died in the rivastigmine group when compared to the placebo group during the study period, 12 versus 4, P=0.07. The trial was halted prematurely because of increased mortality in the rivastigmine group when compared to the placebo group.
In the trial by Marcantino et al where sixteen individuals ≥ 70 years in age with hip fracture were randomized to receive donepezil 5 mg a day or placebo within 24 hours of surgery, preoperatively or postoperatively, the investigators found that the severity of delirium was no different between the donepezil and the placebo groups during the hospital stay and at weeks 2, 4 and 6 [33].
In a meta-analysis Overshott et al included one study that evaluated the efficacy and safety of cholinesterase inhibitors in the treatment of delirium [48]. The investigators included the Liptzin et al [30] study that found no significant difference between the active treatment group and placebo group on the duration of delirium; 1.0 day versus 1.3 days. There were no other outcomes measured in these patients. The investigators concluded that the evidence from controlled trials for the efficacy of donepezil in the treatment of delirium was lacking.
A summary of evidence indicates that three of the four studies that evaluated the efficacy of acetylcholinesterase inhibitors in the prevention and management of delirium did not find benefit for the drugs in the prevention or management of delirium [30-32]. One study that evaluated the efficacy of an acetylcholinesterase inhibitor in the management of delirium found no benefit for the active drug in reducing the duration of delirium [32]. In another study, the investigators found that the duration of delirium and the length of hospital stay were longer in the haloperidol plus rivastigmine group when compared to the haloperidol plus placebo group [34]. (Table 4)
Melatonin and melatonin agonist
Data available from one study of older adults awaiting surgery indicates that melatonin may be beneficial in managing the symptoms of delirium [35]. Melatonin was well tolerated in this study. Possible mechanism for the efficacy of melatonin in the management of delirium is the resetting of the circadian rhythm in these individuals there by reducing the duration and severity of the delirious episode [35].
Benzodiazepines
In our review of the literature, no controlled studies that investigated the use of benzodiazepines for the treatment of delirium in the elderly were noted. However, a meta-analysis by Lonergan et al did evaluate the effectiveness of benzodiazapines for the treatment of non-alcohol withdrawal related delirium in younger adults [51]. In this meta-analysis the investigators included one trial that compared lorazepam to dexmedetomidine, a selective alpha-2-adrenergic receptor agonist for the treatment of delirium among mechanically ventilated individuals in intensive care units. The investigators found that the individuals in the dexmedetomidine group had greater number of deliriumand coma-free days when compared to individuals treated with lorazepam, P=0.01. The investigators also found two partially controlled studies that found no benefit for alprazolam when compared to antipsychotics or lorazepam when compared to haloperidol and chlorpromazine for the treatment of delirium. The lorazepam group had greater side-effects when compared to the haloperidol group. The investigators concluded that there is no data supporting the use of benzodiazepines for the treatment of non-alcohol withdrawal related delirium among hospitalized individuals.
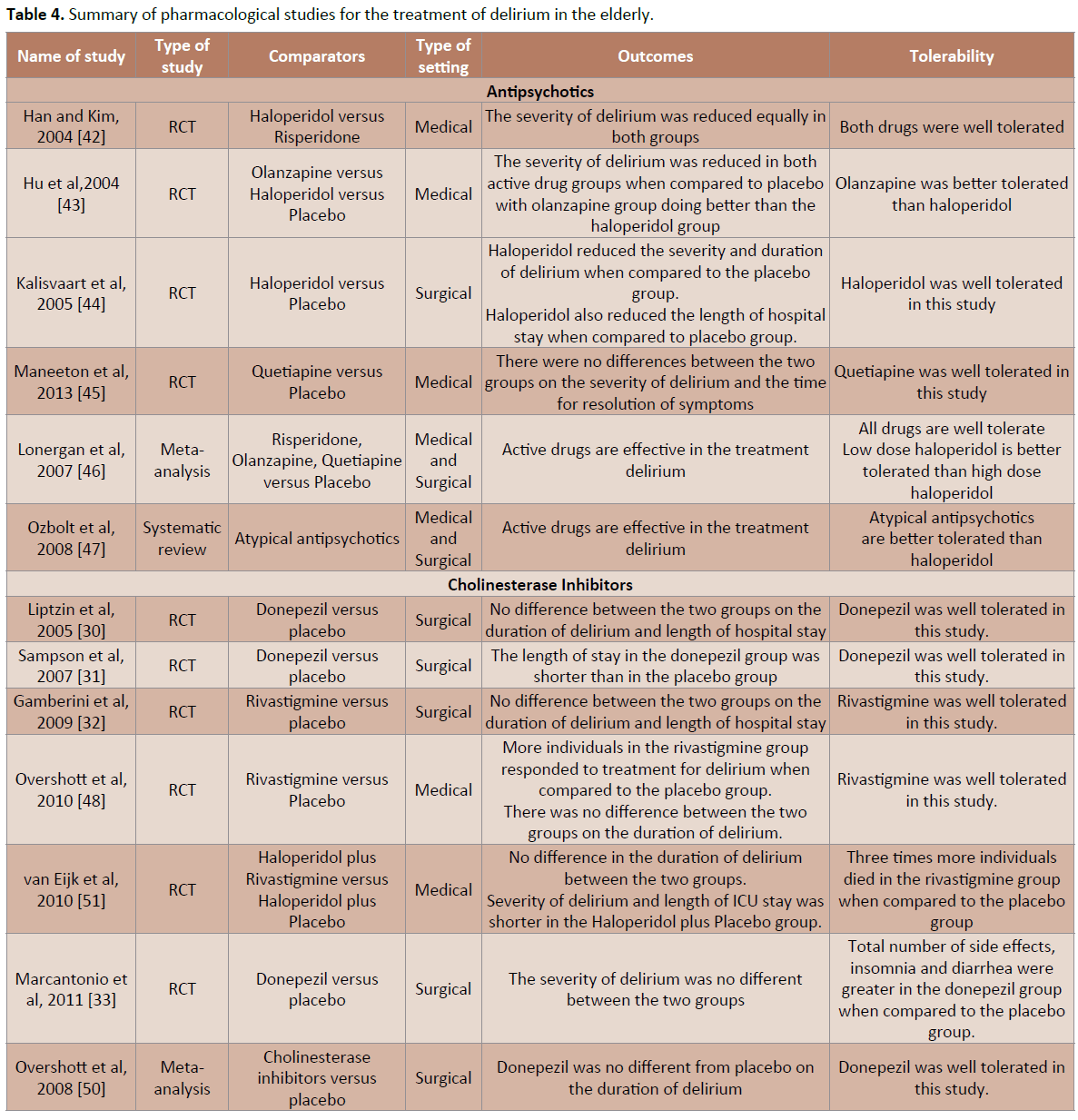
Table 4:Summary of pharmacological studies for the treatment of delirium in the elderly.
Comparative studies not specific to the elderly with delirium
In a review of the literature, we found two systematic reviews that evaluated the efficacy of pharmacological agents for the prevention and management of delirium. In the first review, Campbell et al identified thirteen studies that evaluated the efficacy and safety of pharmacologic interventions for the prevention or management of delirium [52]. The investigators found that neither cholinesterase inhibitors nor procholinergic drugs were effective in the prevention of delirium. They also did not find any difference in the efficacy or safety among the various typical and atypical antipsychotic medications for the treatment of delirium. Available data indicated that the use of haloperidol, risperidone, gabapentin or a mixture of sedatives in individual undergoing surgical procedures may prevent delirium or decrease its severity and/or its duration. The investigators concluded that the prevention of delirium can be achieved via multiple means and that there is no evidence indicating the superiority of atypical antipsychotics over haloperidol in the management of delirium.
In the second review by Friedman et al that evaluated data from forty-five studies, the investigators found that pharmacological strategies are better for the prevention of delirium rather than its treatment [53]. Evidence indicated efficacy for haloperidol, atypical antipsychotics, iliac fascia block, gabapentin, melatonin, lower levels of intraoperative propofol sedation, a single dose of ketamine during anesthetic induction and dexmedetomidine for the prevention of delirium.
Summary of Evidence
Available data from studies specific to older adults indicates that prevention rather than the management of symptoms of delirium results in better clinical outcomes in older adults with delirium. A review of evidence indicates that nonpharmacological and pharmacological strategies are beneficial in the prevention of delirium. Multi-component targeted risk factor intervention (MTI) has the strongest evidence followed by geriatric consultation and home rehabilitation among the non-pharmacological interventions for delirium in older adults. The use of antipsychotics for prevention of delirium in surgical patients has the strongest evidence base followed by the use of melatonin/melatonin agonist and cholinesterase inhibitors among the pharmacotherapeutic interventions.
Data for the treatment of symptoms of delirium in older adults indicates that non-pharmacological interventions that have shown benefit include geriatric-medicine/psychiatry and/or nursing consultation especially in older adults needing surgical interventions. Among the pharmacological interventions, the most robust data is on the use of antipsychotic (typical and atypical) medications followed by cholinesterase inhibitors. Melatonin has shown benefit in treatment of symptoms of delirium from one study. Pharmacotherapy also resulted in a reduction in severity and duration of delirium in some cases along with a shorter length of hospital stay.
The American Psychiatric Association (APA) recommends lowdose haloperidol as a first-line agent for the symptomatic management of delirium [54]. Atypical-antipsychotic medications may be used as an alternative to haloperidol in individuals who have allergy to haloperidol or are not ideal candidates for typical antipsychotic agents, e.g., individuals with Parkinson’s disease, Dementia with Lewy bodies and Parkinson Plus Syndromes.
Available evidence indicates that the use of antipsychotic medications in older adults especially in those individuals with dementia may cause cerebrovascular adverse events (CVAEs) or death [55]. Current data indicates that the risk of CVAEs is higher in the drug treated group when compared to placebo groups. Existing data indicate that the risk of CVAEs and death are similar for both atypical and typical antipsychotic agents when used in individuals with dementia. The time frame for which the risk of CVAEs remains elevated is about 20 months. The risk for death appears to be elevated in the first 30 days and possibly for upto 2 years. In view of these risks, antipsychotics should be used carefully in the elderly especially those individuals with dementia. In addition, the use of these medications in older adults with delirium should be closely monitored as dementia and delirium are highly comorbid conditions.
Our review of evidence indicates that medication classes other than antipsychotics appear to be fairly well tolerated by older adults with delirium. However, one rivastigmine study had to be discontinued prematurely due to greater mortality rates in the rivastigmine group when compared to the placebo group [49]. Data on the duration of these trials indicates that these trials lasted between a few days to up-to 8 weeks. We did not find any difference between the trial outcomes based on the duration of the trial.
Conclusions
Delirium, a common disorder in the elderly is often undiagnosed and results in significant morbidity and mortality in this population. A thorough clinical history, a focused physical examination, the appropriate use of common laboratory tests and standardized screening tools like the Confusion Assessment Method (CAM) can aid in the appropriate diagnosis of delirium. Current data indicate that non-pharmacological and pharmacological interventions show benefit in reducing the incidence of delirium and its overall severity. There is data for additional benefits in older individuals with delirium including a reduction in the duration of delirium and the length of hospital stay. Furthermore, these interventions were well tolerated by older individuals with delirium. Evidence evaluated in this review indicates that it would be most prudent to combine non-pharmacological and pharmacological interventions for the prevention and treatment of delirium in the elderly thereby reducing the morbidity and mortality from this condition.
References
- Desk Reference to the Diagnostic Criteria from DSM-5. Washington DC: American Psychiatric Association 2013:292-298.
- Saxena S, Lawley D (2009) Delirium in the elderly: a clinical review. Postgrad Med J 85: 405-413.
- Fong TG, Tulebaev SR, Inouye SK (2009) Delirium in elderly adults: diagnosis, prevention and treatment. Nat Rev Neurol 5: 210-220.
- Miller MO (2008) Evaluation and management of delirium in hospitalized older patients. AmFam Physician 78: 1265-1270.
- Khan BA, Zawahiri M, Campbell NL, Fox GC, Weinstein EJ, et al. (2012) Delirium in hospitalized patients: implications of current evidence on clinical practice and future avenues for research--a systematic evidence review. J Hosp Med 7: 580-589.
- Inouye SK (1999) Predisposing and precipitating factors for delirium in hospitalized older patients. Dement GeriatrCognDisord 10: 393-400.
- Inouye SK, Charpentier PA (1996) Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability. JAMA 275: 852-857.
- Laurila JV, Laakkonen ML, Tilvis RS, Pitkala KH (2008) Predisposing and precipitating factors for delirium in a frail geriatric population. J Psychosom Res 65: 249-254.
- Siddiqi N, House AO, Holmes JD (2006) Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing 35: 350-364.
- Witlox J, Eurelings LS, de Jonghe JF, Kalisvaart KJ, Eikelenboom P, et al. (2010) Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA 304: 443-451.
- Rockwood K, Cosway S, Carver D, Jarrett P, Stadnyk K, et al. (1999) The risk of dementia and death after delirium. Age Ageing 28: 551-556.
- Leslie DL, Marcantonio ER, Zhang Y, Leo-Summers L, Inouye SK (2008) One-year health care costs associated with delirium in the elderly population. Arch Intern Med 168: 27-32.
- Young J, Inouye SK (2007) Delirium in older people. BMJ 334: 842-846.
- Wong CL, Holroyd-Leduc J, Simel DL, Straus SE (2010) Does this patient have delirium?: value of bedside instruments. JAMA 304: 779-786.
- Cole MG (2004) Delirium in elderly patients. Am J Geriatr Psychiatry 12: 7-21.
- Luetz A, Heymann A, Radtke FM, Chenitir C, Neuhaus U, et al. (2010) Different assessment tools for intensive care unit delirium: which score to use? Crit Care Med 38: 409-418.
- Adamis D, Sharma N, Whelan PJ, Macdonald AJ (2010) Delirium scales: A review of current evidence. Aging Ment Health 14: 543-555.
- Zou Y, Cole MG, Primeau FJ, McCusker J, Bellavance F, et al. (1998) Detection and diagnosis of delirium in the elderly: psychiatrist diagnosis, confusion assessment method, or consensus diagnosis? Int Psychogeriatr 10: 303-308.
- Khan BA, Zawahiri M, Campbell NL, Fox GC, Weinstein EJ, et al. (2012) Delirium in hospitalized patients: implications of current evidence on clinical practice and future avenues for research--a systematic evidence review. J Hosp Med 7:580-589.
- Inouye SK, Bogardus ST Jr, Charpentier PA, Leo-Summers L, Acampora D, et al. (1999) A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med 340: 669-676.
- Rizzo JA, Bogardus ST Jr, Leo-Summers L, Williams CS, Acampora D, et al. (2001) Multicomponent targeted intervention to prevent delirium in hospitalized older patients: what is the economic value? Med Care 39: 740-752.
- Leslie DL, Zhang Y, Bogardus ST, Holford TR, Leo-Summers LS, et al. (2005) Consequences of preventing delirium in hospitalized older adults on nursing home costs. J Am GeriatrSoc 53: 405-409.
- Marcantonio ER, Flacker JM, Wright RJ, Resnick NM (2001) Reducing delirium after hip fracture: a randomized trial. J Am GeriatrSoc 49: 516-522.
- Caplan GA, Coconis J, Board N, Sayers A, Woods J (2006) Does home treatment affect delirium? A randomised controlled trial of rehabilitation of elderly and care at home or usual treatment (The REACH-OUT trial). Age Ageing 35: 53-60.
- Milisen K, Lemiengre J, Braes T, Foreman MD (2005) Multicomponent intervention strategies for managing delirium in hospitalized older people: systematic review. J AdvNurs 52: 79-90.
- Clegg A, Siddiqi N, Heaven A, Young J, Holt R (2014) Interventions for preventing delirium in older people in institutional long-term care. Cochrane Database Syst Rev 1: CD009537.
- Martinez F, Tobar C, Hill N (2015) Preventing delirium: should non-pharmacological, multicomponent interventions be used? A systematic review and meta-analysis of the literature. Age Ageing 44: 196-204.
- Teslyar P, Stock VM, Wilk CM, Camsari U, Ehrenreich MJ, et al. (2013) Prophylaxis with antipsychotic medication reduces the risk of post-operative delirium in elderly patients: a meta-analysis. Psychosomatics 54: 124-131.
- Fok MC, Sepehry AA, Frisch L, Sztramko R, Borger van der Burg BL, et al. (2015) Do antipsychotics prevent postoperative delirium? A systematic review and meta-analysis. Int J Geriatr Psychiatry 30: 333-344.
- Liptzin B, Laki A, Garb JL, Fingeroth R, Krushell R (2005) Donepezil in the prevention and treatment of post-surgical delirium. Am J Geriatr Psychiatry 13: 1100-1106.
- Sampson EL, Raven PR, Ndhlovu PN, Vallance A, Garlick N, et al. (2007) A randomized, double-blind, placebo-controlled trial of donepezil hydrochloride (Aricept) for reducing the incidence of postoperative delirium after elective total hip replacement. Int J Geriatr Psychiatry 22: 343-349.
- Gamberini M, Bolliger D, LuratiBuse GA, Burkhart CS, Grapow M, et al. (2009) Rivastigmine for the prevention of postoperative delirium in elderly patients undergoing elective cardiac surgery--a randomized controlled trial. Crit Care Med 37: 1762-1768.
- Marcantonio ER, Palihnich K, Appleton P, Davis RB (2011) Pilot randomized trial of donepezil hydrochloride for delirium after hip fracture. J Am GeriatrSoc 59 Suppl 2: S282-288.
- Zaslavsky A, Haile M, Kline R, Iospa A, Frempong-Boadu A, et al. (2012) Rivastigmine in the treatment of postoperative delirium: a pilot clinical trial. Int J Geriatr Psychiatry 27: 986-988.
- Chakraborti D, Tampi DJ, Tampi RR (2015) Melatonin and melatonin agonist for delirium in the elderly patients. Am J Alzheimers Dis Other Demen 30: 119-129.
- Hempenius L, van Leeuwen BL, van Asselt DZ, Hoekstra HJ, Wiggers T, et al. (2011) Structured analyses of interventions to prevent delirium. Int J Geriatr Psychiatry 26: 441-450.
- Cole MG, Fenton FR, Engelsmann F, Mansouri I (1991) Effectiveness of geriatric psychiatry consultation in an acute care hospital: a randomized clinical trial. J Am GeriatrSoc 39: 1183-1188.
- Cole MG, Primeau FJ, Bailey RF, Bonnycastle MJ, Masciarelli F, et al. (1994) Systematic intervention for elderly inpatients with delirium: a randomized trial. CMAJ 151: 965-970.
- Milisen K, Foreman MD, Abraham IL, De Geest S, Godderis J, et al. (2001) A nurse-led interdisciplinary intervention program for delirium in elderly hip-fracture patients. J Am GeriatrSoc 49: 523-532.
- Marcantonio ER, Flacker JM, Wright RJ, Resnick NM (2001) Reducing delirium after hip fracture: a randomized trial. J Am GeriatrSoc 49: 516-522.
- Cole MG, McCusker J, Bellavance F, Primeau FJ, Bailey RF, et al. (2002) Systematic detection and multidisciplinary care of delirium in older medical inpatients: a randomized trial. CMAJ 167: 753-759.
- Han CS, Kim YK (2004) A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 45: 297-301.
- Hu H, Deng W, Yang H (2004) A prospective random control study comparison of olanzapine and haloperidol in senile delirium. Chongging Medical Journal8: 1234-1237.
- Kalisvaart KJ, de Jonghe JF, Bogaards MJ, Vreeswijk R, Egberts TC, et al. (2005) Haloperidol prophylaxis for elderly hip-surgery patients at risk for delirium: a randomized placebo-controlled study. J Am GeriatrSoc 53: 1658-1666.
- Maneeton B, Maneeton N, Srisurapanont M, Chittawatanarat K (2013)Quetiapine versus haloperidol in the treatment of delirium: a double-blind, randomized, controlled trial. Drug Des DevelTher24:657-667.
- Lonergan E, Britton AM, Luxenberg J, Wyller T (2007) Antipsychotics for delirium. Cochrane Database Syst Rev 18:CD005594.
- Ozbolt LB, Paniagua MA, Kaiser RM (2008) Atypical antipsychotics for the treatment of delirious elders. J Am Med DirAssoc 9: 18-28.
- Overshott R, Vernon M, Morris J, Burns A (2010) Rivastigmine in the treatment of delirium in older people: a pilot study. Int Psychogeriatr 22:812-818.
- Overshott R, Karim S, Burns A (2008) Cholinesterase inhibitors for delirium. Cochrane Database SystRev : CD005317.
- Van Eijk MM, Roes KC, Honing ML, Kuiper MA, Karakus A, et al. Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-blind, placebo-controlled randomised trial. Lancet 376: 1829-1837.
- Lonergan E, Luxenberg J, Areosa SA (2009) Benzodiazepines for delirium. Cochrane Database Syst Rev 4:CD006379.
- Campbell N, Boustani MA, Ayub A, Fox GC, Munger SL et al. Pharmacological management if delirium in hospitalized adults – a systemic evidence review. J Gen Intern Med 24:848-853.
- Friedman JI, Soleimani L, McGonigle DP, Egol C, Silverstein JH (2014) Pharmacological treatments of non-substance-withdrawal delirium: a systematic review of prospective trials. Am J Psychiatry 171:151-159.
- Alan J. Gelenberg, Marlene PF, John CM, Jerrold FR, Michael ET, et al. (2010) Treatment of Patients with Delirium.American Psychiatric Association, USA.
- Mittal V, Kurup L, Williamson D, Muralee S, Tampi RR (2011) Risk of cerebrovascular adverse events and death in elderly demented patients when treated with antipsychotic medications: A Literature Review of Evidence. Am J Alzheimers Dis Other Demen26:10-28.

