Introduction
The
modernisation reforms of the National Health Service (NHS) are both extensive
and far-reaching. A quality improvement agenda is to drive the development of
the NHS using the framework of clinical governance. A major outcome of clinical
governance is the ‘changing [of] organisational culture in a systematic and
demonstrable way, moving away from a culture of ‘blame’ to one of learning’.[1]
Modernisation and clinical governance documents make repeated reference to the
need for involving staff in developing the organisation, embracing constructive
criticism and new ideas, breaking down barriers between professional groups,
learning from error, personal development of staff and lifelong learning.[1–3]
These cultural changes envisaged as central to the success of the reforms are
embodied in the management approach known as ‘the learning organisation’, defined by Pedler et al. as ‘an organisation which facilitates the learning
of all its members
and thus continually transforms itself .[4]
In fact, the Framework for Lifelong Learning for the NHS states
explicitly that ‘all NHS organisations need to be learning organisations’ and
that ‘there is now unparalleled support for all NHS organisations to develop
and sustain a learning and knowledge sharing culture’.[3]
The smallest organisational unit within NHS primary care is the general
practice. Yet it is in primary care where nine out of ten NHS patients are seen
and where the largest number of patients will experience the success or failure
of modernisation.[5] Thus, if the modernisation reforms are to be
successful, then it is general practices that have to become learning
organisations.
While there has been much exhortation to develop learning organisations
within the NHS, and much effort to produce the infrastructure to support a
learning culture, there has been little to facilitate NHS organisations in
understanding and developing their cultures.[
3]
This paper reports the development of a learning organisation
diagnostic tool for use in general practice and its application to practices
within the North Tees Primary Care Trust (PCT).
Method
Development
of the instrument
A 40-statement
questionnaire using a five-point Likert scale was developed for completion by
the practice-employed staff of general practices. The statements explored staff
perceptions of the extent to which their employing practice displayed eight
characteristics of learning organisations. There was a mixture of positive and
negative statements with five statements pertaining to each of the eight
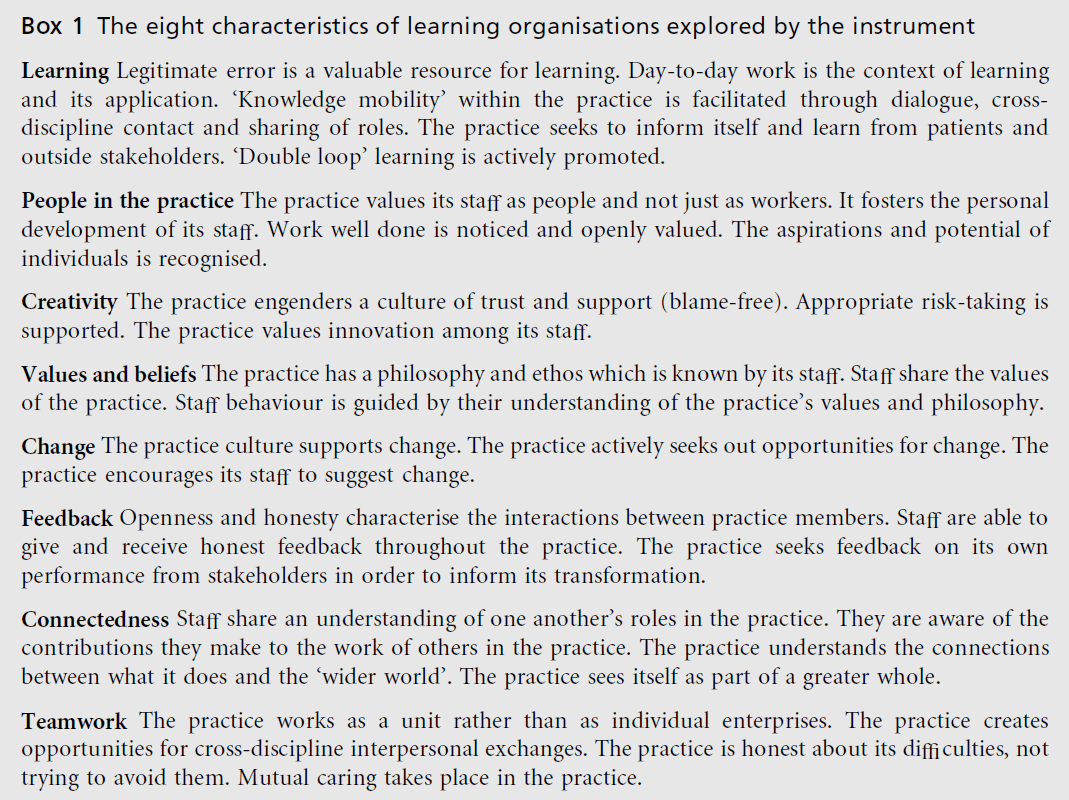
character-istics. The eight characteristics were chosen following an
examination of the management literature on the learning organisation,
particularly drawing on the work of Morgan and Kinston.[6,7] The eight
character-istics explored by the instrument are presented in Box 1.
Responses were indexed with
values from 1 to 5. The more positive the response to a statement (in terms of the
practice displaying that particular learning organisation feature), the higher
the value it was accorded. This method of scoring permitted a cumulative score
to be computed for each of the eight learning organisation characteristics
being measured. Each characteristic had five related statements in the
questionnaire; thus the score for each characteristic had a range of 5 to 25.
The reliability, construct validity and internal consistency of the
questionnaire were checked by a test–retest method involving 23 staff members
from five practices outside the North Tees PCT area (see Appendix 1).
Applying
the instrument
The subjects of
the study were general medical practices which are members of the North Tees
PCT. The North Tees PCT represents 24 practices serving a combined population
size of approximately 180 000. In the study only medical practices employ-ing
at least five staff members (administration and nursing staff) were included. The
reason for this arbitrary cut-off point was the confidential nature of the
inquiry and the risk of anonymity being compromised where only a small number
of staff is asked to participate. By involving larger practices, it was hoped that
staff would feel more willing to express their perceptions honestly. Of the 24
general practices in the North Tees PCT, 16 employed five or more staff and were
invited to participate.
All the employed staff (administrative and nur-sing) in each
participating practice were asked to complete a questionnaire each. They were
assured of anonymity and confidentiality and their responses were sealed in an
envelope prior to being returned to the investigator via their practice
manager. Practice managers and doctors were excluded from the study. While the
views and experience of these two groups are important, the study sought to
‘give voice’ to the experience of practice members who are unlikely to have
major influence in determining the practice culture. Responses to the
questionnaire were entered onto a database (EpiInfo). During data entry, if a
respondent did not respond to a question or their response was not clear, the
rest of their responses for that particular characteristic were excluded from
analysis as well. Analysis was carried out using the computer program to
produce, for each participating practice, a composite score for each of the
eight characteristics being measured. Comparisons were made between practices
and the mean scores for all the practices were calculated. Cumulative responses
to each of the 40 statements were also analysed.
Fifteen of the
16 eligible practices agreed to participate in the study. Of the 290
questionnaires distributed, 248 were returned (an overall response rate of
85.5%). In one practice the staff response rate was 51.7%, in one it was 70% and
in the remaining 13 practices the staff response rates were all greater than
80%. practices the
staff response rates were all greater than 80%.
Practice
size
Practice size,
as judged by number of staff, varied from five to 37 with a mean size of 19.3
staff.
Learning
organisation characteristics
The mean
practice scores and ranges for each of the eight characteristics are presented
in Table 1. The distribution of responses to the 40 statements of the
questionnaire is shown in Tables 2 and 3. Figures 1 to 8 illustrate the results
graphically.
Learning
Two practices
were in definite agreement (a score of 20 or greater) that this characteristic
was being expressed. The responses to the individual related statements identified ‘double loop’ learning and ‘knowledge mobility’ as the least developed areas
in practices.
People
in the practice
Two practices
expressed definite agreement and four definite disagreement (a score of less
than 15) that this characteristic was being expressed. Recognition for a job
well done scored lowest among the individual statements.
Creativity
Two practices expressed de? nite agreement that this characteristic was being expressed. In only one practice was there a less than neutral perception. Thirteen out of 240 staff claimed to be afraid of admitting their mistakes. On the other hand, 76 out of 240 staff felt willing to take risks in their job rather than toe the line.
Values
and beliefs
Table 1: Mean scores and ranges for the 15 participating practices
Table 2: Distribution of responses to statements pertaining to learning organisation
characteristics: learning, people in the practice, creativity and values and beliefs.
Table 3: Distribution of responses to statements pertaining to learning organisation
characteristics: change, feedback, connectedness and teamwork
Figure 1: Practice scores for the learning
organisation characteristic: learning
Figure 2: Practice scores for the learning
organisation characteristic: people in the practice.
Figure 3: Practice scores for the learning organisation
characteristic: creativity.
Figure 4: Practice scores for the learning
organisation characteristic: values and beliefs.
Figure 5: Practice scores for the learning
organisation characteristic: change.
Figure 6: Practice scores for the learning
organisation characteristic: feedback.
Figure 7: Practice scores for the learning
organisation characteristic: connectedness.
Figure 8: Practice scores for the learning
organisation characteristic: teamwork.
One practice
expressed a definite positive perception with regard to this particular
characteristic. Responses to individual statements were consistently near a
neutral perception.
Change
Two practices
expressed definite positive and two definite negative perceptions regarding
this charac-teristic. Out of 240 respondents, 105 disagreed that their practice
changed only when forced to by circumstances.
Feedback
Four practices
expressed a definite negative percep-tion with regard to feedback. Most
respondents (202 out of 244) perceived the practice to be bothered about what
others thought. Out of 244 respondents, 129 felt able to express an honest view
of the practice.
Connectedness
One practice
expressed a definite positive perception, but no practices had negative
perceptions with regard to this characteristic. Out of 238 respondents, 179
felt that their practice was aware of its dependence on external in• uences and
agencies.
Teamwork
Two practices
expressed definite positive and three definite negative perceptions with regard
to team-work. Out of 242 respondents, 193 described their practice as
‘friendly’. However, perceptions of con• ict avoidance were almost equally
split (91 out of 242 agreeing and 96 out of 242 disagreeing with the relevant
statement) and 134 out of 242 respondents agreed that their practice worked as
a team.
Learning
in North Tees PCT practices
While only two
practices agreed that this character-istic was being expressed, the mean practice
score of 17.39 suggests that perceptions tended to be positive. This ought to
encourage practices in their endea-vours. The responses to the individual
statements suggest that there is greater scope for development in the areas of
double loop learning and knowledge mobility.
Double loop learning refers to the practice of responding to error, not
merely by recognising the error and adjusting performance to prevent
recur-rence, but by using the opportunity of error to review or challenge the
assumptions that set the rule in the first place. The results suggest that
overall, staff barely perceive evidence of double loop learning in their
practices. The busy-ness of general practice may militate against formal
opportunities for double loop learning, yet this feature is regarded as key for
learning organisations and its practice is not so much an add-on, but an
approach which underpins the way people think in a learning organisation.[
5]
Knowledge mobility refers to the development of skills and knowledge
across the practice which allows not only a greater understanding (and
therefore support) of one another’s roles, but which distributes knowledge and
skills within the organisation thereby allowing staff to adopt different roles at
times of turbulence and change. Morgan refers to this as pluripotentiality
within the organisation.[5] A basic prerequisite for knowledge
mobility is the opportun-ity to find out about the roles of other staff members
and the results suggest that the staff questioned have limited opportunity for
this. If knowledge mobility is to develop, practices will need to find creative
ways of enhancing mutual understanding and support of roles.
Discussion
This
questionnaire-based survey sought to measure the extent to which primary care
general medical practices in the North Tees PCT expressed the characteristics
of learning organisations. The excel-lent response rates by practices (93.8% of
eligible practices) and their staff (85.5% of staff in participat-ing practices)
suggest that there is a strong desire among practices to understand themselves
as organ-isations and for their staff to feed back to their managers their
perceptions of their own experiences. In the present climate of change and
quality improvement in the NHS, this openness is to be welcomed and should
prompt PCTs to encourage and support primary care practices in examining and
developing their organisational culture.
People in
North Tees PCT practices
Overall, staff
did not feel valued and supported by their employing practices. In particular,
staff per-ceived that they lacked recognition and appreciation for the work they
did well (only 97 out of 242 expressed a positive view of this). The responses
to all the statements related to this characteristic make it plain that
practices who wish to be learning organ-isations have some way to go as far as
the humanistic elements of that ideal are concerned.
Creativity
in North Tees PCT practices
This
characteristic was one of the better expressed among the North Tees practices.
However, when examining the distribution of the responses to the five
statements regarding creativity, there is an interesting paradox. On the one hand staff felt unafraid to admit mistakes, suggesting an open, blame-free culture. Yet, on the other hand, they expressed an inclination ‘to toe the line and not take risks’ (only 97 disagreed with the statement). This possibly indicates that staff are prepared to own up to error, even though they perceive their job as allowing little room for innovation.
Values and
beliefs in North Tees PCT practices
The responses to
the statements regarding values and beliefs appear fairly consistent. The
overall scoring was low when it is considered that 14 of the 15 participating
practices claimed to have a mission statement or similar written statement of
their goals. It must be questioned who was involved in the drawing up of these
statements and how practices use these statements to guide their operation.
Change in
North Tees PCT practices
Fairly uniform views
were expressed about this characteristic of the learning organisation. The
lowest scoring statement, concerning changing only when forced to do so by
circumstances is interesting in the present climate of reform in which most of
the change occurring in primary care practices is externally driven and the
response to this statement may be an expression of this.
Feedback
in North Tees PCT practices
This
characteristic scored least well across the PCT. The responses to the
individual statements suggest that staff perceive their practices as being
better at seeking and valuing feedback from outside the practice than from
inside it. This relative devaluing of staff opinion accords with the perceptions
expressed under the ‘people in the practice’ char-acteristic.
Connectedness
in North Tees PCT practices
Although this
characteristic scored highest among the participating practices, as with
feedback, staff perceived a greater sense of being linked into things outside
the practice than being linked into an interdependent network within the
organisation.
Teamwork
in North Tees PCT practices
The findings
bear out the truth that a group of people working together, however friendly,
does not auto-matically constitute a team. The responses to the individual
statements confirm this, where, although the working atmosphere in practices
was described as ‘friendly’ by 79.3% of respondents, only 55.4% agreed that
they worked as a team in their practice. Brushing over rather than resolving
conflict is one of the ways in which teams malfunction. The fact that only
39.7% disagreed with the statement: ‘if there is bad feeling between people, we
generally avoid the issue’, suggests that this is an area in which primary care
teams struggle.
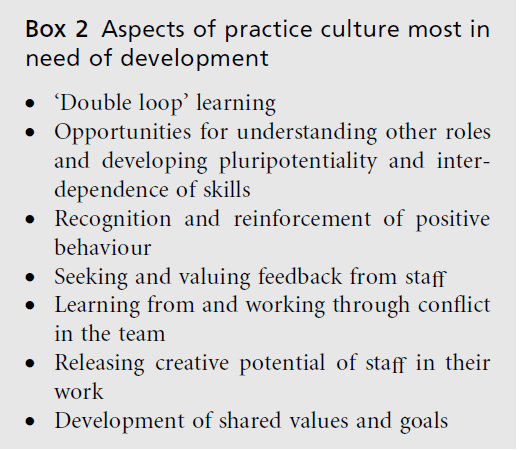
These results suggest that, overall, there is scope for significant
development of the culture within prac-tices in the PCT. This applies to all
eight character-istics that were measured, but it has been possible to identify
particular areas of underdevelopment and these are listed in
Box 2.
The use of a culture diagnostic tool such as that described can assist
practices in their development, both in setting objectives and in identifying
appro-priate resources to support their development. Used across a PCT, the
tool can help identify priority areas for organisational development support.
These find-ings have prompted the development of a practice toolkit to assist
practices who wish to act on the findings of their ‘culture diagnosis’.
Acknowledgements
This study
formed part of a dissertation for the degree of Master of Medical Education
from the Centre for Medical Education, Dundee, Scotland. The author received
funding from the Postgraduate Institute for Medicine and Dentistry, University
of
Newcastle upon Tyne and the Research Practices scheme of the NHS Executive.
References
- Department of Health (1999) Clinical Governance:
quality in the new NHS. NHS Executive: London.
- Department of Health (2000) An Organisation with a
Memory. HMSO: London.
- Department of Health (2001) ‘Working Together,
Learning Together’: a framework for lifelong learning
for the NHS. Department of Health Publications:
London.
- Pedler M, Burgoyne J and Boydell T (1991) The
Learning Company: a strategy for sustainable development.
McGraw-Hill: London.
- Department of Health (2001) Primary Care, General
Practice and the NHS Plan. Department of Health:
London.
- Morgan G (1998) Images of Organisation. Berrett-
Koehler Publishers Inc: San Francisco.
- Kinston W (1994) Strengthening the Management
Culture: phasing the transformation of organisations.
The Sigma Centre: London.
- Altman DG (1990) Practical Statistics for Medical
Research. Chapman and Hall/CRC Statistics and
Mathematics: London.
- Landis JR and Koch GG (1977) The measurement of
observer agreement for categorical data. Biometrics 33:
159–74.
- Mintzberg H (1979) The Structuring of Organizations.
Prentice Hall: Englewood Cli¡s, NJ.
Appendix 1
Reliability
testing
The stability of
the questionnaire was examined using a test–retest method.
Five practices outside the North Tees area (the area to be tested with
the final questionnaire) were contacted and asked to nominate a sample of their
employed staff to participate in the pilot study. Contact was made through the
practice manager of each practice and the method of staff selection was left to
them. In total, 29 practice members were recruited. Each was sent a copy of the
questionnaire to complete and return. Between 10 and 12 weeks later, each
participant completed the same ques-tionnaire a second time.
Individuals’ responses to each question were categorised as agreement
(includes ‘strongly agree’ and ‘agree’ responses), neutral (‘neither agree nor
disagree’) and disagreement (includes ‘disagree’ and ‘strongly disagree’
responses). When comparing paired responses from each individual, the extent to
which responses remained in the same category was measured using the
measurement of agreement known as kappa (K).[8] A value of K = 1 will occur when
there is perfect agreement of scores. A value of K suggests that the
agreement between pairs of responses is no better than chance. Intermediate
values of K were
interpreted according to Landis and Koch as shown in Table 4.[9]
Of the 29 participants, 23 completed a second questionnaire within the
time scale and these were analysed by the method above. The results of the
test– retest reliability after 10 to 12 weeks are displayed in Table 5.
The reliability of the questionnaire may be considered acceptable for
the following reasons:
the period between the
questionnaires (10 to 12 weeks) was long, given that test–retest studies were
usually carried out within intervals of four weeks or less
in the analysis of the final
questionnaire, indi-vidual scores were added in groups of five (thus diluting
the effect of less reliable questions)
Table 4: Interpretation of kappa values
Table 5: Test± retest reliability scores for
the 40 questions in the questionnaire.
the three least reliable
questions fell into different groups of questions, thus distributing them among
more reliable questions.
Internal
consistency
Although there
were five statements testing each of the eight learning practice
characteristics, the five statements were not necessarily testing the same
aspect of the characteristic. For example, the statements: ‘in this practice,
staff from different disciplines meet up regularly to discuss their work in the
practice’ and ‘people show little concern for one another in this practice’,
both test for evidence of teamwork in a practice, but are not measuring the
same concept of teamwork. In order to test for internal consistency, one pair
of statements that explored the same concept was selected from each of the
eight characteristic groups. The responses within each pairing were compared
and the extent of their agreement was measured using K , as had been used for the
test–retest reliability of the questionnaire. The pairs of statements selected
from each of the eight characters along
with the k value
for each pairing are shown in Table 6. For this estimate of internal
consistence the first questionnaire by staff in the pilot practices was used (n = 23). The results suggest a moderate to good degree of consistency within each
characteristic group.
Validity
testing
The way in which
the items were derived was described earlier in this section. The statements
were produced to link with the specific learning practice characteristics
derived from the work of Morgan, Mintzberg and Kinston.[6,7,10] The
face validity of the questionnaire is related to the relev-ance of each
statement to the descriptors derived for each learning practice characteristic.
Construct
validity
Construct
validity was tested during the pilot study by comparing the scores from two
practices known to be very different. One had a reputation for teamwork and
high-quality achievement and the other was going through a very di¤cult period
of low morale and organisational di¤culties. The scores comparing these two
practices are given in Table 7. As the results show, the ‘struggling’ practice
scores are appreciably lower (by 41.2% on average) than those of the highachieving
practice. This suggests that the question-naire is capable of detecting significant differences between practices.
Table 6: Internal consistency scores for the questionnaire, using , a statistical measure of
agreement.
Table 7: Comparison of scores of two contrasting practices.
















