Introduction
Every day 2.8
million prescription items on 1.3 million prescriptions are dispensed in
primary care. Seventy percent of these are ‘repeat prescriptions’, which are
repeated long-term prescriptions where the doctor does not necessarily review
the patient. Recent years have seen concerted efforts to improve the
quality of medicines management. (‘Medicines management is a system of
processes and behaviours that determines how medicines are used by patients and
by the NHS.’[1]) The NHS Plan promised changes that would improve access
to medicines and convenience in obtaining repeat
prescriptions for patients.[2] More recently, changes in NHS contracts
for general practice and community pharmacists have increased the emphasis on good
medicines management. Finally, the concept of information as therapy and the
development of NHS information prescriptions offer the opportunity for
better patient access to information about medi-cines. Taken together, these
changes have considerable potential to improve healthcare quality. But looked
at from a patient’s perspective how does the quality of the service measure up
in 2007?
Problems
with repeat medicines
The lack of
research on the problems that patients experience in relation to repeat
prescriptions is note-worthy. However, in 2002 the local teams of clinicians
and managers participating in the national Medicines Management Services
Collaborative (MMSC) ident-ified the following areas for improvement based on
analysis of their own practices and patients:[1]
prescription review
medication monitoring
improvement of general practitioner
(GP) com-puter and repeat prescribing systems
better prescription collection and
delivery services
development of concordance between
patients and healthcare professionals.
Patients also
experience more basic practical prob-lems; these are summarised in Box 1, with
some examples in patients’ own words in Box 2.

The prevalence
of these problems is difficult to estab-lish. Some practitioners argue
that the low level of complaints from their patients about these issues must
mean that they are not perceived as a real problem by patients. However,
patients may have low expectations of the system based on their previous
experience and assume that is just ‘how things are’. The ‘cost’ in terms of time and
inconvenience to patients is not always recognised or thought about as a cost
by clinicians.


One study found that there was misalignment in repeat intervals for
prescriptions of one in five older people.[3] Unintentional changes to
medicines follow-ing hospital discharge for a substantial proportion of
patients have been reported in several studies.[4] There is widespread
acknowledgement that patients might not be taking the medicines the clinician
thinks they are taking. In one area a nurse has been seeing patients identified
as being at risk of avoidable hospital ad-missions during 2007. When she talked
with patients in their own homes she compared the medicines and doses they were
actually taking with what the practice records showed they should be taking
(often eight, nine or ten medicines). There was not a single case where the two
lists were the same.
Patients’ understanding of their condition and the medicines used to
treat it may not be as complete as clinicians sometimes think, exemplified by a
study in diabetes which showed a lack of understanding about treatment in type
2 diabetes. One in five patients thought it was not very important to take
their medicines and was unaware of the complications of diabetes.[5]
For many patients the manufacturer’s leaf-let in the medicines pack may be the
only piece of information received. A recent review has shown that many
patients do not value these leaflets and want information more tailored to
their needs, including information about their condition as well as the
treat-ment.[6] The same review found consistent evidence that patients
want to know more about the side-effects of medicines, but many
side-effects are never discussed with the GP and only 1% are aware that
patients can report them on a yellow card.[7] Patients’ wishes to know
more about their condition and treatment are well illustrated in the findings
of the 2006 national survey of people with diabetes.[8] Almost a
quarter said they had not received sufficient information at the time
their diabetes was diagnosed. When a medicine is prescribed for the first
time patients need explanation, informa-tion, and the opportunity for
discussion. However, many GPs and nurses find it difficult to allocate
suf-ficient time for this in routine consultations. A recent randomised
controlled trial found that proactive com-munity pharmacist follow-up by
telephone with patient-centred advice increased adherence and reduced
medi-cine-related problems.[9] The simple questions used by the
pharmacist began with ‘How are you getting on with your medicines?’ before
asking more specifically about any problems with the new medicine, how the
patient was taking it and whether they had any questions about it.
Changes in NHS
policy and their effects
In 2000 The NHS
Plan made a series of commitments relating to repeat medicines (see Table 1).
Progress is more advanced in some areas than others, and some
interdependencies have emerged. The Electronic Prescriptions Service (EPS), for
example, has the potential to enable fuller implementation of other services
such as repeat dispensing. Currently most practices and pharmacies have to use
a cumber-some system of hard-copy prescriptions and records for repeat
dispensing. It is therefore perhaps not surprising that in 2006 only 0.7% of
prescription items in England were dispensed through repeat dispensing.
The Department of Health is introducing infor-mation prescriptions,[10]
and a set of pilots will be evaluated before a future service is specified. One
pilot specifically deals with information about medicines for children across
hospital and primary care. The government’s recently announced NHS Choices
website will offer, among other things, ‘Access to a vast library of
approved medical literature, previously only avail-able to clinicians, to
enable a deeper understanding of conditions & treatment options’.[11]
Primary
care contractual changes
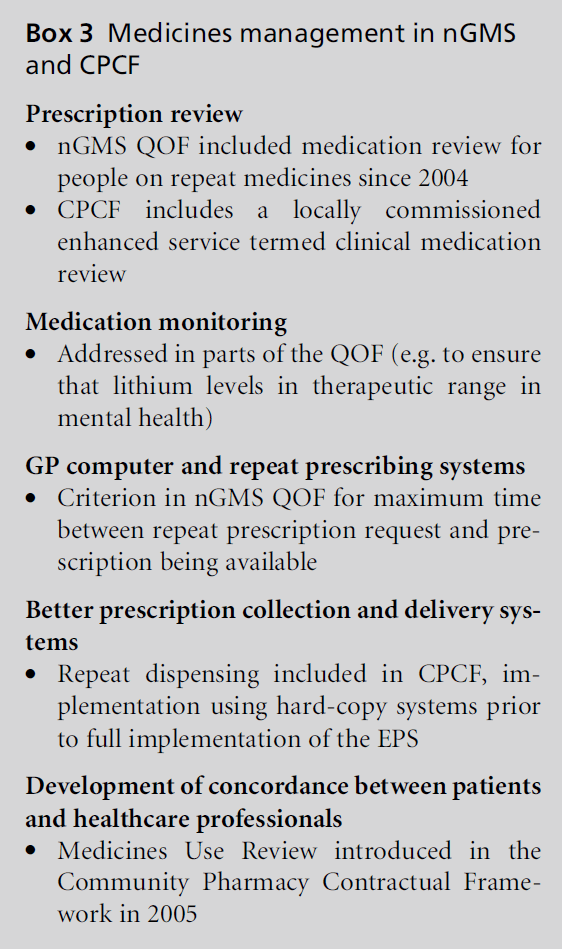
Both the revised
‘new General Medical Services’ (nGMS) contract and its Quality and Outcomes
Framework (QOF) in 2004 and the new Community Pharmacy Contractual Framework
(CPCF) in 2005 included several requirements and incentives relating to
medi-cines management (see Box 3).

Table 1: Commitments made in The NHS Plan and progress by 2007
‘Transfer of prescription data between GPs, pharmacies
and the Prescription Pricing Authority will be carried out electronically,
using the NHSNet, in the large majority of cases by 2008, or even earlier.’
National roll-out began in 2005. By March 2007 the
Electronic Prescriptions Service (EPS)a using Release 1 systems was
responsible for ‘over 8% of daily prescription messages’ and ‘1669 practices
were actively operating EPS’. Later in 2007 ‘initial implementer’ primary care
trusts (PCTs) will use Release 2 systems prior to full roll-out in 2008. Thus
by the end of 2008 patients should be able to nominate a pharmacy where their
prescriptions will be sent electronically. Repeat dispensing will then become
more feasible to implement on a wider scale.
The introduction this year (2000) of ‘‘Patient Group
Directions’’, which enable nurses and other professionals to supply medicines
to patients according to protocols authorised by a doctor and a pharmacist.
Patient Group Directions (PGDs) are now widely used in
primary care, e.g. practices; walk-in centres; community pharmacies.
‘By 2004 a majority of nurses should be able to
prescribe'.
Independent prescribing by nurses and pharmacists is
now established with flexibility to prescribe any medicine from the British
National Formulary according to individual competence.
‘... a wider range of over-the-counter medicines
available.’
Several key medicines have been switched from
prescription-only medicines (POM) to P (pharmacy), mainly for self-limiting
acute problems (e.g. chloramphenicol eye drops).
‘By 2004 every primary care group or trust will have
schemes in place so that people get more help from pharmacists in using their
medicines.’
New pharmacy contract was introduced in 2005 with
repeat dispensing as an ‘essential’ and medicines use review (MUR) as an
‘advanced’ service.
‘By 2004 there will be repeat dispensing schemes
nationwide to make obtaining repeat prescriptions easier for patients with
chronic conditions.’
‘NHS Direct nurses will be in regular contact
to help patients manage their medicines and check that older people living
alone are all right.’
At the end of
2006 repeat dispensing schemes were operating in many PCTs but only involved
0.7% of prescription items.
NHS Direct ‘is
keen to develop ... these [interactive digital TV] and online services further’
to support people with long-term conditions.[12]
a EPS, formerly Electronic Transfer of
Prescriptions, ETP.
The GMS QOF
introduced the first standards for prescription ordering and collection, and
for medi-cation review:
The number of hours from requesting a
prescrip-tion to availability for collection by the patient is 72 hours or less
(excluding weekends and bank/local holidays)
a medication review is recorded in the
notes in the preceding 15 months for all patients being pre-scribed four or
more repeat medicines (excluding over-the-counter (OTC) and topical
medications): standard 80%.
More patients do
now have their medicines reviewed and the Medicines Management Services
Collaborative made this a key area of work from its inception, which pre-dated
the QOF by several years. There are different types of review, not all of
which involve the patient or carer. Ideally the patient or carer will be
involved in the review. This is not a requirement of the QOF, and practices are
likely to prioritise cases where face-to-face discussion is likely to be of
particular benefit (for example multiple medical conditions and medicines,
patients frequently admitted to hospital, and those in residential or nursing
home settings). Medicines use review (MUR) by
community pharmacists is intended to focus on practical aspects of medicines
use, provide education to increase patients’ understanding of their medicines,
and to act as a filter for identifying patients who might need a clinical medication
review from the GP or practice pharmacist. However, evidence so far suggests
that MUR is not yet sufficiently integrated into primary care in a number
of ways.[13] GPs and primary care nurses can refer patients to a local
com-munity pharmacist for a MUR where, for example, a new medicine has been
started and the clinician perceives a need for further education and
informa-tion, or a patient is taking several medicines and they seem to be
having problems in managing them.
Practice-driven
changes
Other changes have been introduced by local
prac-titioners to meet patients’ needs. When compared with the situation in
2000:
prescription ordering using email and
fax has been introduced by some practices
prescription collection arrangements
between phar-macies and surgeries are much more widespread
prescription delivery is offered
by many phar-macies
information leaflets are now
offered by many sur-geries using the practice computer system.
There are no
figures on the extent of changes in prescription-ordering methods in practices.
Some practices are wary of introducing email or faxed requests, for safety
reasons. Anecdotally, a high proportion of repeat prescriptions are now dealt
with within existing informal collection and delivery arrangements. This should
make the process of nominating a preferred pharmacy for the EPS straightforward
for many patients. Although there are professional standards for
pre-scription-collection services, these do not include a minimum time in which
the collected prescription will be dispensed.[14] Prescription
delivery is offered by many community pharmacy services in response to
patient need, and its costs are met by pharmacies, with no contribution from
the NHS. Unsurprisingly not all pharmacies offer the service and since it
is not an NHS service there are no nationally agreed criteria to define who
should be eligible to have their medicines delivered. Pharmacies tend to
operate informal criteria and offer the service to patients who are
housebound or who have mobility problems. There are no data on the extent of
usage of information leaflets by practices. A small study found variability
between practices and between individual clinicians within practices.[15]

Towards patient-centred standards for
medicines management
In Box 4 we set
out a list of possible standards for discussion and local adaptation.16
Achieving quality in medicines management is only possible through local
collaboration between general practice, community
pharmacy and
other settings where medicines are prescribed (e.g. walk-in centres) in primary
care. Input from patients is needed to identify local issues and discuss
possible solutions. Those practices that do not have a patient participation
group can find alternative ways of achieving this.
A set of possible survey
questions to assess areas where standards are met or not met is listed in Box
5.

Conclusions
Medicines
management in primary care has improved in many respects since the publication
of The NHS Plan in 2000. Primary care teams could adapt and use our proposed
patient-centred standards, audit current performance and work with patients
towards im-provement in the areas identified.
Acknowledgement
We would like to thank Julia Bundock,
specialist primary care nurse, for her comments on the draft article
References
- National Prescribing Centre. Medicines management
services – why are they so important? MeReC Bulletin
2002;12(6). www.npc.co.uk/MeReC_Bulletins/2001
Volumes/pdfs/vol12no6.pdf (accessed 4 May 2007).
- Department of Health. The NHS Plan. London: Department
of Health, 2000.
- Hartzig V, Langley CA, Marriott JF and Wilson KA.
Polypharmacy and asynchronous prescribing in elderly
patients within primary care. International Journal of
Pharmacy Practice 2001;9(suppl):R77.
- Duffin J, Norwood J and Blenkinsopp A. An investigation
into medication changes initiated in general
practice after patients are discharged from hospital.
Pharmacy Journal 1998;261:R32.
- Assocation of British Pharmaceutical Industry, Diabetes
UK, Ask About Medicines. The Diabetes Information
Jigsaw. www.abpi.org.uk/publications/pdfs/diabetes_
jigsaw.pdf (accessed 4 May 2007).
- Raynor DK, Blenkinsopp A, Knapp P et al. A systematic
review of quantitative and qualitative research on the
role and effectiveness of written information available to
patients about individual medicines. Health Technology
Assessment 2007;11(5).
- Medicines and Healthcare Products Regulatory Agency.
Risks and Benefits of Medicines and Medical Devices –
Perceptions, Communication and Regulation. 2006. www.
mhra.gov.uk/home/idcplg?IdcService=SS_GET_PAGE&
useSecondary=true&SSDocName=CON2025474
- Healthcare Commission. Diabetes: the views of people
with diabetes. London: Healthcare Commission, 2007.
- Clifford S, Barber N, Elliott RA, Hartley E and Horne R.
Patient centred advice is effective in improving adherence
to medicines. Pharmacy World and Science 2006;
28:165–70.
- Department of Health. Our Health, our Care, our Say: a
new direction for community services. London: Department
of Health, 2006.
- Department of Health. Hewitt unveils Patient Choice for
all. London: Department of Health, 2007. www.gnn.
gov.uk/environment/fullDetail.asp?ReleaseID=277419 &NewsAreaID=2&NavigatedFromDepartment=False
(accessed 4 May 2007).
- Department of Health. Supporting People with Long
Term Conditions to Self Care. London: Department of
Health, 2006.
- Blenkinsopp A, Celino G, Bond C and Inch J. Medicines
use reviews: the first year of a new community pharmacy
service. Pharmacy Journal 2007;278:218–23.
- Royal Pharmaceutical Society of Great Britain. Code
of Ethics and Standards. 2006. www.rpsgb.org.uk/pdfs/
coe060524.pdf (accessed 4 May 2007).
- Blenkinsopp A and Dost A. Support for Self Care in
General Practice and Urgent Care Settings. London:
Department of Health, 2006.
- Department of Health. Management of Medicines: a
resource to support implementation of the wider aspects
of medicines management for the National Service Frameworks
for Diabetes, Renal Services and Long-Term Conditions.
London: Department of Health, 2003. www.dh.
gov.uk/en/Publicationsandstatistics/Publications/
PublicationsPolicyAndGuidance/DH_4088754
(accessed 4 May 2007).
- Bellingham C. Improving medicines management in
intermediate care. Pharmacy Journal 2004;273:349–50.
Conflict of Interest
None.

