Masafumi Seki1* and Yuji Watanabe1,2
1Division of Infectious Diseases and Infection Control, Japan
2Laboratory for Clinical Microbiology, Tohoku Medical and Pharmaceutical University Hospital, Sendai City, Miyagi, Japan
Corresponding Author:
Masafumi Seki
Division of Infectious Diseases and Infection Control
Tohoku Medical and Pharmaceutical University Hospital, Japan
Tel: +81-22-983-1221
E-mail: seki@hosp.tohoku-mpu.ac.jp
Received date: August 28, 2017; Accepted date: September 12, 2017; Published date: September 19, 2017
Citation: Seki M, Watanabe Y (2017) Microbiological Improvement by Antimicrobial Stewardship Program and Infection Control in Japan. J Prev Infect Cntrol. Vol.3 No.2:9.
Keywords
Antimicrobial stewardship (AS); Infection control team (ICT); Drug-resistant pathogens; Pseudomonas aeruginosa.
Introduction
Antimicrobial stewardship (AS) has been defined as an activity that includes appropriate selection, dosing, route and duration of antimicrobial therapy [1,2].
The benefits of AS are improved patient outcomes, reducedfrequency adverse events, improved rates of antibiotic susceptibility to targeted antibiotics and optimization of resource utilization across the continuum of care. The Infectious Diseases Society of America (IDSA), the Society for Healthcare Epidemiology of America (SHEA) and the Pediatric Infectious Diseases Society (PIDS) have strongly suggested that AS program (ASP) are best led by infectious disease physicians with additional stewardship training [1,2].
Recently, in addition to Infection Control Teams (ICT), interdisciplinary AS teams (AST), comprising infectious disease physicians, pharmacists, nurses and microbiological technicians, have begun to be organized at university and/or tertiary hospitals in Japan and the efficacy of the resulting interventions in preventing inappropriate antibiotic use have been reported for Japanese AST [3-5]. In our hospital, a 600-bed tertiary-care university hospital in the city of Sendai in Japan, all adult patients who were (a) hospitalized at our facility from 2010 to 2017, (b) received antibiotic therapy, and (c) for whom an intervention was recommended by our ICT/AST, were eligible for enrolment in this analysis.
The roles of the ICT/AST included a review of antimicrobial orders with respect to the usage, dose, isolated pathogens and sites of infection for all inpatients receiving parenteral antibiotics, and consultation with physicians before the prescription of antibiotics. Cases receiving carbapenems, antipseudomonad penicillins, fluoroquinolones, 4th-generation cefems and anti-Methicillin resistant Staphylococcus aureus (MRSA) agents were specifically reviewed. When an inappropriate use of antibiotics was found, ICT/AST members made immediate contact with the prescriber over the telephone, via report papers, and/or via electronic messaging on the computer order system. Usually, total 50-100 patients were monitored and finally a half of them were intervened in each month by our ICT/AST.
As the results, antibiotic susceptibility of Pseudomonas aeruginosa were significantly improved, and multiple-drug resistant P. aeruginosa (MDRP) were become none from 2010 to 2017 (Figure 1). Especially, resistant P. aeruginosa for carbapenems including imipenem/cilastatin and meropenem, aztreonam and fluoroquinolones including levofloxacin and ciprofloxacin were significantly decreased.
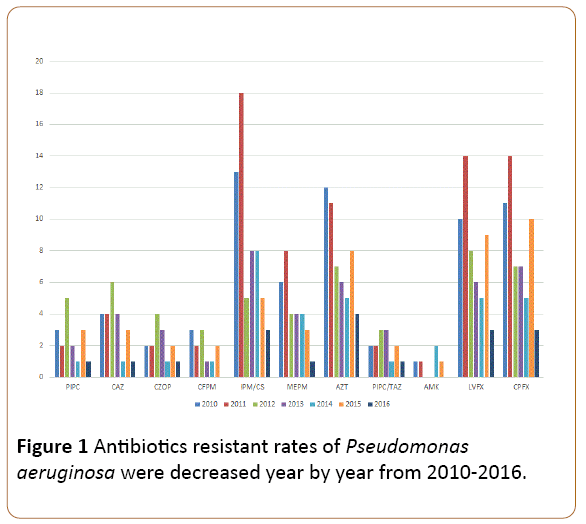
Figure 1: Antibiotics resistant rates of Pseudomonas aeruginosa were decreased year by year from 2010-2016.
As we have previously reported, the occurrences of drugresistant strains including MDRP and related infectious diseases, such as pneumonia and blood stream infection (BSI), were big issues in Japan [6,7].
ICT/AST intervention for pneumonia has been reported to yield a significant decrease (from a median of 10 to 7 days) in the duration of antibiotic therapy and also result in more frequently narrowing of antibiotic spectrum or modification on the basis of susceptibility results [8]. Maeda et al. [4] showed that an AST intervention approach decreases the use of inappropriate therapy and may improve clinical outcomes in BSI patients and previous other studies have reported that clinical intervention by infectious disease specialists also reduces mortality, length of stay (LOS) and medical costs. These results indicate that ICT/AST interventions can decrease inappropriate therapy and also potentially improve clinical and economic outcomes in severe infectious disease, including pneumonia and BSI by P aeruginosa [9,10].
Conclusion
Therefore, a multidisciplinary ICT/AST, including microbiologists, is very important for successful interventions and improving drug susceptibility of the pathogenic bacteria [4,11]. Recommendations regarding appropriate therapies require a broad knowledge of infectious diseases. Interdisciplinary teams that are able to facilitate discussion among specialists from various relevant occupational fields may be lead to successful implementation by ICT/AST.
Acknowledgement
This work was supported by Japanese Society for the Promotion of Science Grant-in-Aid for Scientific Research 17K09623 (to M.S.).
References
- Dellit TH, Owens R., McGowan JE Jr, Gerding DN, Weinstein RA, et al. (2007) Infectious diseases society of America and the society for healthcare epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis 44: 59-77.
- Barlam TF, Cosgrove S, Abbo LM, MacDougall C, Schuetz AN, et al. (2016) Implementing an antibiotic stewardship program: guidelines by the infectious diseases society of America and the society for healthcare epidemiology of America. Clin Infect Dis 62: e51-e77
- Niwa T, Shinoda.Y, Suzuki A, Ohmori T, Yasuda M, et al. (2012) Outcome measurement of extensive implementation of antimicrobial stewardship in patients receiving intravenous antibiotics in a Japanese university hospital. Int J Clin Pract 66: 999-1008.
- Maeda M, Takuma T, Seki H, Ugajin K, Naito Y, et al. (2016) Effect of interventions by an antimicrobial stewardship team on clinical course and economic outcome in patients with bloodstream infection. J Infect Chemother 22: 90-95.
- Tagashira Y, Horiuchi M, Tokuda Y, Heist BS, Higuchi M (2016) Antimicrobial stewardship for carbapenem use at a Japanese tertiary care center: An interrupted time series analysis on the impact of infectious disease consultation, prospective audit and feedback. Am J Infect Control 44: 708-710.
- Miyawaki K, McQuillen D, Nahass R, Martinelli L, Rubin M, et al. (2014) Infectious diseases specialty intervention is associated with decreased mortality and lower healthcare costs. Clin Infect Dis 58: 22-28
- Isobe M, Uejima E, Seki M, Yamagishi Y, Miyawaki K, et al. (2012) Methicillin-resistant Staphylococcus aureus bacteremia at a university hospital in Japan. J Infect Chemother 18: 841-847.
- Avdic E, Cushinotto L, Hughes AH, Hansen AR, Efird LE, et al. ( 2012) Impact of an antimicrobial stewardship intervention on shortening the duration of therapy for community-acquired pneumonia. Clin Infect Dis 54: 1581-1587.
- Schmitt S, McQuillen D, Nahass R, Martinelli L, Rubin M, et al. (2014) Infectious diseases specialty intervention is associated with decreased mortality and lower healthcare costs. Clin Infect Dis 58: 22-28.
- Huang AM, Newton D, Kunapuli A, Gandhi TN, Washer LL, et al. (2013) Impact of rapid organism identification via matrix-assisted laser desorption/ionization time-of-flight combined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia. Clin Infect Dis 57: 1237-1245.
- Briceland LL, Nightingale C, Quintiliani R, Cooper BW, Smith KS (1988) Antibiotic streamlining from combination therapy to monotherapy utilizing an interdisciplinary approach. Arch Intern Med 148: 2019-2022.

