Keywords
Antioxidants; Ascorbic Acid; Cystic Fibrosis; Cytochrome P-450 Enzyme System; Mast Cells; Methionine
Abbreviations
CFTR: gene encoding the cystic fibrosis conductance regulator protein; CFTR: protein product of the CFTR gene; CTRC: gene encoding for chymotrypsinogen C; CYP: cytochrome P450; CYP1A2: polycyclic aromatic hydrocarboninducible form of cytochrome P450; CYP2A6: coumarin and nicotine metabolizing form of cytochrome P450; CYP2E1: ethanol-inducible form of cytochrome P450; ERCP: endoscopic retrograde cholangiopancreatography; PRSS1: gene encoding cationic trypsinogen; SPINK1: gene encoding the serine protease inhibitor Kazal type 1
INTRODUCTION
It is a sobering thought that more than 200 years after the post-mortem identification of chronic pancreatitis [1], removal of the whole gland is an accepted form of treatment when pain is unrelenting [2]. Micronutrient therapy, formulated from observations at Manchester over a 15-year period 1983-1998 [3, 4, 5, 6, 7, 8, 9], is poised to change this bleak outlook now that a definitive study from Delhi has been published [10], after trials in Santander [11], Belfast [12], Brno [13] and Naples [14]. This paper sets out the background to the treatment and expands on the implications of its success, in the light of groundbreaking advances in genetic information.
The Disease
Natural History
Chronic pancreatitis is a crippling disease. It maims by increasingly agonizing pain with superimposed attacks of pancreatitis on a variable timescale [15]. Each bout causes patchy loss of acini until all are destroyed and replaced by fibrous tissue, when pain tends to regress. By then, however, patients have often become addicted to narcotic analgesics, lost their jobs, homes and families. Duct strictures and calculi may develop and are readily diagnosed, in contrast to small-duct disease [4]. Pancreatic cancer looms [16]. Most patients fall into alcoholic and idiopathic groups, the latter with its tropical variant. Among the others hereditary pancreatitis, autoimmune disease, hyperlipidaemia or hyperparathyroidism may be detected. Alcohol is overrated, in that about 18 years elapse before the first symptom in men who drink more than 150 grams of ethanol daily. Any theory on pathogenesis should reconcile the paradox that some fall prey after just 20 grams per day, and other idiosyncrasies; accommodate genetic links; and rationalize demography [15].
Pathopysiology: Initiating Mechanisms
Today acute pancreatitis which is characterized by a histological restitutio in integrum after full clinical recovery, recurrent acute pancreatitis, and the irreversible inflammatory fibrosis of chronic pancreatitis are regarded more as a disease continuum than utterly different entities [15, 16]. This view is supported by the clinical and biochemical identity of a pancreatitis attack, overlapping extrinsic [3, 4] and genetic [16] aetiologies, and the observation that experimental protocols which induce acute pancreatitis can be manipulated to cause fibrosis [15, 17].
It has long been known that experimental pancreatitis begins in the acinar cell with a functional blockade to apical exocytosis of enzymes [18], for which anomaly the term ‘pancreastasis’ seems apt [17]. Subsequent events can be interpreted as a strategy to prevent the build-up of food digestive enzymes, when the cell perceives a threat to its secretory integrity [17].
i) Newly synthesized enzyme is quickly shunted out via the basolateral membrane into the portal venous outflow and lymphatics [19], which could account for the blood enzyme rise in a clinical attack of pancreatitis.
ii) Stored enzyme is removed by centripetal dissolution of zymogen granules [20] and by their redirection to the basolateral membrane [21].
iii) A controlled activation of trypsinogen in the secretory pathway by co-localization with lysosomal enzymes, which yields <2% of potential trypsin load [22] and facilitates protease degradation [20]; and
iv) apoptosis of cells that contain trypsin or mutated cationic trypsinogen [23] could be part of the same strategy.
Alternatively, as is now generally believed, the colocalization phenomenon is pathological and signifies the start of pancreatic ‘autodigestion’ [16].
Whatever the true interpretation may be, time-course analysis shows that a burst of electron transfer reactions is tied in with the disease-initiating secretory blockade [17]. For example, in the experimental model of mild acute pancreatitis produced by excessive stimulation with caerulein, the spark from reactive oxygen species is seen by chemiluminescence within five minutes as also is a huge increase in stress activated protein kinase evoked thereby: amylase in the gland’s venous outflow increases by 10 minutes in line with the reversed secretory polarity [24]. Similarly in endoscopic retrograde cholangiopancreatography (ERCP)-induced acute pancreatitis, analysis of peripheral blood by electron spin resonance spectroscopy identifies the burst of reactive oxygen species by the end of the clinical procedure, followed by steep increases in amylase, lipase and trypsinogen [25].
The complex downstream interactions that result in pancreatic inflammation have been reviewed [26]. They involve reactive oxygen and nitrogen species, free radical oxidation products, chemokines and cytokines liberated by a variety of cells, including the injured acinar cell.
Chronic Pancreatitis: Casualty of Oxidative Detoxification
Manchester Model
This disease model has evolved over the years to accommodate new observations. The 1998 version [27] views the acinar cell as the site of steady erosion of methyl and thiol, essentially glutathione, moieties as a result of regular exposure to xenobiotics that induce cytochrome P450 (CYP) mono-oxygenases while yielding electrophilic intermediates: inadequate prior diets set the scene. Within this framework, each burst of unopposed electron transfer reactions jeopardizes apical exocytosis to trigger an attack. The secretory diversion drives pro-inflammatory oxidation products into the interstitium, such that mast cells degranulate: this leads to fat necrosis, activation of the ‘contact system’ of blood coagulation, nociceptive axon reflexes, and profibrotic interactions. Duct cells are caught up in a manner that unfortunately amplifies the disease. These problems are compounded when relatively stable substances generated via induced hepatic CYP find their way into the gland by bile reflux or the bloodstream [15, 17]. The template allows for methyl-thiol depletion due to protracted stress from reactive oxygen species alone, as in hereditary pancreatitis (see below). In regard to autoimmune disease, wherein lactoferrin is a suspected antigen [28], the ability of reactive oxygen species to derange the structure and hence immunogenicity of gammaglobulin is relevant.
CYP Induction; Toxic Electrophiles
The metabolism of xenobiotics in the liver is usually a two-stage process [29]. In phase-1, microsomal CYP utilize reactive oxygen species to reveal or insert a functional group such that the intermediate metabolite can move into the cytoplasm for phase-2 conjugation reactions with glucuronic acid, inorganic sulphur, acetyl groups or glutathione. In the process the substrate is usually detoxified, or de-activated in the case of a drug. Regular exposure to a xenobiotic results in an increase of the corresponding CYP isoform, as can be gauged by studying the disposal of drug probes: for example, theophylline clearance kinetics reflect activity of CYP1A that is induced by polycyclic aromatic and chlorinated hydrocarbons [29]. This protective mechanism of enzyme induction backfires, however, if a xenobiotic inadvertently undergoes bioactivation to a hazardous intermediate metabolite, for now cell viability is threatened both by the increased load of reactive oxygen species and by reactive xenobiotic species: the former is especially true for induction of CYP2E1 [30]. The concerted action of superoxide dismutase in two forms (manganese or copper-dependant), catalase, glutathione peroxidase, and pyridine nucleotides limits the lifespan of reactive oxygen species [31]. Glutathione, synthesized from the essential aminoacid methionine (Figure 1), is the main defence to reactive xenobiotic species but, whereas it is easily regenerated after reactions in removing oxygen free radicals, it is irretrievably lost in glutathione transferase-mediated conjugation with reactive xenobiotic metabolites [31, 32]. Clinicians are familiar with these principles in relation to paracetamol hepatotoxicity.
Figure 1. Methionine metabolism, adapted from [15]. Abbreviations
are listed alphabetically. ATP: adenosine triphosphate; B6: pyridoxyldependant
enzymes; B12: cyanocobalamin; CYP: cytochromes P450;
iSO4: inorganic sulphate; glu-6-PO4: glucose-6-phosphate; GSH:
glutathione; GSH-GST: the glutathione-glutathione transferase
couple; GSH.Px: selenoenzyme glutathione peroxidase; GSH.Rx:
riboflavin-dependant glutathione reductase that interlinks with
shuttles involving glucose-6-phosphate (glu-6-PO4) and nicotine
adenosine phosphate in oxidized (NADP) or reduced (NADPH)
form; GSSG: reversibly oxidized form of glutathione; GSSR:
irreversibly oxidized form of glutathione that is excreted from the
cell; MTA: methyl thioadenosine; Pi: activated phosphate; RXS:
reactive xenobiotic species; SAH: sulph-adenosylhomocysteine;
SAMe: sulph-adenosylmethionine.
High fat/protein diets, as are associated with chronic pancreatitis, facilitate CYP induction: constituents of cigarette smoke, which increase disease risk, are potent inducers and generate reactive intermediates [3]. The bulk of ethanol is processed oxidatively via the alcohol-acetaldehyde route; there is a non-oxidative route that yields free fatty acid ethyl esters; both have been implicated in pancreatic injury [33, 34]; and duct cells are active too [35] - but long-term ethanol does not produce chronic pancreatitis experimentally [36]. However, even a small dose induces CYP2E1, thus increasing the toxicity from other chemicals to which the animal is simultaneously exposed [37]. This becomes relevant with the identification of occupational volatile chemicals (diesel exhaust fumes and chlorinated solvents in particular) as an independent risk factor for chronic pancreatitis at Manchester [38], as also of the association with the disease of those chemicals alongside domestic paraffin at Soweto [33, 39] or domestic kerosene at Madras (Chenai) [40].
A large-scale pharmacokinetic investigation indicated CYP induction, especially CYP1A, in the majority of Manchester patients with chronic pancreatitis [41]. Proof of acinar involvement has come from immunolocalization studies, which also show a degree of induction in ductal elements [42, 43, 44]. Although induced pancreatic CYP contribute virtually nothing to overall xenobiotic removal [29, 43], their toxicological significance is evident from structural and biochemical analysis: cytoplasmic vacuolation and excess lipofuscin in acinar cells [4, 15, 17]; dilated endoplasmic reticulum and increased lysosomes in duct cells [4]; increased concentrations of free radical oxidation products in the gland [45], pancreatic juice [46] and duodenal aspirates [5, 47]; mobilization of endogenous antioxidant defences [48] such as lactoferrin by acinar cells [4, 28] and mucus by ducts [40].
The CYP-induced hepatocyte is under strain too, as revealed by microvesicular steatosis and excess lipofuscin in many non-alcoholic patients [15]: increased bilirubin in bile, with a striking surge during a relapse, reflects the activation of haem oxygenase and both represent antioxidant defences [15, 48]. Yet these aberrations are silent, while the acinar cell bears clinical witness to the xenobiotic assault. This is analogous to the far greater sensitivity of the pancreas to CYP-mediated injury from carbon tetrachloride [17, 27]. Also of note, a single injection of dibutyltin (which has many industrial applications [32]) produces within 60 days a good animal model of chronic pancreatitis after an initial phase of acute inflammation, with damage amplification by doses of ethanol that are otherwise harmless, indicating CYP2E1-mediated reactive xenobiotic metabolites [49]. Several factors help to rationalize these findings.
i) There is a dearth of glutathione transferases in acinar cells [32, 42, 50, 51] and virtually no coppersuperoxide dismutase [52] - whereas duct cells are better protected - while pancreatic levels of the other antioxidant enzymes fall in chronic pancreatitis [53].
ii) The pancreas has a much lower complement of glutathione than the liver [32].
iii) Its pool of cysteine for glutathione synthesis is small, and needed for protein folding [32].
iv) The inhalation route of xenobiotic entry [33, 38, 39, 40] ensures a direct arterial strike once the pulmonary circulation is traversed.
v) Although islets have a generous quota of glutathione transferases [42, 50, 51], they show such potent CYP induction in chronic pancreatitis [42, 43, 44] that reactive xenobiotic metabolites which escape into the gland’s portal circulation would amplify injury [27, 51].
vi) Above all, considering the huge turnover of protease grenades, is the vulnerability to toxic electrophiles of the signal transduction pathway towards apical exocytosis [15, 18, 54].
Disrupted Methyl and Thiol Metabolism
Toxic electrophiles can disrupt signal transduction in many ways [17, 27], and it may be that different mechanisms operate in different settings of acute pancreatitis. However, reviewed studies in young female mice with lethal disease due to a cholinedeficient DL-ethionine-supplemented diet offer useful insights [17, 55]: the relative safety of older females but vulnerability of oestrogen-treated males implicates a reactive oestrogen metabolite [17]. A burst of electron transfer reactions is detected by electron spin resonance spectroscopy at six hours, and apical secretion is paralysed by 24 hours with death by the fifth day. DL-ethionine injury is caused by a metabolic blockade high up in the methionine trans-sulphuration route, such that the supply of adenosine for synthesis of adenosine triphosphate, and of both methyl and thiol groups is compromised: denial of choline augments these problems (Figure 1). Of note, methyl and thiol (glutathione) moieties are essential for exocytosis [17, 27], as is folate which acts as a methyl donor [55]. Reports on paracetamol and carbon tetrachloride toxicity show that key enzymes in the transsulphuration pathway are vulnerable to reactive xenobiotic metabolites [15, 27]. Modification of the DL-ethionine regimen induces chronic pancreatitis-like lesions [17, 55].
Studies of human chronic pancreatitis indicate a similar pattern. Thus, at admission in an attack, neutrophils show low glutathione but increase in the oxidized disulphide form indicating electrophilic stress [56], while urine [56] and blood analysis [7] point to a metabolic block in the trans-sulphuration pathway, but now distal to cysteine (Figure 1) - leading to surges in cysteine and more proximate metabolites, but a fall in inorganic sulphur. By the third day subnormal methionine and a further decline in sulphur levels hint at poor pre-morbid intakes. These twin problems, of on-going oxidant-related hindrance in the transsulphuration pathway and methionine insufficiency, are reflected in findings on serum/plasma analysis in quiescent disease: increased free radical oxidation products [7, 8, 10, 33, 45, 57, 58] but subnormal methionine (unpublished), sulph-adenosylymethionine [7], cysteine and cysteinyl glycine [57], taurine [59], total thiols [58] and glutathione [33, 57]. Moreover, a study using radiolabelled L-methionine showed good uptake by the pancreas but then backdiffusion, coupled with reduced enzyme and label secretion into the duodenum [60]. In these conditions cysteine appears to be diverted along pathways that generate hydrogen sulphide [61], which is increased in exhaled air of patients with chronic pancreatitis [62] and has been linked experimentally to pancreatic pain [63].
Genetic Studies
The possibility of a genetic predisposition to chronic pancreatitis due to heightened oxidative metabolism or defective antioxidant/conjugation resources has been explored but without consistent evidence for either [34, 64, 65]. However, two reports on idiopathic disease suggest susceptibility to xenobiotic stress: increased frequency of functional glutathione transferase form GSTT1*A, which tends to yield reactive xenobiotic metabolites [26], but lowered glutathione and its redox ratio in erythrocytes [64]; increased frequency of the PON1-192Q allele of paraoxonase which compromises its xenobiotic detoxification capability [66].
Micronutrient Therapy
Clinical Trials
Several micronutrients have antioxidant potential [31]. However, a comparison of the habitual diets of patients with idiopathic chronic pancreatitis, an equally CYP1A-induced set of epilepsy controls on anticonvulsants, and healthy volunteers at Manchester identified the patients’ need of just three (methionine, vitamin C and selenium [67]), which together should buttress pancreatic methyl and thiol groups (Figure 1). Subnormal serum/plasma concentrations of these micronutrients have been reported [7, 8, 33, 58, 68, 69, 70, 71] but are also influenced by increased oxidation, utilization, tissue sequestration, and malabsorption. In the 1980s there was no tablet that would deliver these, and only these, three substances. By trial and error, using Selenium-ACE® (selenium with vitamins A, C and E; Wassen International Ltd., Leatherhead, United Kingdom) with or without methionine tablets (Evans Medical Ltd., Horsham, United Kingdom), we found that doses for symptom relief varied widely and that patients with recurrent acute pancreatitis benefited too: they displayed elevated levels of free radical oxidation products in duodenal aspirates and serum [5], although blood levels of micronutrients were generally normal [15, 70]. By 1985, observations in 23 patients showed that six Selenium-ACE® plus eight methionine tablets per day most often controlled symptoms [9]. That combination, but with beta-carotene in place of vitamin A, was selected for formal assessment. Table 1 summarizes results of trials to date, wherein every effort was made to eliminate bias [72].
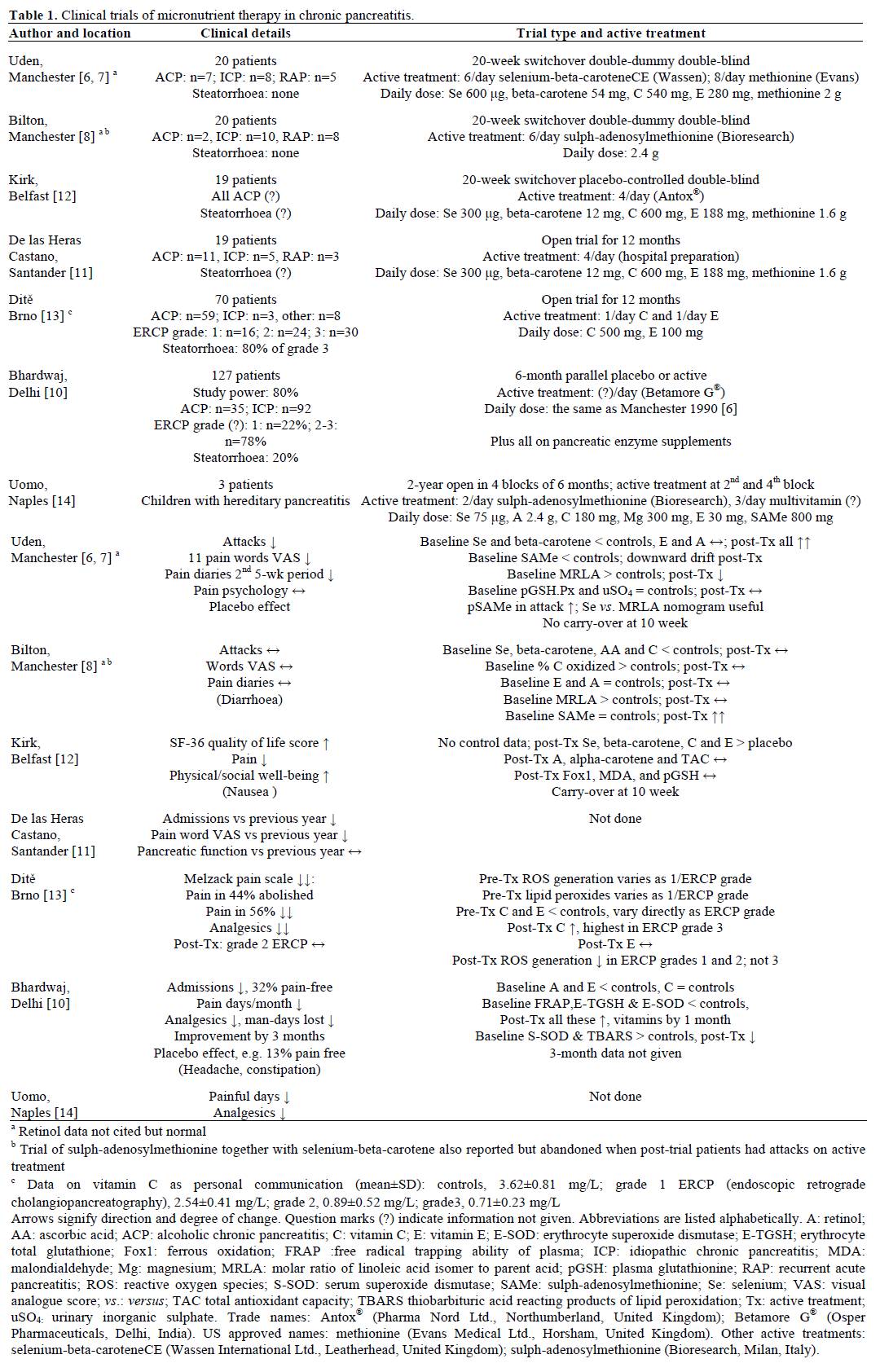
Some interesting points emerge.
i) Treatment curbs attacks and controls background pain in chronic pancreatitis pari passu with a fall in markers of electrophilic stress and restoration of erythrocyte glutathione. This holds true irrespective of aetiology or pancreatogram appearance.
ii) The Dehli study shows that blood antioxidant profiles improve within a month and pain is controlled by three months, in keeping with the Manchester and Belfast experience at 10 weeks.
iii) The Brno study suggests that the degree of electrophilic stress is highest in patients with the greatest amount of functional parenecyhma, that is with least abnormal pancreatograms.
iv) Measures of total antioxidant status do not help to monitor micronutrient therapy, as the Belfast study shows for a kit method which largely reflects albumin, glucose, uric acid and bilirubin [73]. Similar problems beset the ’free radical trapping ability of plasma’ assay as used at Delhi: ascorbic acid (the active form of vitamin C) normally contributes 20% to the reading, vitamin E 5%, beta-carotene very little and thiols none. The assay value in Delhi controls is much less than elsewhere [57, 74] although the endogenous component was normal (uric acid not reported) and plasma ‘total vitamin C’ as high as at Manchester, on average 12 mg/L [8]; further, the lower reading in patients improved on treatment although their baseline vitamin C level was normal. The first anomaly may be methodological [74]. The second strongly suggests low ascorbic acid in Delhi controls with a further fall in chronic pancreatitis, but masked in the total vitamin C assay - as has been noted previously [8, 33], including in a report from Madras which suggested ascorbate oxidation during cooking [75].
v) Studies of acute pancreatitis in cyclosporinetreated pancreatic allografts [76] suggested that sulphadenosylmethionine may be enough (Figure 1). It was not, whereas combined treatment attenuated damage in a cyclosporine-hyperstimulation model of pancreatic fibrosis [77].
vi) We did not think that vitamin C alone as in the Brno trial in alcoholic chronic pancreatitis could work (vitamin E was given too, but its levels did not improve). However, there are experimental precedents. Thus: a synthetic analogue of ascorbic acid improved survival in the virulent dietary model of acute pancreatitis [78], and was very helpful in the caerulein model [79]; ascorbic acid ameliorated damage from dibutyltin [80]; and it attenuated the secretory blockade caused by the potent oxidant tert-butylhydroxyperoxide [81]. Several properties of ascorbic acid rationalize the benefit: its excellent capacity to scavenge electrophiles [82, 83]; its action as ‘Michael donor’ in toxicity studies of acrolein [82], which is a derivative of acetaldehyde, as well as in reactions with genotoxic lipid peroxidation products [83]; and redox coupling between glutathione/glutathione disulphide and ascorbic/dehydroascobic acid (Figure 1) [84]. The last effect and the delayed onset of scurvy by treatment with glutathione-ester in ascorbate deficient guinea pigs [85] indicate metabolic substitution between ascorbic acid and glutathione. Since plasma vitamin C was very low in Brno controls (Table 1), the inference may be that methionine status was good, and that prescribed ascorbic acid in the chronic pancreatitis group protected trans-sulphuration enzymes from reactive chemical species.
The restoration of methyl and thiol groups needed for apical exocytosis in the acinar cell is the best explanation for the fall in attack frequency on micronutrient therapy. Lowered delivery of proinflammatory substances via basolateral pathways and increased micronutrient levels in tissues rationalize alleviation of background pain. Among the many factors implicated [86], these could be mollified by 10 weeks’ treatment: increased interstitial fluid pressure; the inflammation-immune response [26, 87]; mast cells [17, 25, 27, 88] with the pro-inflammatory [17, 25, 89], and painful [27, 90] consequences of their activation; and the hydrogen sulphide effect on nociceptive channels [61, 63].
Trials of other electrophile scavengers in alcoholic chronic pancreatitis include a Baghdad study which noted dramatic benefit from daily intra-rectal treatment with allopurinol or dimethyl sulphoxide in an attack [91], and an anecdotal report of benefit after intravenous chlorophyll-A [92]. By contrast, trials in quiescent chronic pancreatitis showed that neither allopurinol [93] nor curcumin [94] alleviated pain. We conclude that the first two interventions controlled neutrophil-derived reactive oxygen species during exacerbations [95] but the others failed to protect the trans-sulphuration pathway in stable disease. It seems that a grape seed extract with potent antioxidant qualities was able to do so, judging by another anecdotal report [96].
Follow-up: Need To Control Reductive Stress?
The long-term value of micronutrient therapy at Manchester and practicalities of delivery have been documented [9, 97]. Among the 10% of treatment failures there were two patients (chronic pancreatitis and polycystic kidneys; recurrent acute pancreatitis and arthritis on ‘sulindac’) in whom a choline supplement to provide more methyl groups (Figure 1) afforded rapid relief (Braganza, unpublished). This benefit concurs with a shift in thinking, namely, that ‘reductive stress’ is the common cause of reactive oxygen species generation in human pathology (Dormandy unpublished, acknowledged in reference [98]). There is a growing body of indirect supportive evidence for this [98, 99]. Reductive stress can be simplistically envisaged as an increase in ‘electron pressure’ just as acidosis is an increase in ‘proton pressure’: the two are in fact closely linked (Dormandy, personal opinion, unpublished). The body’s answer to reductive stress is probably to liberate labile methyl groups and generate methane which is exhaled, while ascorbic acid acts as counterpoise by generating carbon dioxide in reactions with hydrogen peroxide in the presence of iron [99]. Excess alcohol, ischaemia-reperfusion, redox cycling drugs, and uncouplers like non-steroidal antiinflammatory drugs and cyclosporine generate reductive stress. This is alleviated pharmacologically by electrophilic methyl groups as in choline [98], the prescription of which might circumvent the adverse effects, albeit theoretical, of prolonged methionine supplementation [87].
Corollary 1: Accommodating Genetic Links
Hereditary Pancreatitis
The large volume of genetic information has been reviewed twice in 2009 [100, 101]. There are six basic messages.
i) Gain-of-function mutations in the PRSS1 gene that encodes for cationic trypsinogen cause hereditary pancreatitis and are transmitted in autosomal dominant fashion, with 80% penetrance.
ii) PRSS1 mutations play little part in other forms of chronic pancreatitis.
iii) Loss-of-function mutations in the SPINK1 gene that encodes for serine protease inhibitor Kazal type 1 are strongly associated with idiopathic chronic pancreatitis, especially the tropical variant, but are seen as disease-modifying, not causative.
iv) The last point is also true for mutation in the CTRC gene that encodes for chymotrypsinogen, the active form of which degrades trypsin.
v) Genetic links with alcoholic chronic pancreatitis are modest.
vi) About 50% of patients have normal trypsin-related genes and also CFTR (see below).
The potent inhibitory effect of thiols on trypsin and other proteases is overlooked by proponents of the theory that mutations in trypsin-related genes are synonymous with pancreatic autodigestion [16]. The crucial mechanism of serine protease control by thiols was described 40 years ago and elucidated by Manchester scientists in elegant in-vitro studies [102, 103]. They showed that trypsin inhibition is a reversible reaction involving thiol-disulphide exchange; that the inhibited complex can be reactivated by oxidants; but that high concentrations of oxidants result in irreversible cleavage of the significant disulphide bond in trypsin, with permanent loss of activity. The inhibitory effect of glutathione on trypsin and protection by glutathione of trypsin-digestible substrates has been confirmed by others [27, 104]. Should any trypsin survive this cytosolic shield and escape into the pancreatic interstitium, it would encounter powerful inhibitors such as alpha-1 antitrypsin and beta-2 microglobulin.
Glutathione that is diverted for trypsin control in hereditary pancreatitis kindreds would compromise its availability for other vital functions: signal transduction; maintenance of redox balance; control of reactive oxygen species that are generated for many physiological roles; removal of reactive xenobiotic metabolites; cysteine replenishment; and protection of trans-sulphuration enzymes that ensure methyl flow (Figure 1) [27, 32]. The methyl-thiol shortfall rationalizes pancreatitis attacks. It also explains electrophilic stress as in studies from Cleveland [105] and Nantes [106]. Both found elevated superoxide dismutase in erythrocytes of patients as well as unaffected family members. Erythrocyte glutathione peroxidase was depressed to the same extent in each subset in the first study, but in the second unaffected members had increased levels such that only in patients was the enzyme ratio elevated - indicating unmitigated electrophilic stress. Patients had low selenium and in the Cleveland study also low vitamin E but elevated glutathione transferase. Thus as might have been anticipated, micronutrient therapy ameliorated symptoms in children with the disease (Table 1) [14].
Mutation in the Cystic Fibrosis Transmembrane Conductance Regulator Gene (CFTR)
The pancreatic lesion in cystic fibrosis is a diffuse form of chronic pancreatitis, the inflammatory stigmata lost when acinar tissue atrophies completely [107]. Hence observations on the pathogenesis of cystic fibrosis should be relevant to chronic pancreatitis, and vice versa. In 1998 two groups reported an increased frequency of CFTR mutations in patients with chronic pancreatitis [108, 109] and some with recurrent acute pancreatitis [109]. A recent review concluded that idiopathic chronic pancreatitis may occur with one abnormal allele but possession of two (as is usual and in some may represent a forme fruste of the disease [16]) confers a 40-fold increase in risk, rising to 500- fold when a SPINK1 mutation is present too [110]. Why?
The high concentration of trypsinogen in serum of the cystic fibrosis neonate falls exponentially in line with loss of acini until all are eradicated within the first decade. The pattern suggests a permanent blockade to apical exocytosis [15, 17, 111, 112], whereas that is an isolated event in acute pancreatitis (as after ERCP discussed above), but returns sporadically in recurrent acute pancreatitis and with greater frequency and duration in chronic pancreatitis [15]. Thus CFTR mutations could facilitate chronic pancreatitis by hindering exocytosis [15, 17, 112]. This interpretation requires the presence of CFTR in the luminal membrane of the normal acinar cell, as is indeed the case [113]. Studies using fluorescent probes, or confluent/semi-confluent cells that retain their secretory polarity [114] or, better still, studies on the isolated perfused cystic fibrosis pancreas, are needed to decide the concept’s validity in relation to acinar cells: using the first approach we have shown a failure of antibiotic exocytosis in upper airway cells [115]. The distinction between apical and basolateral discharge is difficult to make using secretagogues on acinar suspensions [112] because basolateral channels are sensitive to regulation too [19].
The findings of hyper-trypsinogenaemia in neonate cystic fibrosis carriers [116], and of the increased severity of caerulein pancreatitis in CFTR heterozygote mice [117] (but with redundant ductal channels for chloride transport), again point to the need for a full complement of CFTR protein for apical exocytosis. They do more, suggesting that the CFTR deficit is exposed by electrophilic strain, in that neonatal antioxidant systems are precarious [118], and, as noted earlier, experimental acute pancreatitis is detonated by an electrophilic burst. With evidence for continuous CYP-mediated strain in chronic pancreatitis and symptom control by micronutrient therapy irrespective of CFTR status [108], the obvious next question was whether CFTR may be targeted by toxic electrophiles [15, 27]. Recent studies confirm that it is [119, 120]. Oxidants as in cigarette smoke decrease CFTR expression and compromise CFTR function in vivo (as gauged by nasal potential difference studies) and in vitro [119]. Conversely, ascorbic acid promotes channel opening [121] as also do thiols [122].
It is no surprise that the 90% reduction in CFTR protein in compound heterozygotes with idiopathic chronic pancreatitis results in abnormal nasal potential difference and sweat tests [110]. The key point is that in these sites high levels of CYP expression persist into adulthood [123], such that an increase in toxic electrophiles would impair CFTR function in the absence of CFTR mutations. Abnormal sweat tests in the following disparate groups can now be rationalized:
i) African patients with alcoholic chronic pancreatitis [124];
ii) Indian patients with trisomy 21 [125] - wherein an extra copy of superoxide dismutase increases the yield of reactive oxygen species; and
iii) patients with kwashiorkor-marasmus [126] who have an absolute lack of defence to elctrophiles [31].
Germane to these arguments, both abnormal sweat tests and elevated serum trypsinogen are documented in malnourished Canadian children [127, 128]. Of note too, nasal potential difference studies indicate CFTR dysfunction in patients with recurrent acute pancreatitis [129,130], as is associated with pancreas divisum [129], in keeping with electrophilic strain [5].
The final piece in the jigsaw of chronic pancreatitis pathogenesis, namely, intraductal calcifying precipitates in many patients with large-duct disease, is provided by new evidence that CFTR in the luminal membrane of duct cells is a channel not only for chloride but also for bicarbonate [131, 132] and glutathione [133]. A reduced quota of CFTR in chronic pancreatitis ductal cells (whether due to CFTR mutation, toxic metabolic stress via CYP or other means) would result in less bicarbonate and glutathione concentrations in pancreatic juice at a time when (between attacks) protein secretion from acinar cells is excessive and/or abnormal [4, 15, 27].
Experimental studies show that progressive acidification of acinar and ductal lumena jeopardizes endocytosis of shed granule membranes and impairs the solubilization of secreted (pro)enzymes, leading to the histological picture of both cystic fibrosis and large-duct chronic pancreatitis [134]: indeed, the importance of bicarbonate is underlined by a study of mice with disrupted cilia function [135]. The way in which bicarbonate lack could compromise removal of the calcium shield from secreted mucus to facilitate protein plug formation has been described [131], as also the key role of glutathione in lysing disulphide bonds in mucus [133]. In our unpublished preliminary work, concentrations of glutathione in pure pancreatic juice (collected endoscopically in the first 10 minutes after secretin) were 1.11, 1.67, 2.02 and 3.02 μmol/L in four healthy controls, but 0.29 μmol/L in a patient with idiopathic calcific chronic pancreatitis, increasing to 2.50 μmol/L after eight months on micronutrient therapy.
Miscellaneous
i) Mutation in the lipoprotein lipase gene predisposes to recurrent pancreatitis: micronutrient therapy controlled attacks without lowering serum triglycerides in three Manchester patients, of whom a young woman with small-duct chronic pancreatitis had undergone multiple pancreatic operations culminating in a failed attempt at total resection [136]. In a study from Taiwan, CFTR mutation rate was 26% in the group with hypertriglyceridaemia and pancreatitis, compared to 1.3% in the group without pancreatitis [137].
ii) Primary hyperparathyroidism is linked to chronic pancreatitis: in a study of 826 patients, only the subset with a history of pancreatitis had a mutation in SPINK1 and/or CFTR [138].
iii) Primary haemochromatosis usually causes pancreatic fibrosis, not classical chronic pancreatitis: intravenous micronutrient therapy offered rapid relief in an emaciated woman with calcific disease and a mass in the head of the gland, overcoming by thiols the potential danger of giving vitamin C in the presence of free iron [139].
A New Template for the Pathogenesis of Chronic Pancreatitis
This can be constructed (Figure 2) to accommodate all the information discussed so far. It now becomes possible to see that when environmental and genetic factors combine to cause methyl-thiol lack, as in tropical chronic pancreatitis, the disease begins at a young age and runs an accelerated course. Permutations and combinations among CYP induction, trypsin-favouring mutations, diet, and ductal CFTR involvement would determine outcome - whether large or small-duct chronic pancreatitis, or recurrent acute pancreatitis.

Figure 2. A template for the pathogenesis of chronic pancreatitis based upon arguments in the text. Environmental (top 2 blocks on left) and genetic
(top 2 on right) factors come together via lowered CH3 (methyl)-GSH (glutathione, main thiol) status in acinar cells to cause a secretory block,
‘pancreastasis’ [17]. A fall in functional CFTR (cystic fibrosis transmembrane conductance regulator protein) compounds that threat, while its loss in
duct cells drives towards large-duct disease. Arrows indicate consequences of preceding events. Note the bidirectional relationship between methyl
and thiol status wherein methyl lack signifies lack of sulph-adenosylmethionine for GSH synthesis by way of cysteine; while low GSH leaves transsulphuration
enzymes vulnerable to attack by ROS/RXS and thereby jeopardizes delivery of methyl groups for signal transduction. Plus symbols
represent activation/increase, negative symbols decrease/inhibition. Gene mutations are shown in italics. Abbreviations are listed alphabetically. AA:
ascorbic acid; ACP: alcoholic chronic pancreatitis; C18:2: linoleic acid; CFTR: cystic fibrosis transmembrane conductance regulator protein; CYP:
cytochromes P450; HP: hereditary chronic pancreatitis; FROP: free radical oxidation products; GP-2: protein of the zymogen granule membrane
analogous to that in renal casts; GSH: glutathione; H2S: hydrogen sulphide; HCO3-: bicarbonate; ICP: idiopathic chronic pancreatitis; meth:
methionine; PAF: platelet activating factor initially from the acinar cell and then the mast cell [17]; ROS: reactive oxygen species; RXS: reactive
xenobiotic species; Se: selenium; SH: non-protein thiols; TCP: tropical chronic pancreatitis.
Corollary 2: Understanding Demography
There is a need to explain:
i) the high frequency of chronic pancreatitis in underprivileged communities [33, 140];
ii) 40% concurrence of gallstones and chronic pancreatitis in China where alcoholic chronic pancreatitis is infrequent [141];
iii) susceptibility of African Americans to both chronic pancreatitis and pancreatic cancer [3, 142]; and
iv) increased risk of that tumour in patients with chronic pancreatitis [3, 15, 16].
All this is rationalized within the framework of CYPrelated pathology, with poor pre-morbid intake of methyl/thiol precursors as a linking thread. The validity of the explanation is underlined, respectively, by:
i) low micronutrient status from foodstuffs inaffordability, not increased oxidation due to ‘Bantu siderosis’ [143], in non-alcoholic and alcoholic controls at Soweto where alcoholic chronic pancreatitis is rife [33], as also from hostile cooking practices in Madras where idiopathic disease predominates[75];
ii) dietary/ biochemical studies in relation to gallstones [144, 145];
iii) studies showing high intrinsic CYPA1 activity in African Americans [146], which would amplify the risk from reactive xenobiotic metabolites;
iv) high intrinsic activity of CYP2A6 which tends to bioactivate procarcinogens [147], the roles of reactive oxygen and xenobiotic species in carcinogenesis in general [148] and, in particular, the link between low methyl status and pancreatic cancer [55, 149].
Corollary 3: Opportunity for Prophylaxis
There is an opportunity for prophylaxis by a daily micronutrient tablet in groups at high risk of chronic pancreatitis, as in hereditary pancreatitis kindreds, patients lacking lipoprotein lipase and workers in particular industries. Population prophylaxis should be considered in areas where chronic pancreatitis is endemic. The scientific way would be to tailor tablet composition according to identified need: vitamin C with beta carotene in south India [75], or with selenium in Soweto [33]. The practical solution may be a daily tablet of a compound formulation. Apart from humane considerations, the economic gain should be considerable.
Conclusion
Hitherto environmental and genetic “causes” of chronic pancreatitis seemed to be poles apart. The success of micronutrient therapy across the board makes it possible to draw together these two pathogenetic strands. Chronic pancreatitis emerges as a good (perhaps the best) example of “chaos theory” as applied to medicine: an electrophilic strike on a metabolic pathway that has devastating consequences. Fortunately in this instance there is a simple way of prevention.
Acknowledgement
We thank Dr. C Brooking and Dr. D Brooking for preparing the Figures. We thank Dr. FN Leach, former Head of the North West Regional Drug Information Unit, United Kingdom, for advice on drug nomenclature
Conflict of interest
None
References
- Cawley T. A singular case of diabetes, consisting entirely in the quantity of urine: With an inquiry into the different theories of the disease. Lond Med J 1788; 9:286-308.
- Ahmad SA, Lowy AM, Wray CJ, D'Alessio D, Choe KA, James LE, et al. Factors associated with insulin and narcotic independence after islet autotransplantation in patients with severe chronic pancreatitis. J Am CollSurg 2005; 201:680-7. [PMID 16256909]
- Braganza JM. Pancreatic disease: a casualty of hepatic 'detoxification'? Lancet 1983; ii:1000-3. [PMID 6138545]
- Braganza JM. The pancreas. Recent AdvGastroenterolLond, Churchill-Livingstone, 1986; 6:251-80.
- Guyan PM, Uden S, Braganza JM. Heightened free radical activity in pancreatitis. Free RadicBiol Med 1990; 8:347-54. [PMID 2379863]
- Uden S, Bilton D, Nathan L, Hunt LP, Main C, Braganza JM. Antioxidant therapy for recurrent pancreatitis: placebo-controlled trial. Aliment PharmacolTher 1990; 4:357-71. [PMID 2103755]
- Uden S, Schofield D, Miller PF, Day JP, Bottiglieri T, Braganza JM. Antioxidant therapy for recurrent pancreatitis: biochemical profiles in a placebo-controlled trial. Aliment PharmacolTher 1992; 6:229-40. [PMID 1600043]
- Bilton D, Schofield D, Mei G, Kay PM, Bottiglieri T, Braganza JM. Placebo-controlled trials of antioxidant therapy including Sadenosulmethionine in patients with recurrent non-gallstone pancreatitis. Drug Invest 1994; 8:10-20.
- McCloy R. Chronic pancreatitis at Manchester, UK. Focus on antioxidant therapy. Digestion 1998; 59(Suppl 4):36-48. [PMID 9832634]
- Bhardwaj P, GargPK, Maulik SK, Saraya A, TandonRK, Acharya SK. A randomized controlled trial of antioxidant supplementation for pain relief in patients with chronic pancreatitis. Gastroenterology 2009; 136:149-59. [PMID 18952082]
- De lasHerasCastaño G, García de la Paz A, Fernández MD, FernándezForcelledo JL. Use of antioxidants to treat pain in chronic pancreatitis. Rev EspEnferm Dig 2000; 92;381-85. [PMID 10985097]
- Kirk GR, White JS, McKie L, Stevenson M, Young I, Clements WD, Rowlands BJ. Combined antioxidant therapy reduces pain and improves quality of life in chronic pancreatitis. J GastrointestSurg 2006; 10:499-503. [PMID 16627214]
- Dítě P, Precechtelová M, Novotný I, Soška V, Źáková A, Lata J. Changes of reactive oxidative substances in patients with morphologically different degrees of chronic pancreatitis and effects of long-term therapy with natural antioxidants. GastroenterologiaPolska 2003; 10: 379-83.
- Uomo G, Talamini G, Rabitti PG. Antioxidant treatment in hereditary pancreatitis. A pilot study on three young patients. Dig Liver Dis 2001; 33:58-62. [PMID 11303976]
- Braganza JM. The pathogenesis of chronic pancreatitis. QJM 1996; 89:243-50. [PMID 8733510]
- Mitchell RM, Byrne MF, Baillie J. Pancreatitis. Lancet 2003; 361:1447-55. [PMID 12727412]
- Braganza JM. Towards a novel treatment strategy for acute pancreatitis. 1. Reappraisal of the evidence on aetiogenesis. Digestion 2001; 63:69-91. [PMID 11244246]
- Lin TM, Grossman MI. Reversal by DL-methionine of acute effect of DL-ethionine on pancreatic enzyme output in dogs. Am J Physiol 1954; 176: 377-80. [PMID 16193325]
- Cook LJ, Musa OA, Case RM. Intracellular transport of pancreatic enzymes. Scand J Gastroenterol 1996; 31(Suppl 219):1-5. [PMID 8865462]
- Rinderknecht H. Acute necrotizing pancreatitis and its complications: an excessive reaction of natural defence mechanisms? In: Braganza JM (ed). The pathogenesis of Pancreatitis Manchester, UK: Manchester University Press, 1990; 86-100.
- GaisanoHY, GorelickFS. New insights into the mechanisms of pancreatitis. Gastroenterology 2009; 136:2020-4. [PMID 19379751]
- Halangk W, Krüger B, Ruthenbürger M, Stürzebecher J, Albrecht E, Lippert H, Lerch MM. Trypsin activity is not involved in premature intrapancreatictrypsinogen activation. Am J PhysiolGastrointest Liver Physiol 2002; 282: G367-74. [PMID 11804859]
- Gaiser S, Ahler A, Gundling F, Kruse ML, Savkovic V, Selig L, et al. Expression of mutated cationic trypsinogen reduces cellular viability in AR4-2J cells. BochimBiophys Res Commun 2005; 334:721- 8. [PMID 16036133]
- Mantke R, Schubert D, Röcken C, Paege I, Halangk W, Peters B, et al. Caerulein or taurocholate induced enzymatic and histologic alterations in the isolated perfused rat pancreas. Langenbecks Arch Surg 2009; 394:363-9. [PMID 18690472]
- Braganza JM. Towards a novel treatment strategy for acute pancreatitis. 2. Principles and potential practice. Digestion 2001; 63:143-62. [PMID 11351142]
- Leung PS, Chan YC. Role of oxidative stress in pancreatic inflammation. Antioxid Redox Signal 2009 ;11:135-65. [PMID 18837654]
- Braganza JM. A framework for the pathogenesis of chronic pancreatitis. Digestion 1998; 59(Suppl 4):1-12. [PMID 9832631]
- Jin CX, Hayakawa T, Kitagawa M, Ishiguro H. Lactoferrin in chronic pancreatitis. JOP. J Pancreas (Online) 2009; 10:237-41. [PMID 19454813]
- Houston JM. Cytochromes P450 in chronic pancreatitis. In: Braganza JM (ed). The Pathogenesis of Pancreatitis Manchester, UK: Manchester University Press 1991: 103-14.
- Gonzalez FJ. Role of cytochromes P450 in chemical toxicity and oxidative stress: studies with CYP2E1. Mutat Res 2005; 569:101-10. [PMID 15603755]
- Golden MHN. The exocrine pancreas in severe malnutrition. In: Braganza JM (ed). The Pathogenesis of Pancreatitis Manchester, UK: Manchester University Press 1991: 139-55.
- Wallig M. Xenobiotic metabolism, oxidant stress and chronic pancreatitis. Digestion 1998; 59(Suppl 4):13-24. [PMID 9832632]
- Segal I. Pancreatitis in Soweto, South Africa. Focus on alcoholrelated disease. Digestion 1998; 59(Suppl 4):25-35. [PMID 9832633]
- Chowdhury P, Gupta P. Pathophysiology of alcoholic pancreatitis: an overview. World J Gastroenterol 2006; 12:7421-7. [PMID 17167828]
- Askari MD, Tsao MS, Cekanova M, Schuller HM. Ethanol and the tobacco-specific carcinogen, NNK, contribute to signaling in immortalized human pancreatic duct epithelial cells. Pancreas 2006; 33:53-62. [PMID 16804413]
- Li J, Guo M, Hu B, Liu R, Wang R, Tang C. Does chronic ethanol intake cause chronic pancreatitis?: evidence and mechanism. Pancreas 2008; 37:189-95. [PMID 18665082]
- Strubelt O. Interactions between ethanol and other hepatotoxic agents. BiochemPharmacol 1980; 29: 1445-9. [PMID 6994745]
- McNamee R, Braganza JM, Hogg J, Leck I, Rose P, Cherry NM. Occupational exposure to hydrocarbons and chronic pancreatitis: a case-referent study. Occup Environ Med 1994; 51:631-7. [PMID 7951796]
- Jeppe CY, Smith MD. Transversal descriptive study of xenobiotic exposures in patients with chronic pancreatitis and pancreatic cancer. JOP. J Pancreas (Online) 2008; 9:235-9. [PMID 18326937]
- Braganza JM, John S, Padmalayam I, Mohan V, Viswanathan M, Chari S, Madanagopalan M. Xenobiotics and tropical chronic pancreatitis. Int J Pancreatol 1990; 7:231-45.
- Acheson DW, Hunt LP, Rose P, Houston JB, Braganza JM. Factors contributing to the accelerated clearance of theophylline and antipyrine in adults with exocrine pancreatic disease. ClinSci (Lond) 1989; 76:377-85. [PMID 2714050]
- Foster JR, Idle JR, Hardwick JP, Bars R, Scott P, Braganza JM. Induction of drug-metabolizing enzymes in human pancreatic cancer and chronic pancreatitis. J Pathol 1993;169:457-63. [PMID 8501544]
- Wacke R, Kirchner A, Prall F, Nizze H, Schmidt W, Fischer U, et al. Up-regulation of cytochrome P4501A2, 2C9 and 2E1 in chronic pancreatitis. Pancreas 1998; 16:521-8. [PMID 9598815]
- Standop J, Schneider M, Ulrich A, Büchler MW, Pour PM. Differences in immunohistochemical expression of xenobioticmetabolizing enzymes between normal pancreas, chronic pancreatitis and pancreatic cancer. ToxicolPathol 2003; 31:506-13. [PMID 14692619]
- Schoenberg MH, Büchler M, Pietrzyk C, Uhl W, Birk D, Eisele S, et al. Lipid peroxidation and glutathione metabolism in chronic pancreatitis. Pancreas 1995; 10:36-43. [PMID 7899458]
- Santini SA, Spada C, Bononi F, Foschia F, Mutignani M, Perri V, et al. Liver, pancreas and biliary tract enhanced lipoperoxidation products in pure pancreatic juice: evidence for organ-specific oxidative stress in chronic pancreatitis. Dig Liver Dis 2003; 35:888- 92. [PMID 14703885]
- Pai GC, RaoMNS. Evidence for oxidant stress in chronic pancreatitis. Indian J Gastroenterol 1999; 18:156-7. [PMID 10531717]
- GutteridgeJMC. Lipid peroxidation and antioxidants as biomarkers of tissue damage. ClinChem 1995; 41:1819-28. [PMID 7497639]
- Weber H, Merkord J, Jonas L, Wagner A, Schröder H, Käding U, et al. Oxygen radical generation and acute pancreatitis: effects of dibutyltin dichloride/ethanol and ethanol on rat pancreas. Pancreas 1995; 11:382-8. [PMID 8532655]
- Ulrich AB, Schmied BM, Matsuzaki H, Lawson TA, Freiss H, Andrén-Sandberg A, et al. Increased expression of glutathione Stransferase- pi in the islets of patients with primary chronic pancreatitis but not secondary chronic pancreatitis. Pancreas 2001; 22:388-94. [PMID 11345140]
- Ulrich AB, Schmied BM, Standop J, Schneider MB, Lawson TA, Friess H, et al. Differences in the expression of glutathione Stransferases in normal pancreas, chronic pancreatitis, secondary chronic pancreatitis, and pancreatic cancer. Pancreas 2002; 24:291-7. [PMID 11893938]
- Hausmann DH, Porstmann T, Weber I, Hausmann S, Dummler W, Liebe S, Emmrich J. Cu/Zn-SOD in human pancreatic tissue and pancreatic juice. Int J Pancreatol 1997; 22:207-13. [PMID 9444552]
- Cullen JJ, Mitros FA, OberleyLW. Expression of antioxidant enzymes in diseases of the human pancreas: another link between chronic pancreatitis and pancreatic cancer. Pancreas 2003; 26:23-7. [PMID 12499913]
- Brown LA. Glutathione protects signal transduction in type II cells under oxidant stress. Am J Physiol 1994; 266: 172-7. [PMID 7511342]
- Longnecker DS. Abnormal methyl metabolism in pancreatic toxicity and diabetes. J Nutr 2002; 132:2373-6s. [PMID 12163695]
- Mårtensson J, Bolin T. Sulfur amino acid metabolism in chronic relapsing pancreatitis. Am J Gastroenterol 1986; 81:1179-84. [PMID 3788926]
- Verlaan M, Roelofs HM, van-Schaik A, WantenGJ, Jansen JB, Peters WH, Drenth JP. Assessment of oxidative stress in chronic pancreatitis patients. World J Gastroenterol 2006; 12:5705-10. [PMID 17007026]
- Sajewicz W, Milnerowicz S, Nabzdyk S. Blood plasma antioxidant defense in patients with pancreatitis. Pancreas 2006; 32:139-44. [PMID 16552332]
- Schrader H, Menge BA, Belyaev O, Uhl W, Schmidt WE, Meier JJ. Amino acid metabolism in patients with chronic pancreatitis and pancreatic carcinoma. Pancreas 2009; 38:416-21. [PMID 19169171]
- Syrota A, Dop-Ngassa M, Paraf A. 11C-L-methionine for evaluation of pancreatic exocrine function. Gut 1981; 22:907-15. [PMID 6171485]
- Schemann M, Grundy D. Role of hydrogen sulfide in visceral nociception. Gut 2009; 58:744-6. [PMID 19433593]
- Morselli-LabateAM, Fantini L, Pezzilli R. Hydrogen sulfide, nitric oxide and a molecular mass 66 u substance in the exhaled breath of chronic pancreatitis patients. Pancreatology 2007; 7:497- 504. [PMID 17912017]
- Nishimura S, Fukushima O, Ishikura H, Takahashi T, Matsunami M, Tsujiuchi T, et al. Hydrogen sulfide as a novel mediator for pancreatic pain in rodents. Gut 2009; 58:762-70. [PMID 19201768]
- RahmanSH, Nanny C, Ibrahim K, O'Reilly D, Larvin M, KingsnorthAJ, McMahon MJ. Genetic polymorphisms of GSTT1, GSTM1, GSTP1, MnSOD, and catalase in nonhereditary chronic pancreatitis: evidence of xenobiotic stress and impaired antioxidant capacity. Dig Dis Sci 2005; 50:1376-83. [PMID 16047490]
- Osterreicher CH, Schultheiss J, Wehler M, Homann N, Hellerbrand C, Künzli B, et al. Genetic polymorphisms of manganese-superoxide dismutase and glutathione-S-transferase in chronic alcoholic pancreatitis. Mutagenesis 2007; 22:305-10. [PMID 17548864]
- Verlaan M, HarbersEG, Pap A, Jansen JB, Peters WH, Drenth JP. Paraoxonase 1-192Q allele is a risk factor for idiopathic chronic pancreatitis. MolDiagn 2005; 9:9-15. [PMID 16035730]
- Uden S, Acheson DW, Reeves J, Worthington HV, Hunt LP, Brown S, Braganza JM. Antioxidants, enzyme induction, and chronic pancreatitis: a reappraisal following studies in patients on anticonvulsants. Eur J ClinNutr 1988; 42:561-9. [PMID 3224602]
- Braganza JM, Hewitt C, Day JP. Serum selenium concentration in chronic pancreatitis: lowest values during painful exacerbations. Trace Elem Med 1988; 5: 79-84.
- Van Gossum A, Closset P, Noel E, Cremer M, Neve J. Deficiency in antioxidant factors in patients with alcohol-related chronic pancreatitis. Dig Dis Sci 1996; 41:1225-31. [PMID 8654156]
- Morris-Stiff GJ, Bowrey DJ, Oleesky D, Davies M, Clark GW, Puntis MC. The antioxidant profiles of patients with recurrent acute and chronic pancreatitis. Am J Gastroenterol 1999; 94:2135-40. [PMID 10445540]
- Vaona B, Stanzial AM, Talamini G, Bovo P, Corrocher R, Cavallini G. Serum selenium concentrations in chronic pancreatitis and controls. Dig Liver Dis 2005; 37:522-5. [PMID 15975540]
- Schulz KF, Grimes DA. Sample size calculations in randomised trials: mandatory and mystical. Lancet 2005; 365:1348-53. [PMID 15823387]
- Schofield D, Braganza JM. Shortcomings of an automated assay for total antioxidant status in biological fluids. ClinChem 1996; 42:1712-14. [PMID 8855160]
- Benzie IFF, Strain JJ. The ferric reducing ability of plasma (FRAP) as a measure of "antioxidant power": the FRAP assay. Anal Biochem 1996; 239:70-6. [PMID 8660627]
- Braganza JM, Schofield D, Snehalatha C, Mohan V. Micronutrient antioxidant status in tropical compared with temperate-zone chronic pancreatitis. Scand J Gastroenterol 1993; 28: 1098-104. [PMID 8303214]
- Scott PD, Knoop M, McMahon RFT, Braganza JM, Hutchinson IV. S-Adenosyl-L-Methionine protects against haemorrhagic pancreatitis in partially immunosuppressed pancreaticoduodenal transplant recipients. Drug Invest 1992; 4(Suppl 4):69-77.
- de Las Heras-Castaño G, García-Unzueta MT, Domínguez-Diez A, Fernández-González MD, García-de la Paz AM, Mayorga- Fernández M, Fernández-Fernández F. Pancreatic fibrosis in rats and its response to antioxidant treatment. JOP. J Pancreas (Online) 2005; 6:316-24. [PMID 16006681]
- Nonaka A, Manabe T, Tobe T. Effect of a new synthetic ascorbic acid derivative as a free radical scavenger on the development of acute pancreatitis in mice. Gut 1991; 32:528-32. [PMID 1710198]
- Nonaka A, Manabe T, Kyogoku T, Tamura K, Tobe T. Evidence for a role of free radicals by synthesized scavenger, 2- octadecylascorbic acid, in cerulein-induced mouse acute pancreatitis. Dig Dis Sci 1992; 37:274-9. [PMID 1370933]
- Lu XL, Song YH, Fu YB, Si JM, QianKD. Ascorbic acid alleviates pancreatic damage induced by dibutyltin dichloride (DBTC) in rats. Yonsei Med J 2007; 48:1028-34. [PMID 18159597]
- SwieryJH, Mann GE. Role of oxidative stress in the pathogenesis of acute pancreatitis. Scand J Gastroenterol 1996; 31(Suppl 219):10-5. [PMID 8865464]
- Arnold R, Fodov G, Mathelier H, Mohasci T, Szent-Györgyi A, VeltriRW. Recent aspects of the chemistry of vitamin C. In: McBrienDCH, Slater TF (eds). Protective Agents in Cancer London, UK :Academic Press 1983:197-213.
- Sowell J, Frei B, Stevens JF. Vitamin C conjugates of genotoxic lipid peroxidation products: structural characterization and detection in human plasma. ProcNatlAcadSci USA 2004; 101:17964-9. [PMID 15608056]
- Winkler BS. Unequivocal evidence in support of the nonenzymatic redox coupling between glutathione/glutathione disulfide and ascorbic acid/dehydroascorbic acid. BiochimBiophysActa 1992, 1117:287-90. [PMID 1420278]
- Mårtensson J, Han J, Griffith OW, Meister A. Glutathione ester delays the onset of scurvy in ascorbate-deficient guinea pigs. ProcNatlAcadSci USA 1993; 90:317-21. [PMID 8419936]
- Lieb JG 2nd, Forsmark CE. Review article: pain and chronic pancreatitis. Aliment PharmacolTher 2009; 29:706-19. [PMID 19284407]
- Grimble RF. The effects of sulfur amino acid intake on immune function in humans. J Nutr 2006; 136:1660S-5s. [PMID 16702336]
- Zimnoch L, Szynaka B, Puchalski Z. Mast cells and pancreatic stellate cells in chronic pancreatitis with differently intensified fibrosis. Hepatogastroenterology 2002; 49:1135-8. [PMID 12143220]
- Dib M, Zhao X, Wang X, Andersson R. Mast cells contribute to early pancreatitis-induced systemic endothelial barrier dysfunction. Pancreatology 2002; 2:396-401. [PMID 12138228]
- Hoogerwerf WA, Gondesen K, Xiao SY, Winston JH, Willis WD, PasrichaPJ. The role of mast cells in the pathogenesis of pain in chronic pancreatitis. BMC Gastroenterol 2005; 5:8. [PMID 15745445]
- Salim AS. Role of oxygen-derived free radical scavengers in the treatment of recurrent pain produced by chronic pancreatitis. Arch Surg 1991; 126:1109-14. [PMID 1929842]
- Yoshida A, Yokono O, Oda T. Therapeutic effect of chlorophyll-A in the treatment of patients with chronic pancreatitis. GastroenterolJpn 1980; 15:49-61. [PMID 6153629]
- Banks PA, Hughes M, Ferrante M, Noordhoek EC, Ramagopal V, Slivka A. Does allopurinol reduce pain of chronic pancreatitis? Int J Pancreatol 1997; 22:171-6. [PMID 9444547]
- Durgaprasad S, Pai CG, Vasanthkumar, AlvresJF, Namitha S. A pilot study of the antioxidant effect of curcumin in tropical pancreatitis. Indian J Med Res 2005; 122:315-8. [PMID 16394323]
- Szuster-Ciesielska A, Daniluk J, Kandefer-Szerszen M. Oxidative stress in blood of patients with alcohol-related pancreatitis. Pancreas 2001; 22:261-6. [PMID 11291927]
- Banerjee B, Bagchi D. Beneficial effects of a novel IH636 grape seed proanthocyanidin extract in the treatment of chronic pancreatitis. Digestion 2001; 63:203-6. [PMID 11351148]
- Leach FN, Braganza JM. Treatment of recurrent pancreatitis with antioxidants. Hosp Pharmacist 1997; 4:169-71.
- Ghyczy M, Boros M. Electrophilic methyl groups present in the diet ameliorate pathological states induced by reductive and oxidative stress: a hypothesis. Br J Nutr 2001; 85:409-14. [PMID 11348555]
- Ghyczy M, Torday C, Boros M. Simultaneous generation of methane, carbon dioxide, and carbon monoxide from choline and ascorbic acid: a defensive mechanism against reductive stress? FASEB J 2003; 17:1124-6. [PMID 12692080]
- Chen JM, Férec C. Chronic pancreatitis: genetics and pathogenesis. Annu Rev Genomics Hum Genet 2009; 10:63-87. [PMID 19453252]
- Mahurkar S, Reddy DN, RaoGV, Chandak GR. Genetic mechanisms underlying the pathogenesis of tropical calcific pancreatitis. World J Gastroenterol 2009; 21:256-69. [PMID 19140225]
- Steven FS, Al-Habib A. Inhibition of trypsin and chymotrypsin by thiols. Biphasic kinetics of reactivation and inhibition induced by sodium periodate addition. BiochimBiophysActa 1979; 568:408-15. [PMID 226148]
- Steven FS, Griffin MM. Studies on the molecular mechanism of mersalyl and 4-aminophenylmercuric acetate re-activation of trypsinthiol complexes. Eur J Biochem 1980; 109:567-73. [PMID 7408902]
- Chauhan UP. Glutathione as inhibitor of trypsin induced proteolysis. Indian J ExpBiol 1989; 27:472-3. [PMID 2599558]
- Mathew P, Wyllie R, Van Lente F, Steffen RM, Kay MH. Antioxidants in hereditary pancreatitis. Am J Gastroenterol 1996; 91:1558-62. [PMID 8759661]
- Georgelin T, Schnee M, Sagniez M, Bailly F, Naudot I, Soulard FM, Martin F. Antioxidant status in patients with hereditary chronic pancreatitis (HCP) and alcoholics. Gastroenterology 1998; 114: A461.
- Dodge JA. Paediatric and hereditary aspects of chronic pancreatitis. Digestion 1998; 59(Suppl 4):49-59. [PMID 9832635]
- Sharer N, Schwarz M, Malone G, Howarth A, Painter J, Super M, Braganza J. Mutations of the cystic fibrosis gene in patients with chronic pancreatitis. N Engl J Med 1998; 339:645-52. [PMID 9725921]
- Cohn JA, Friedman KJ, Noone PG, Knowles MR, Silverman LM, Jowell PS. Relation between mutations of the cystic fibrosis gene and idiopathic pancreatitis. N Engl J Med 1998; 339:653-8. [PMID 9725922]
- Cohn JA. Reduced CFTR function and the pathobiology of idiopathic pancreatitis. J ClinGastroenterol 2005; 39:S70-7. [PMID 15758663]
- Uden S, Bilton D, Guyan PM, Kay PM, Braganza JM. Rationale for antioxidant therapy in pancreatitis and cystic fibrosis.AdvExp Med Biol 1990; 264:555-72. [PMID 2244539]
- Tang S, Beharry S, Kent G, Durie PR. Synergistic effects of cAMP- and calcium-mediated amylase secretion in isolated pancreatic acini from cystic fibrosis mice. Pediatric Res 1999; 45:482-8. [PMID 10203138]
- Zeng W, Lee MG, Yan M, Diaz J, Benjamin I, Marino CR, et al. Immuno and functional characterization of CFTR in submandibular and pancreatic acinar and duct cells. Am J Physiol Cell Physiol 1997; 273:C442-5. [PMID 9277342]
- Morris AP, Frizzell RA. Vesicle targeting and ion secretion in epithelial cells: implications for cystic fibrosis. Annu Rev Physiol 1994; 56:371-97. [PMID 7516644]
- QuesnelLB, Jaran AS, Braganza JM. Antibiotic accumulation and membrane trafficking in cystic fibrosis cells.J AntimicrobChemother 1998; 41:215-21. [PMID 9533463]
- Scotet V, De Braekeleer M, Audrézet MP, Lodé L, Verlingue C, Quéré I, et al. Prevalence of CFTR mutations in hypertrypsinaemia detected through neonatal screening for cystic fibrosis. Clin Genet 2001; 59:42-7. [PMID 11168024]
- Liu Q, Fischer H, Welch WJ, Harris HW. Cerulein-induced acute pancreatitis is more severe in mice heterozygous for the DF508 cystic fibrosis transmembrane conductance regulator gene mutation than wild-type controls. J Surg Res 2000; 93:317-8.
- Lee YS, Chou YH. Antioxidant profiles in full term and preterm neonates. Chang Gung Med J 2005; 28:846-51. [PMID 16515018]
- Cantin AM, HanrahanJW, Bilodeau G, Ellis L, Dupuis A, Liao J, et al. Cystic fibrosis transmembrane conductance regulator function is suppressed in cigarette smokers. Am J RespCrit Care Med 2006; 173:1139-44. [PMID 16497995]
- Schwarzer C, Fischer H, Kim EJ, Barber KJ, Mills AD, KurthMJ, et al. Oxidative stress caused by pyocyanin impairs CFTRCl(-) transport in human bronchial epithelial cells. Free RadicBiol Med 2008; 45:1653-62. [PMID 18845244]
- Fischer H, Schwarzer C, Illek B. Vitamin C controls the cystic fibrosis transmembrane conductance regulator chloride channel. Proc National AcadSci 2004; 101:3691-6. [PMID 14993613]
- Köttgen M, Busch AE, Hug MJ, Greger R, Kunzelmann K. NAcetyl- L-cysteine and its derivatives activate a Cl- conductance in epithelial cells. Pflugers Arch 1996; 431-549-55. [PMID 8596698]
- Braganza JM. Cystic fibrosis: a casualty of 'detoxification'? Med Hypotheses 1986; 20:233-43. [PMID 3637621]
- Bank S, Marks IN, Novis B. Sweat electrolytes in chronic pancreatitis. Am J Dig Dis 1978; 23:178-81. [PMID 623082]
- Geetha H, Shetty KT. Sweat osmolality in Down's syndrome and cystic fibrosis in an Indian population. Brit Med J 1987; 294:156. [PMID 2954606]
- Yigit H, Selimoglu MA, Altinkaynak S. Sweat test results in children with primary protein energy malnutrition. J PediatrGastroenterolNutr 2003; 37:242-5. [PMID 12960643]
- Beck R, Durie PR, Hill JG, Levison H. Malnutrition: a cause of elevated sweat chloride concentration. ActaPaediatrScand 1986; 75:639-44. [PMID 3751557]
- Durie PR, ForstnerGG, Gaskin KJ, Weizman Z, KopelmanHR, Ellis L, Largman C. Elevated serum immunoreactive pancreatic cationic trypsinogen in acute malnutrition: evidence of pancreatic damage. J Pediatr 1985; 106:233-8. [PMID 3968610]
- Gelrud A, Sheth S, Banerjee S, Weed D, Shea J, Chuttani R, et al. Analysis of cystic fibrosis gener product (CFTR) function in patients with pancreas divisum and recurrent acute pancreatitis. Am J Gastroenterol 2004; 99:1557-62. [PMID 15307877]
- Segal I, Yaakov Y, Adler S, Blau H, Broide E, Santo M, et al. Cystic fibrosis transmembrane conductance regulator ion channel function testing in recurrent acute pancreatitis. J ClinGastroenterol 2008; 42:810-4. [PMID 18360295]
- Quinton PM. Cystic fibrosis: impaired bicarbonate secretion and mucoviscidosis. Lancet 2008; 372:415-7. [PMID 18675692]
- Ishiguro H, Steward MC, Naruse S, Ko SB, Goto H, Case RM, et al. CFTR functions as a bicarbonate channel in pancreatic duct cells. J Gen Physiol 2009; 133:315-26. [PMID 19204187]
- Hudson VM. New insights into the pathogenesis of cystic fibrosis: pivotal role of glutathione system dysfunction and implications for therapy. Treat Respir Med 2004; 3:353-63. [PMID 15658882]
- Freedman SD. New concepts in understanding the pathophysiology of chronic pancreatitis.Int J Pancreatol 1998; 24:1- 8. [PMID 9746883]
- Zhang Q, Davenport JR, CroyleMJ, Haycraft CJ, Yoder BK. Disruption of IFT results in both exocrine and endocrine abnormalities in the pancreas of Tg737(orpk) mutant mice. Lab Invest 2005; 85:45-64. [PMID 15580285]
- Heaney AP, Sharer N, Rameh B, Braganza JM, DurringtonPN. Prevention of recurrent pancreatitis in familial lipoprotein lipase deficiency with high-dose antioxidant therapy.J ClinEndocrinMetab 1999; 84:1203-5. [PMID 10199753]
- Chang YT, Chang MC, Su TC, Liang PC, Su YN, Kuo CH, et al. Association of cystic fibrosis transmembrane conductance regulator (CFTR) mutation/variant/haplotype and tumor necrosis factor (TNF) promoter polymorphism in hyperlipidemic pancreatitis. ClinChem 2008; 54:131-8. [PMID 17981921]
- Felderbauer P, Karakas E, Fendrich V, Bulut K, Horn T, Lebert R, et al. Pancreatitis risk in primary hyperparathyroidism: relation to mutations in the SPINK1 trypsin inhibitor (N34S) and the cystic fibrosis gene. Am J Gastroenterol 2008; 103:368-74. [PMID 18076731]
- Sharer NM, Taylor PM, Linaker BD, GutteridgeJMC, Braganza JM. Safe and successful use of vitamin C to treat painful calcific chronic pancreatitis despite iron overload from primary haemochromatosis.Clin Drug Invest 1995;10:310-5.
- GargPK, TandonRK. Survey on chronic pancreatitis in the Asia-Pacific region. J GastroenterolHepatol 2004; 19:998-1004. [PMID 15304116]
- Yan MX, Li YQ. Gall stones and chronic pancreatitis: the black box in between. Postgrad Med j 2006; 82:254-8. [PMID 16597812]
- Lowenfels AB, Maisonneuve P, Grover H, Gerber E, Korsten MA, Antunes MT, et al. Racial factors and the risk of chronic pancreatitis. Am J Gastroenterol 1999; 94: 790-4. [PMID 10086667]
- Segal I, Sharer NM, Kay PM, GutteridgeJM, Braganza JM. Iron, ascorbate and copper status of Sowetan Blacks with calcific chronic pancreatitis.QJM 1996; 89:49-53. [PMID 8730342]
- Simon JA, HudesES. Serum ascorbic acid and gallbladder disease prevalence among US adults: the Third National Health and Nutrition Examination Survey (NHANES III). Arch Int Med 2000; 160:931-6. [PMID 10761957]
- Worthington HV, Hunt LP, McCloyRF, UbbinkJB, Braganza JM. Dietary antioxidant lack, impaired hepatic glutathione reserve, and cholesterol gallstones. ClinChimActa 2004; 349: 157-65. [PMID 15469869]
- Johnson JA, Herring VL, Wolfe MS, Relling MV. CYP1A2 and CYP2D6 4-hydroxylate propranolol and both reactions exhibit racial differences. J PharmacolExpTher 2000; 294:1099-105. [PMID 10945865]
- Kadlubar S, Anderson JP, Sweeney C, Gross MD, Lang NP, KadlubarFF, Anderson KE. Phenotypic CYP2A6 variation and the risk of pancreatic cancer.JOP. J Pancreas (Online) 2009; 10: 263-70. [PMID 19454817]
- Guyton KZ, Kenslev TW. Oxidative mechanisms in carcinogenesis. In: CheesemanKH, Slater TF (eds). Free Radicals in Medicine. London, UK: Churchill Livingstone 1993: 523-44.
- Larsson SC, Giovannucci E, Wolk A. Folate intake, MTHFR polymorphisms, and risk of esophageal, gastric, and pancreatic cancer: a meta-analysis. Gastroenterology 2006; 131:1271-83. [PMID 17030196]


