Key words
health needs assessment, health planning,
modernisation agenda, prison health
Introduction
Modernisation is usually thought of as an NHS
phenomenon but already its influence has spread
beyond health and social care. There are challenges
associated with providing good continuing healthcare
to people who become prisoners, but we believe that
prison healthcare can benefit greatly from participating
in modernisation activity alongside the NHS.
From our experience of supporting a local prison in
undertaking health needs assessment and developing
its health improvement planning, we have been able
to observe modernisation beginning to work in prison
healthcare planning and this has occurred over a
relatively short period of time. Evidence that planning
has moved on is easy to generate, but demonstrating
direct benefits to patients is less easy. Nevertheless it
will ultimately be important to do so because improving
the health of people who become prisoners can
potentially benefit not only the individual but also the
communities to which they return, and it is therefore
essential to be sure that innovations are effective.Here we report on a brief survey of how prison healthcare
staff currently view modernisation and its perceived
benefits for patients.
Background
Prisoners and their health
In outlining the case for a major reform of prison
healthcare, the NHS Executive recognised that it is
inappropriate when considering prison healthcare to
regard prisons as ‘distinct entities which have little
relevance for or impact on the wider community’.[1]
They highlighted the transient nature of the prison
population, most of whom will ultimately return to
the wider community ‘taking with them their health
and social problems’.1 Data compiled by the Home
Once showed that over half (56.8%) of prisonerswere
serving less than six months.[2] Even life-sentenced
prisoners are likely to serve a limited time in prison – for example the 127 life-sentenced prisoners who
were released from prisons in England and Wales in
2000 had served an average of 13.3 years.[2]
It is also significant that many prisoners come from
sections of the population that may be ‘dincult to
reach in any other situation, and for many a spell in
prison represents an opportunity for consistent contact
with health services’.[1] According to the Home
Once, 91.7% of people entering prison in 2000 were
men, with around half (50.2%) aged under 30 and
around four-fifths (82.9%) under 40.2 The 1997
survey carried out by the Once for National Statistics
(ONS) indicated that a high proportion had been
taken into local authority care as children (ranging
from around a quarter of female sentenced prisoners
to a third of male remand prisoners).[3] The vast
majority had experienced at least one stressful life
event such as running away from home, serious
money problems, relationship breakdown or bereavement,
and about half had experienced five or more
such events. Around half of those surveyed had no
educational qualifications and many (around two-
fifths) reported having left school before their 16th
birthday with almost 1 in 10 reporting that they had
left school before age 13.
Although the benefits of better healthcare in prisons
both for prisoners themselves and for the wider
community are clear, the provision of healthcare
presents particular challenges. There is a high incidence
of mental health issues, for example. The ONS
survey reported that about 20% of male respondents
and 40% of female respondents had received treatment
for a mental or emotional problem in the
12 months before entering prison.3 In addition the
reported rates of suicide attempts were very high,
especially amongst the remand prisoners, with 27% of
male remand prisoners reporting that they had
attempted suicide at some time in their lives, 15%
in the year before interview and 2% in the previous
week. It has been reported that around 80% of male
sentenced prisoners smoke and around 24% of adult
prisoners have injected drugs at some time.[4,5] Of those
who reported having injected drugs 20% were
infected with hepatitis B and 30% with hepatitis C.[5]
There is also the transient nature of the prison
population and the issues that this raises for providing
continuity of healthcare.
Given the challenges of providing good continuing
healthcare to people who become prisoners, but the
obvious potential benefits for addressing health
inequalities by improving their general health, it is
important that the modernisation agenda extends to
and is effective in the prison setting.
Modernisation and prison healthcare:
intentions
Historically, prison healthcare has been separate from
the NHS. In 1996, Her Majesty’s Chief Inspector of
Prisons called for the responsibility for healthcare
provision to move from the Prison Service to the
NHS.[6] A working group was jointly established by the
Home Secretary and the Secretary of State for Health
to look at this issue and reported in 1999.[1] The
working group found that some prison establishments
were making progress towards meeting the
existing aim of giving ‘prisoners access to the same
quality and range of healthcare services as the general
public receives from the National Health Service’.[1]
However, they also reported that there was considerable
variation in the ‘organisation and delivery, quality,
funding, effectiveness and links with the NHS’.[1]
They described prison healthcare as having been
characterised by services developed on an ad hoc
basis to suit custodial or organisational requirements
rather than based on the health needs of prisoners and
this has led to ‘questions about equity, standards
{and} professional isolation’.[1] The working group
recommended the establishment of a formal partnership
between the NHS and the Prison Service but that
funding and departmental accountabilities remain
with the Home Once.
At a national level, this resulted in the establishment
of a Prison Health Policy Unit and Prison
Health Taskforce in April 2000 and a Development
Work Programme which encompasses services, workforce
and performance management. In December
2002 to aid effective integration between the Prison
Service and the NHS these two bodies formed a single
Prison Heath Development Unit.[7]
Regional prison health taskforces were established
to support prisons and health authorities to ‘drive
forward the assessment of need’ and prison health
improvement programmes.[1] In 1999, health authorities
had joint responsibility alongside their prison
partners for conducting a health needs assessment and
developing a prison health improvement programme.
As a result of Shifting the Balance of Power the NHS
side of this responsibility has devolved to the host
primary care trust (PCT) i.e. the PCT within which
the prison is geographically located.[8] Guidance on the
process of needs assessment and health improvement
planning has been issued and prisons and their NHS
partners will shortly start their third round of needs
assessment activity.[9–11]
From April 2003, the budgetary responsibility for
commissioning prison healthcare will be transferred
from the Home Once to the Department of Health
with the ultimate aim of devolving commissioning of
prison healthcare to the host PCT level.[12]
Modernisation and prison healthcare:
reality
Within the prison establishments themselves, modernisation
has primarily focused on the systematic
identification of healthcare need and the development
and implementation of health improvement plans to
meet this need. We have supported prisons in two
rounds of needs assessment and planning within
prison healthcare in which we have had the opportunity
to observe directly how modernisation has been
taken up and to confirm and test our impressions by
consulting with colleagues elsewhere. Specifically, we
decided to survey prison healthcare staff within the
prisons that make up the government onces for
Yorkshire and the Humber and the North East (GO
Y&H and NE) to:
• identify what NHS–prison partnership arrangements
are in place in prisons within the geographical
region GO Y&H and NE
• explore the experience of healthcare staff involved
in the development of needs assessment and health
improvement planning
• identify evidence of examples of direct benefits to
patients arising out of the development of health
improvement plans.
We recognised that a survey at this early stage of the
uptake of modernisation by prisons would not
demonstrate conclusively that patients were directly
benefiting. However, we hoped to provide initial
insights into how modernisation was operating and
whether a larger survey or more detailed evaluation is
warranted.
Survey of the prisons within GO
Y&H and NE
Methodological approach
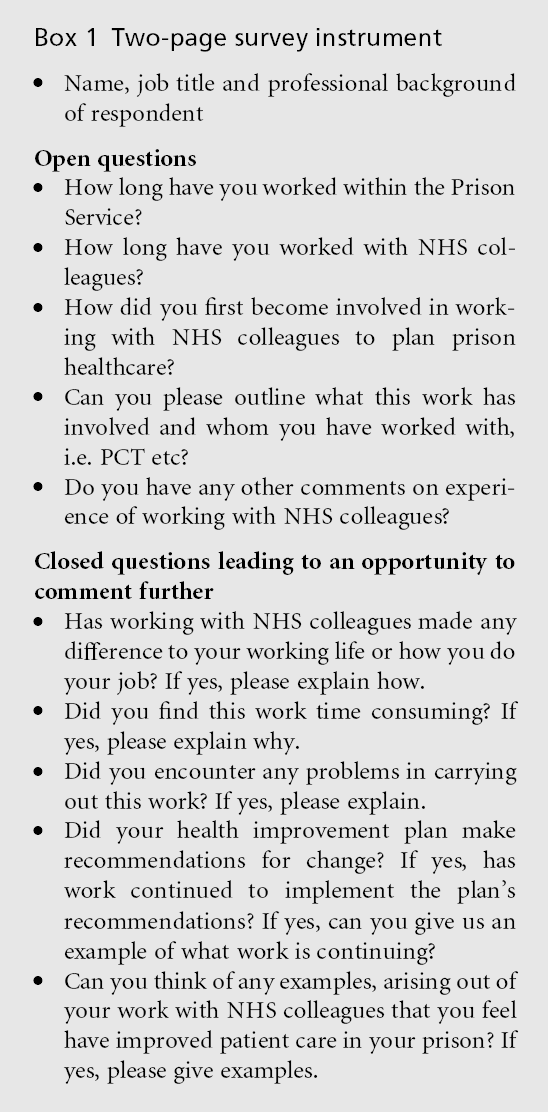
We aimed to explore how prison healthcare staff have
found the experience of working with NHS colleagues
to assess health need and plan prison healthcare, and
in particular to gather examples of developments
which they felt had improved patient care. We drew
on our experiences of needs assessment and planning
in prisons to design and interpret replies to a brief
two-page survey instrument (see Box 1 for content)
which we administered via each establishment’s governing
governor. Governing governors were asked to
pass the questionnaire on to an appropriate member
of their healthcare team, i.e. someone who had been
involved in the development of their health improvement
plan.
Ethical Approval
We sought and gained ethical approval for the survey
from Hull and East Riding Local Research Committee
and gained support from the Regional Prison Health
Taskforce (Northern and Yorkshire).
Findings
Respondents
We received responses from 14 of the 22 prisons
surveyed. For the most part the survey was completed
by prison healthcare staff with a nursing background.
Of these, there was an equal split between general and
mental health nursing.We also had respondents from
both a medical and prison governor background.
Generally, the survey was answered by the people we
expected it to be passed on to, i.e. people whom we were aware had been involved in implementing the
modernisation agenda. The respondents had worked
for the Prison Service for between 14 months and
26 years but even the longer serving respondents
had only fairly recently engaged with NHS colleagues,
i.e. post-1997, to plan services.
Partnerships
Every prison from which a response was received was
able to demonstrate the existence of partnerships with
the NHS. Many referred to formal joint arrangements,
e.g. a Prison Health Steering Group and even of those
who did not, all but one described having a range of
contacts within the NHS. PCTs, strategic health
authorities, health action zones, NHS workforce confederations,
acute trusts, community trusts, public
health departments and the prison health taskforce
were all referred to.
Achievements and problems
We found clear evidence that the modernisation
agenda has taken a hold in prisons for example:
• The majority of respondents identified aspects of
the modernisation agenda in prisons (i.e. the task
of completing a health needs assessment etc) as the
main stimulus for working with their NHS colleagues
although pre-existing relationships sometimes
made this easier.
• Virtually all respondents described undertaking
new initiatives that are clearly linked with the
modernisation agenda. For example: health needs
assessment, mental health needs assessment, mental
health in-reach, clinical governance, electronic
medical records, shared protocols, joint conferences
etc were all mentioned by our respondents.
• In addition, there were several examples whereby
existing services were enhanced because of easier
access to specialists, e.g. specialist diabetic nurse or
specialised services, e.g. CCDC (Consultant in
Communicable Disease Control).
• There were also several positive comments around
the reduction of professional isolation and the
ability to access support, advice and up-to-date
knowledge. One respondent stated ‘{I} feel more
part of a team and less isolated, now {I} have
people that I can contact in a professional capacity’.
However, the majority of respondents described dif-
ficulties with developing a health improvement plan
beginning with needs assessment. One of the biggest
dinculties was the time-consuming nature of this
process especially given the lack of familiarity with
health needs assessment at a population level within
the Prison Service. Also, the lack of additional resources
and dedicated time meant that within some
prisons a single person ‘had to do most of the work’. One respondent described the process as time
consuming because of the need to ‘go into depth and
identify deficits’. Some respondents felt that needs
assessment requires the collection of a great deal of
background information and quantitative data. This
was described as particularly dincult because of the
lack of information technology in the prison setting.
There was also the need to spend time outside the
prison attending meetings with NHS colleagues.
Reference was made to the various quality improvement
initiatives of which needs assessment and planning
is but one alongside prison health standards
audit, clinical governance, ‘tranc lights’ etc all requiring
individual action plans.[11,13] Finally, several
respondents reported that their partnerships had to
work to overcome the differing cultures and objectives
of the NHS and Prison Service, in particular the
compromise between care on the one hand and
correction on the other. One respondent expressed
this as ‘the main problem is that both organisations
have vastly different cultures and structures which can
lead to dinculties; also, both organisations have
different primary goals/objectives’, and another respondent
emphasised that ‘trying to balance NHS
policies with those of the Prison Service has been a
major dinculty’. Additionally, one respondent made
the distinction between ‘orders and instructions’ in
the Prison Service and ‘protocols and guidelines’
within the NHS.
Nevertheless, all respondents stated that their
health action plans included recommendations for
change or development and that further work had
been undertaken to implement the recommendations.
In particular, most respondents stated that
new services had been developed, e.g. day care, sexual
health, nurse-led clinics, additional external staff
sessions, e.g. psychiatry, genitourinary medicine etc.
Many of the respondents also described setting up
mental health in-reach services. Another aspect that
many of these prisons had looked at was reviewing
skill-mix and staff development, and examples of
progress in this area were cited. Some respondents
also described developing clinical governance
mechanisms and the regular review of the health
action plans. Respondents also welcomed the
increased accountability and one respondent linked
the introduction of clinical governance with
‘enhanced patient care’.
We asked respondents whether they could give us
examples, arising out of their work with NHS colleagues
that they felt had improved patient care in
their prison. The vast majority of respondents were
able to list numerous examples, which are summarised
in Box 2.

It is encouraging that despite the dinculties presented
by modernisation and outlined above there
was a strong perception that healthcare in prisons had already improved. As a result, several respondents
were able to describe their overall experience of
working with the NHS in a positive light. We noted
the following responses in particular:
‘These have been demanding times in which all staff have
been stretched. However, the experience has been
rewarding in regards that all staff have put in increased
effort but have the satisfaction of seeing a better service in
partnership with the NHS.’
‘I have found the NHS to be responsive, helpful and above
all enthusiastic to the idea of taking forward healthcare
{in this prison}.’
‘The relationship with the PCT and local prison{s} in {. . .}
appears to improve constantly, building trust and effective
partnership working.’
Discussion
Although we did not set out to demonstrate conclusively
that modernisation of health services within
prisons has resulted in direct benefits for patients, we
consider we have found some encouraging evidence
that this is probably the case. Our findings are limited
by this not being a national survey. Also the response
rate was lower than we would have liked but we opted
not to follow up non-responders. In any case this is
not an epidemiological study, for which response rate
would be crucial. Rather our aim at this early stage of
evaluation was not to quantify how many prisons
could demonstrate benefits from modernisation but
rather to determine if any considered that they could.
We considered that a larger, more sophisticated study
though ultimately desirable was not warranted at this
early stage, if indeed it is currently possible.
We feel that our approach of gathering the impressions
from staff, backed up by concrete examples has
provided encouraging evidence that the processes of
modernisation are embedding in prisons. As to
whether modernisation has had benefits for patients,
all but one of the 14 responding prisons were able to
cite numerous examples of modernisation-linked
service developments. We therefore feel it is likely
that there is a multitude of similar examples throughout
the prison estate. An early task should be to
initiate systematic identification of the range of
initiatives in place as a precursor to generating robust
evidence of what works and specifically what works
and why in specific prison settings. Unfortunately,
prisons currently lack both the culture and the capacity
to undertake systematic evaluation. Even within
PCTs, robust evaluation of small-scale modernisation
initiatives such as those described here seems uncommon.
Nevertheless, there is real opportunity to build
upon the momentum generated by the modernisation
agenda to build research and evaluation capacity by
capitalising on the new dynamic partnerships that
have been created. We would encourage prisons and
PCTs to seek academic partners to support them in
this.
Acknowledgements
We would like to acknowledge the support and hard
work of the members of the Prison Health Steering
Group at HMP Hull, in particular Sue Altass (clinical
healthcare manager), Pat Costello (head of healthcare)
and Dr Peter Saunders (acting clinical director)
from HMP Hull, Peter England (public health specialist)
from Eastern Hull PCT and Dr Richard Turner
(consultant in public health medicine) from West
Hull PCT. Thanks are also due to the governing
governors and survey respondents of the 14 prisons
who responded to our survey. We welcomed their
comprehensive responses and insights. We are also
grateful to Paul Fallon – Regional Prison Health Lead,
Northern and Yorkshire Regional Prison Health
Taskforce, Directorate of Health and Social Care:
North – for support in conducting this survey.
HTJ and SH are funded by the four PCTs in Hull and
the East Riding of Yorkshire.
References
- HM Prison Service, NHS Executive (1999) The Future Organisation of Prison HealthCare: report by the Joint Prison Service and National Health Service Executive Working Group. The Stationery O¤ce: London.
- Office for National Statistics,HomeO¤ce (2000) Prison Statistics England and Wales 2000. ONS: London.
- SingeltonN, Meltzer H, Gatwood R, Coid J andDeasyD (1998) Psychiatric Morbidity among Prisoners: summaryreport. A survey carried out in 1997 by the Social Survey Division of ONS on behalf of the Department of Health. The Stationery O¤ce: London.
- Bridgwood A and Malbon G (1995) Survey of the Physical Health of Prisoners 1994. A survey of sentenced male prisoners in England and Wales, carried out by the Social Survey Division of OPCS on behalf of the Prison Service Health Care Directorate. HMSO: London.
- Weild A, Gill O, Livingstone S, Parry J and Curran L (2000) Prevalence of HIV, hepatitis B, and hepatitis C antibodies in prisoners in England and Wales: a national survey. Communicable Disease and Public Health 3: 121–6.
- Her Majesty’s Chief Inspector of Prisons (1996) Patient or Prisoner? A new strategy for health care in prisons. Discussion Paper. The Home O¤ce: London.
- Department of Health, HM Prison Service, Welsh Assembly Government (2003) Prison Health Handbook Revised January 2003. The Stationery O¤ce: London.
- Department of Health (2001) Shifting the Balance of Power within the NHS. Securing Delivery. Department of Health: London.
- Marshall T, Simpson S and Stevens A (2000) Toolkit for Health Care Need Assessment in Prisons. The University of Birmingham: Birmingham.
- Department of Health, HM Prison Service, Welsh Assembly Government (2002) Guidance on Developing Prison Health Needs Assessments and Health Improvement Plans. The Stationery O¤ce: London.
- HM Prison Service (2002) Health Services for Prisoners Standard (3e). HM Prison Service: London.
- Narey M (2002) Letter to Governing Governors. 24th September 2002. Department of Health: London.
- HM Prison Service (2003) Clinical Governance: quality in prison healthcare. Prison Service Order 3100. Department of Health: London.

