Keywords
Morbidity; Pancreas; Pancreatectomy; Retroperitoneal Neoplasms; Sarcoma
Abbreviations
ISGPS: International Study Group of Pancreatic Surgery
INTRODUCTION
Surgery for abdominal mesenchymal tumors may be challenging because of their association with the resection of different visceral organs. Some recent reports show that, as a frontline aggressive surgical approach (liberal en-bloc resection of most of the adjacent uninvolved organs when in proximity of the tumor surface) to primary retroperitoneal sarcomas, it is associated with improved local control [1, 2, 3].
Pancreatic resections are known to have an acceptable risk of morbidity and mortality when carried out at high volume centers for pancreatic diseases [4, 5].
There is only one paper reporting on morbidity and mortality caused by a pancreatectomy when performed in the context of a multivisceral resection [6].
Given their size at presentation, mesenchymal neoplasms are typically treated by extended procedures. We recently reported on the overall morbidity of these extended procedures in a large series of primary retroperitoneal sarcomas from two referral institutions [1]. No association between the resection of the left pancreas and specifically increased morbidity in comparison to other organs was found. We wanted to investigate whether the resection of the left pancreas in our series of multivisceral resections for abdominal mesenchymal neoplasms was as safe as the only similar one reported [6] and/or the numerous straightforward resections [7, 8, 9, 10, 11, 12, 13, 14, 15].
METHODS
This study investigated all patients surgically treated at the National Cancer Institute, Milan, Italy from January 1997 to May 2009 for abdominal mesenchymal neoplasms, the resection of which required a concomitant left pancreatectomy. It was based on clinical data retrieved from both the prospective sarcoma database of our institution and patients’ clinical charts.
The standard preoperative investigation consisted of a contrast-enhanced abdominal and thoracic computed tomography for all patients. The preoperative risk was graded according to the American Society of Anesthesiologists (ASA) classification.
All resections were performed via laparotomy. Sectioning of the pancreas was performed in all cases but one using a mechanical stapler (1 Proximate® Reloadable Linear Cutter with Safety Lock-out 55 mm Ref. TCT55; Ethicon Endosurgery, Johnson & Johnson Co., Cincinnati, OH; stapler dimension before closure 3.0x4.5 mm); in one patient, manual suturing was used. Silicon drain tubes of 21Ch diameter (Rusch, Duluth, GA, USA) were always placed in the abdomen during surgery and were removed postoperatively, according to the quality (absence of pancreatic component) and quantity (less than 50 mL per day) of the output. Amylase levels were routinely measured in the drain tubes on postoperative days 1 and 3. Further measurements were taken only if clinically needed.
A left pancreatectomy has often been associated with the resection of other major organs, such as the spleen, kidney and left colon as part of a multivisceral resection, performed to obtain tumor excision with surrounding healthy tissue. The opportunity of performing a left pancreatic resection was considered, in the preoperative setting, in order to obtain wide healthy tissue margins around the tumor when radiological examination showed a free tumor margin of 1 cm or less between the tumor and the pancreatic tissue.
Surgical resections were classified as macroscopically complete (R0 or R1) or not (R2), because the anatomic location of retroperitoneal sarcomas makes it difficult to achieve a reliable microscopic assessment of the margins in a retrospective review.
As far as histological types are concerned, all tumors were reviewed during the course of the study by at least two experienced pathologists.
All complementary treatments were administered on the basis of decisions made by the multidisciplinary Institutional Sarcoma Board. However, no prospectively selected criteria were used to this end. Chemotherapy was given according to the standard regimens used at the time or within institutional/multiinstitutional clinical trials. Radiation therapy was delivered through external beams at doses ranging from 36 to 65 grays (Gy) (median: 50 Gy). Overall, the timing of both treatments was equally distributed in the preoperative and postoperative setting, but a higher tendency to administer them preoperatively was observed recently.
Operative notes, and postoperative hospital and outpatient records were reviewed for all patients. All complications were recorded prospectively in the database and in the patients’ case histories.
Postoperative hospital stay, histopathology of the resected pancreas, surgical technique of the pancreatic resection, preoperative chemo-radiotherapy, development of postoperative pancreatic fistula and overall postoperative morbidity and mortality were evaluated.
We considered only intraoperative and postoperative surgery-related complications. The mortality rate was defined as the total in-hospital death rate, a surgical related mortality within three months from surgery or non surgical-related mortality due to a complication occurring within 30 days from surgery.
Postoperative pancreatic fistula was defined as outlined by the International Study Group on Pancreatic Fistula (ISGPF) classification [7]: “output via an operatively placed drain (or a subsequently placed, percutaneous drain) of any measurable volume of drain fluid on or after postoperative day 3, with an amylase content greater than 3 times the upper normal serum value”. Postoperative pancreatic fistula was also graded as A, B and C with respect to the clinical impact [5].
Delayed gastric emptying was defined according to the scale provided by the International Study Group of Pancreatic Surgery (ISGPS) [16].
The management of postoperative pancreatic fistulae was also analyzed with particular attention paid to its treatment and the possible need for re-exploration.
STATISTICS
Median, range and frequencies were used as descriptive statistics. Overall survival from the time of surgery at our institution was calculated by using Kaplan-Meier estimates. Data were analyzed by means of the PASW Statistics 18 package (https://support.spss.com/productsext/statistics/documen tation/18/clientindex.html).
ETHICS
All patients gave signed informed written consent for data collection, analysis and interpretation. The study protocol conforms to the ethical guidelines of the “World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004, and was approved by the institutional review board of the “National Cancer Institute”.
RESULTS
In 57 patients affected by localized left retroperitoneal soft tissue sarcoma, gastrointestinal stromal tumors (GISTs) or other mesenchymal tumors of borderline malignancy, surgical resection and a concomitant left pancreatectomy were performed. The patients’ median age at diagnosis was 55 years (range: 32-85 years). Twenty-seven (47.4%) patients were female and 30 (52.6%) were male. The median size of the tumors was 18 cm (range: 8-50 cm).
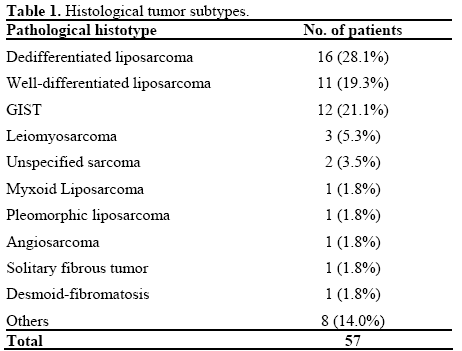
In 14 patients (24.6%) a pancreatic tail resection was performed while 43 patients (75.4%) underwent a pancreatic body-tail resection extending from the left side of the portal-mesenteric axis. The median operative time was 290 min (range: 180-540 min). As expected, the most common histologic subtype was liposarcoma since this type of tumor prevails at this site. All different histologic subtypes are listed in Table 1.
Neoplastic pancreatic involvement was documented at pathology in 26 patients (45.6%); 31 cases (54.4%) had no direct involvement of the pancreatic tissue. Only rarely did resected uninvolved pancreata show inflammatory-fibrous processes (4 patients, 7.0%). Of the 11 patients affected by GISTs, neoplastic involvement of the pancreas was detected in 4 cases (36.4%).
A macroscopically complete resection was achieved in all but three patients: one patient had a locally advanced retroperitoneal liposarcoma involving the hepatic hilus and superior mesenteric vessels and the other two had large gastric GISTs resistant to imatinib and underwent a surgical resection of the progressive lesions.
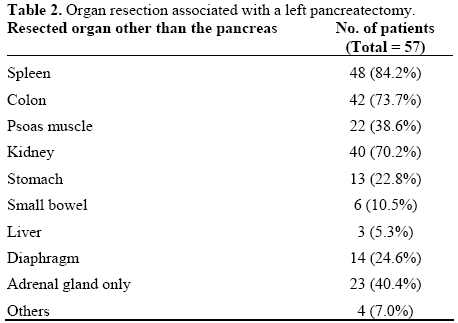
A left pancreatectomy was always associated with other major organ resections, in particular, the spleen, left or right colon and kidney (48, 42, and 40 patients, respectively). In nine cases, a splenectomy had been performed before the patient was referred to our center: no spleen-preserving procedure was ever attempted at our center. The organ resections associated with a left pancreatectomy are listed in Table 2.
Complementary treatments were administered to 22 patients (38.6%): 5 patients (8.8%) received preoperative chemotherapy, 2 received radiotherapy (3.5%) and 6 (10.5%) both treatments. Nine (15.8%) patients underwent perioperative treatment with imatinib 400 mg/die. Thirty-five patients (61.4%) did not receive any preoperative treatment.
Thirty-two patients (56.1%) did not have any postoperative complications; 20 patients (35.1%) had at least one complication and 5 (8.8%) had two or more complications.
A second surgical procedure was necessary in four patients (7.0%) (two patients with postoperative bleeding and hemoperitoneum, one intra-abdominal collection resolved with a colostomy and evacuation of purulent fluids, and one gastric colo-pancreatic fistula).
Postoperative Morbidity
The most common complication was delayed gastric emptying; according to the scale provided by the ISGPS, delayed gastric emptying occurred in 9 patients (15.8%). No grade C delayed gastric emptying with need for interventional treatment occurred. In 2 patients, grade B delayed gastric emptying occurred; nutritional support with enteral nutrition via a nasogastric tube and the administration of prokinetic drugs was carried out. In 7 patients, delayed gastric emptying was classified as grade A; in all these cases, treatment with prokinetic drugs was administered with fast resolution of the complication.
Postoperative pancreatic fistulae occurred in seven (12.3%) patients (1 grade A, 5 grade B and 1 grade C) and are listed in Table 3.
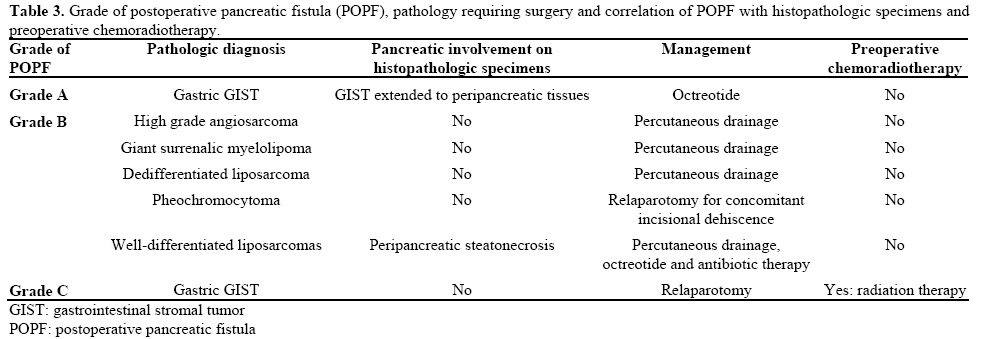
Most postoperative pancreatic fistulae were treated conservatively by drainage and octreotide administration; when postoperative pancreatic fistulae caused an intra-abdominal collection, antibiotic therapy was also administered and percutaneous drainage under computed tomography guidance was undertaken. Only two patients affected by postoperative pancreatic fistulae required a second surgical procedure. One patient, affected by a pheochromocytoma, suffered from incisional dehiscence concomitant with a postoperative pancreatic fistula and underwent a second laparotomy with drainage of the peripancreatic fluid collection and closure of the abdominal wall (reintervention was required for wound dehiscence). The second patient had a relaparotomy due to a gastric, colo-pancreatic fistula after multivisceral organ resection for a gastric GIST; he developed sepsis and died, and his management is subsequently described. No patients affected by retroperitoneal soft tissue sarcoma needed a second laparotomy for a postoperative pancreatic fistula. No patient had postoperative pancreatitis and, in the late postoperative course, pseudo-cystic fluid accumulation did not occur. In two patients (3.5%) general physical decay (weight loss, cachexia, asthenia) concomitant with postoperative pancreatic fistulae (grade B) occurred; they underwent percutaneous drainage and total parenteral nutrition with an improvement in symptoms. New-onset permanent insulin-dependent diabetes occurred in three patients (5.3%) while no sign of exocrine insufficiency (weight loss or steatorrhea) was detected in any of the patients.
Clostridium difficilis diarrhea occurred in one patient (1.8%), probably due to prolonged antibiotic therapy and one patient (1.8%) developed wound infection.
Postoperative Mortality
Death from causes directly or indirectly related to the surgery occurred in two patients (3.5%). Both patients had suffered from postoperative pancreatic fistulae (grades C and B, respectively). The first death occurred in a patient who underwent a splenopancreatectomy associated with the long gastric curve and left colon flexure resection for a gastric GIST infiltrating the colon and pancreas in the pre-imatinib era (1999). A gastric colono-pancreatic fistula occurred and a relaparotomy was performed, but the patient died one month after surgery from sepsis and multiple organ failure. The second patient died from pneumonia 3 months after surgery due to a retroperitoneal dedifferentiated liposarcoma; resection of the tumor mass en-bloc with the left colon, spleen, tail of the pancreas, kidney, adrenal gland and part of the left diaphragm had been performed. A grade B postoperative pancreatic fistula and intra-abdominal collections occurred postoperatively and were managed by insertion of an external drain with resolution of the complication. After discharge, the patient developed pneumonia from unknown causes and died during hospitalization in another hospital.
No apparent correlation between preoperative chemoradiotherapy and the development of postoperative pancreatic fistulae was detectable; only one patient with a postoperative pancreatic fistula underwent neoadjuvant treatment. No relationship between histologic subtype and postoperative pancreatic fistula was detected (data not shown).
The patient who developed a grade C postoperative pancreatic fistula had neoplastic pancreatic involvement at surgical specimen examination; the pathological diagnosis revealed a gastric GIST extending to the peripancreatic soft tissues.
After a median follow-up of 32 months (interquartile range: 20-57 months) for the 45 surviving patients, the overall survival at 5 years of the entire populations was 67.0% (Figure 1).
Figure 1. Kaplan-Meier estimates of overall survival for the entire series.
DISCUSSION
In our series of 57 patients who underwent a left pancreatectomy as part of a multivisceral resection for an abdominal mesenchymal tumor, the incidence of postoperative pancreatic fistulae was 12.3% with a related mortality rate of 3.5%.
Pancreatic resection was historically associated with significant postoperative morbidity and mortality. However, in recent years, many reports from high volume pancreatic surgery centers have described a significant improvement in outcome after both a pancreaticoduodenectomy and a left pancreatectomy. The incidence of postoperative mortality, overall morbidity and pancreatic fistulae after a left pancreatectomy vary from 0.9 to 3%, from 13 to 47% and from 5 to 31%, respectively in the literature [8, 9, 10, 11, 12].
The only formal retrospective comparison in a single institutional series between patients undergoing a distal pancreatectomy straightforwardly or as part of en-bloc resection for a contiguous tumor was recently reported by Irani et al. [6]. They did not find any significant difference in the overall complication rate in the two groups, showing that resection of the left pancreas did not have more complications when performed as part of multivisceral resections. Their data showed postoperative morbidity and mortality rates of 37% and 3%, respectively which were also comparable to what has been reported in other series of straightforward left pancreatic resection. Their most common complications were pancreatic duct leaks (23%) and intra-abdominal abscesses (7.6%) [6]
Our rates of both postoperative pancreatic fistula and mortality are very similar to what was reported by Irani et al.. Indeed, they are at least as good as those reported in the literature from the most important pancreatic high volume centers on straightforward pancreatic surgery. Worthy of note, their patients had mainly exclusive left pancreatic resection (with an associated splenectomy in most cases) while, in most of our cases, the left pancreas and spleen were resected en-bloc with at least one other abdominal organ. Moreover, the majority of our cases did not have inflammatory-fibrous processes in the pancreatic tissue at pathological examination (93%).
The variability observed among the different groups may be in part related to a selection bias and in part to the changes in the definition of postoperative fistulae since 1999. Nevertheless, all these reports show how, in the last decade, pancreatic resections have become safer procedures if performed by experienced surgeons in dedicated centers [13].
Some authors believe that a lower postoperative pancreatic fistula incidence occurs in pancreata with fibrosis or chronic inflammatory processes since the pancreatic tissue becomes harder (i.e. for peritumoral fibrosis or chronic pancreatitis) [13, 14, 15]. A soft and friable pancreas, as is found under normal conditions, could, in fact, be more prone to developing suturing failures [17]. Our series involved patients for the most part having a normal pancreas, as expected in the general population.
In this respect, the results of our pancreatic resections appear satisfactory and encourage an aggressive approach when needed.
From the technical standpoint, mechanical staplers were used to close the pancreatic stump in 56 patients while, in only one case was manual suturing employed. In the literature, the most appropriate way of closing the pancreatic remnant is still under debate; even between the largest high volume pancreatic surgical centers, there is no agreement regarding the best surgical technique [18]. In 2002, Fahy et al. reported the manual closure of the pancreatic stump as a risk factor for pancreatic leaks [19]; in 2003 Bilimoria et al. indicated failure to ligate the pancreatic duct as the only risk factor for pancreatic leaks [20]. In 2008, Ferrone et al. reported that, in their series, there was no difference in the rate of fistula formation between the different stump closure techniques [21]. In 2005, Knaebel et al., after a systematic review of the literature, reported that it was not possible to draw any firm conclusions on the optimal surgical technique for pancreatic stump closure; however, they described a trend in favor of the stapling technique [22]. Even Irani et al. could not ascertain the optimal method of pancreatic stump closure, as several other groups had tried, because a significant difference in the leak rate based on closure technique was not found (stapler vs. oversewn vs. both) [6]. Our results cannot help in resolving this issue since virtually all our patients underwent mechanical closure of the stump. Indeed, the way the stump is closed seems to have a limited - if any - impact on the risk of postoperative pancreatic fistulae.
We did observe a significantly delayed gastric emptying rate in our patients, although all patients eventually returned to normal food intake and weight. This is quite a rare event in straightforward left pancreatectomies. We believe that our findings may be a result of the extended retroperitoneal dissection related to these procedures rather than the left pancreatectomy itself. Nevertheless, all patients who underwent similar extended procedures without a left pancreatic resection did not experience any significant delayed gastric emptying. What then seems to cause it is the combination of an extended retroperitoneal dissection with a resection of the spleen and the left pancreas; this may be partially explained by the posterior displacement of the stomach.
Further studies are warranted to better understand its mechanisms and possibly address how to try to avoid it.
When, then, should a left pancreatectomy be associated with the resection of an abdominal mesenchymal neoplasm? There are conditions where it should be performed only if the gland is directly invaded (i.e., GISTs and tumors of borderline malignancy). The employment of effective preoperative treatment could be also considered whenever the risk of pancreatic involvement can be anticipated on cross sectional imaging. Conservative surgery should always be considered a goal. The availability of targeted therapies for GISTs has inaugurated a new era, even for patients affected by localized disease at difficult sites. Preoperative treatment with imatinib has proven to be effective and capable of improving the rate of organs spared and function-preserving procedures [23]. A left pancreatectomy should then be performed only in those rare situations when the tumor does not respond to therapy or the gland remains extensively invaded, even after medical treatment.
On the other hand, there are other conditions where this procedure could be offered to improve surgical margins (i.e., left retroperitoneal soft tissue sarcoma). Recent reports advocate the systematic employment of frontline aggressive surgery to improve local outcome and, possibly, survival in retroperitoneal soft tissue sarcoma. Local control of disease is the main goal in order to avoid recurrence in retroperitoneal soft tissue sarcomas; peritumoral resection can be an important risk factor for disease recurrence. Wide resection should be considered. These reports showed better results than those of most historical series [3]. The main concern preventing the systematic recommendation of this extended approach is the possible increased morbidity related to such procedures. A recent report of a combined series from two major institutions (including ours) has extensively analyzed the contribution of both the number and the quality of different resections to the risk of morbidity in the context of multivisceral resection for retroperitoneal soft tissue sarcoma [1]. The results were quite reassuring, although a left pancreatectomy was associated with a somewhat higher risk of complications in comparison to the resection of other abdominal organs. The results of the present series show that the morbidity associated with this procedure in the context of a multivisceral resection is comparable to that of a left pancreatectomy alone. In other words, the context of a multivisceral resection does not add to the risk of a left pancreatectomy [6].
It is well known that, in pancreatic surgery, the higher the volume of the center performing the procedure, the better the outcome [24, 25]. This has also been shown for surgery at many other critical sites [26] and it is also the case for abdominal mesenchymal tumors. An aggressive multivisceral approach should be undertaken only in specialized centers, with dedicated multidisciplinary teams and surgeons experienced in treating the disease.
In conclusion, given its acceptable morbidity, left pancreatic resection can be considered as part of the surgery for abdominal mesenchymal neoplasms. The decision whether or not to resect it should then be made taking into account the exact nature of the disease. Whenever possible, every effort should be made to spare the pancreas, but when the margins are crucial for cure, it must be resected to improve them, even in the absence of direct involvement.
Therefore, every effort should be made to deal with these cases in specialized centers in order to maximize the ratio between costs and benefits, and possibly increase the chance of cure.
Conflicts of interest
The authors have no potential conflicts of interest
References
- Bonvalot S, Miceli R, Berselli M, Causeret S, Colombo C, Mariani L, et al. Aggressive surgery in retroperitoneal soft tissue sarcoma carried out at high-volume centers is safe and is associated with improved local control. Ann Surg Oncol 2010; 17:1507-14. [PMID 20393803]
- Bonvalot S, Rivoire M, Castaing M, Stoeckle E, Le Cesne A, Blay JY, Laplanche A. Primary retroperitoneal sarcomas: a multivariate analysis of surgical factors associated with local control. J Clin Oncol 2009, 27:31-37. [PMID 19047280]
- Gronchi A, Lo Vullo S, Fiore M, Mussi C, Stacchiotti S, Collini P, et al. Aggressive surgical policies in a retrospectively reviewed single-institution case series of retroperitoneal soft tissue sarcoma patients. J Clin Oncol 2009, 27:24-30. [PMID 19047283]
- Van Heek NT, Kuhlmann KF, Scholten RJ, De Castro SM, Busch OR, Van Gulik TM, et al. Hospital volume and mortality after pancreatic resection: a systematic review and an evaluation of Intervention in The Netherlands. Ann Surg 2005; 242:781-8. [PMID 16327488]
- Lieberman MD, Kilburn H, Lindsey M, Brennan MF. Relation of perioperative deaths to hospital volume among patients undergoing pancreatic resection for malignancy. Ann Surg 1995; 222:638-45. [PMID 7487211]
- Irani JL, Ashley SW, Brooks DC, Osteen RT, Raut CP, Russell S, et al. Distal pancreatectomy is not associated with increased perioperative morbidity when performed as part of a multivisceral resection. J Gastroint Surg 2008; 12:2177-82. [PMID 18677539]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005; 138:8-13. [PMID 16003309]
- Lillemoe KD, Kaushal S, Cameron JL, Sohn TA, Pitt HA, Yeo CJ. Distal pancreatectomy: indications and outcomes in 235 patients. Ann Surg 1999; 229:693-8. [PMID 10235528]
- Kleeff J, Diener MK, Z'graggen K, Hinz U, Wagner M, Bachmann J, et al. Distal pancreatectomy risk factors for surgical failure in 302 consecutive cases. Ann Surg 2007; 245: 573-82. [PMID 17414606]
- Ferrone CR, Warshaw AL, Rattner DW, Berger D, Zheng H, Rawal B, et al. Pancreatic fistula rates after 462 distal pancreatectomies: staplers do not decrease fistula rate. J Gastrointest Surg 2008; 12:1691-7. [PMID 18704597]
- Goh BK, Tan YM, Chung YF, Cheow PC, Ong HS, Chan WH, et al. Critical appraisal of 232 consecutive distal pancreatectomies with emphasis on risk factors, outcome, and management of the postoperative pancreatic fistula. A 21-year experience at a single institution. Arch Surg 2008; 143:956-65. [PMID 18936374]
- Vin Y, Sima CS, Getrajdman GI, Brown KT, Covey A, Brennan MF, Allen PJ. Management and outcomes of postpancreatectomy fistula, leak, and abscess: results of 908 patients resected at a single institution between 2000 and 2005. J Am Coll Surg 2008; 207:490-8. [PMID 18926450]
- Liang TB, Bai XL, Zheng SS. Pancreatic fistula after pancreaticoduodenectomy: diagnosed according to International Study Group Pancreatic Fistula (ISGPF) definition. Pancreatology 2007; 7:325-31. [PMID 17627097]
- Yang YM, Tian XD, Zhuang Y, Wang WM, Wan YL, Huang YT. Risk factors of pancreatic leakage after pancreaticoduodenectomy. World J Gastroenterol 2005; 28;11:2456- 61. [PMID 15832417]
- Pedrazzoli S, Liessi G, Pasquali C, Ragazzi R, Berselli M, Sperti C. Postoperative pancreatic fistulas preventing severe complications and reducing reoperation and mortality rate. Ann Surg 2009; 249:97- 104. [PMID 19106683]
- Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, et al. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007; 142:761-8. [PMID 17981197]
- Mathur A, Pitt HA, Marine M, Saxena R, Schmidt CM, Howard TJ, et al. Fatty pancreas: a factor in postoperative pancreatic fistula. Ann Surg 2007; 246:1058-64. [PMID 18043111]
- Sheehan MK, Beck K, Creech S, Pickleman J, Aranha GV. Distal pancreatectomy: does the method of closure influence fistula formation? Am Surg 2002; 68:264-7. [PMID 11893105]
- Fahy BN, Frey CF, Ho HS, Beckett L, Bold RJ. Morbidity, mortality, and technical factors of distal pancreatectomy. Am J Surg 2002; 183:237-41. [PMID 11943118]
- Bilimoria MM, Cormier JN, Mun Y, Lee JE, Evans DB, Pisters PW. Pancreatic leak after left pancreatectomy is reduced following main pancreatic duct ligation. Br J Surg 2003; 90:190-6. [PMID 12555295]
- Knaebel HP, Diener MK, Wente MN, Büchler MW, Seiler CM. Systematic review and meta-analysis of technique for closure of the pancreatic remnant after distal pancreatectomy. Br J Surg 2005; 92:539-46. [PMID 15852419]
- Maki RG. Recent advances in therapy for gastrointestinal stromal tumors. Curr Oncol Rep 2007; 9:165-9. [PMID 17430686]
- Neoptolemos JP, Russell RC, Bramhall S, Theis B. Low mortality following resection for pancreatic and periampullary tumours in 1026 patients: UK survey of specialist pancreatic units. UK Pancreatic Cancer Group. Br J Surg 1997; 84:1370-6. [PMID 9361591]
- Balzano G, Zerbi A, Capretti G, Rocchetti S, Capitanio V, Di Carlo V. Effect of hospital volume on outcome of pancreaticoduodenectomy in Italy. Br J Surg 2008; 95:357-62. [PMID 17933001]
- Nathan H, Cameron JL, Choti MA, Schulick RD, Pawlik TM. The volume-outcomes effect in hepato-pancreato-biliary surgery: hospital versus surgeon contributions and specificity of the relationship. J Am Coll Surg 2009; 208:528-38. [PMID 19476786]


