Keywords
APACHE; Multiple Organ Failure; Pancreatitis; Pancreatitis, Acute Necrotizing
Abbreviations
SOFA: Sepsis-related Organ Failure Assessment
INTRODUCTION
Acute pancreatitis is a relatively common illness, with incidence rates varying from 50 to 80 cases per 100,000 people per year in the United States [1, 2]. In 2006, the incidence in Brazil was 15.9 cases per 100.000 people per year and, in the city of São Paulo, it was 19.2 per 100.000 people per year (unpublished original data).
According to the Atlanta Classification, acute pancreatitis should be classified as mild or severe depending on the development of organ failure and/or local complications [3]. The majority of acute pancreatitis cases are of mild manifestation, and they generally resolve themselves spontaneously within a few days, without the need for specific treatment. The severe form of acute pancreatitis is defined by the presence of one or more of the following criteria: a Ranson score equal to, or greater than 3 or an APACHE II score equal to, or greater than 8, failure of one or more systems, such as shock, respiratory insufficiency, renal failure, gastrointestinal bleeding, severe thrombocytopenia and hypokalemia, and local complications, such as necrotizing pancreatitis, abscess formation, or pancreatic pseudocyst [3]. The severe form of the disease, defined in this way, is present in up to 25% of cases, with a mortality rate of 10- 20% [1, 2, 3, 4].
Severe acute pancreatitis has two clinical phases. The first is characterized by SIRS and lasts for the first ten days of the disease. The second phase starts at the end of the second week when infectious complications occur [5, 6]. The first four days are crucial to the evolution of acute pancreatitis, during which 15-25% of patients develop the severe form of the disease [7].
Early identification of these critical patients allows an appropriate intensive treatment plan to be undertaken and reduces the chances of organ failure, thus lowering mortality rates. The two most common methods for evaluating organ failure in acute pancreatitis are the Ranson criteria score [8] and the APACHE II score [9]. The main issues with the Ranson criteria score are the need to wait 48 hours to confirm whether a patient should be considered critically ill and the fact that it does not allow for scores to be reevaluated on a daily basis. The APACHE II is commonly used in intensive care units and permits a daily score to be calculated as needed. However, it also presents problems, such as the complexity of calculating the score, the age factor (i.e., someone with an age of 45 full years gets two more points than someone in the middle of their 45th year of life), and difficulty in distinguishing between necrotizing and interstitial pancreatitis as well as between infected and sterile necrotizing pancreatitis [10]. In addition, APACHE II can overestimate the severity of acute pancreatitis, characterizing as critical some patients who do not actually have organ failure. For this reason, other criteria, such as the Sepsisrelated Organ Failure Assessment (SOFA) [11] and Marshall [12] scores, have been suggested in recent years for evaluating patients with severe acute pancreatitis. The initial determination of necrotizing pancreatitis plays an important role in defining a patient’s risk of infection during the second phase of the disease, and for the prophylactic introduction of antibiotics in those patients with a necrosis of more than 30% [6, 13]. Thus, the rapid identification of patients likely to develop organ failure and necrotizing pancreatitis is fundamental for providing adequate treatment and for improving the prognosis for patients with severe pancreatitis. The aim of this study was to determine which factors are related to the development of systemic complications, mortality and necrotizing pancreatitis in patients with severe acute pancreatitis.
METHODS
Data were collected from 175 consecutive patients with acute pancreatitis who were admitted to the Emergency Unit of the Santa Casa of São Paulo between August 2003 and December 2005. The criterion for inclusion in this analysis was the presence of an APACHE II score greater than eight at admission. The 39 (22.3%) patients with severe acute pancreatitis according to this criterion were included in the analysis. Patients who transferred from other hospitals were excluded.
All patients included underwent computerized tomography (CT) 72 hours after onset. The CT findings were classified according to the Balthazar-Ranson index which assesses edema, fluid collection and necrosis. Patients with necrotizing pancreatitis greater than 30% were given antibiotics (ciprofloxacin and metronidazol) prophylactically for a period of 10 to 14 days [6]. The preferred nutritional support for these patients was enteral through an enteral feeding tube, placed in the first jejunum segment by endoscopy.
The SOFA and Marshall scores were calculated when these patients were admitted. The SOFA score includes the evaluation of six organ systems (pulmonary, hematologic, hepatic, renal, cardiovascular and central nervous system), considering the worst values on each day and a scoring system from 0 (normal) to 4 (most abnormal) [11]. The Marshall score considers three organ systems (pulmonary, cardiovascular and renal) using a scoring system from 0 (normal) to 4 (most abnormal) [12]. Organ failure was defined according to the Atlanta Classification [3].
The variables analyzed were age, sex, acute pancreatitis etiology, hematocrit and leukocyte count at admission, CRP 48 hours after the onset of the disease, Balthazar- Ranson CT index and length of stay. These variables were correlated with the development of systemic complications, mortality, and necrotizing pancreatitis.
ETHICS
This protocol for treating acute pancreatitis was approved by the Committee on Research Ethics of the Surgery Department of the Santa Casa of São Paulo.
STATISTICS
Data are reported as mean±standard deviation (DS) and frequencies. Statistically significant findings were revealed by the application of the Student’s t test and the Fisher’s exact test. A two-tailed P value less than 0.05 was considered significant in all cases. Data were analyzed by means of the SPSS version 16.0 software (SPSS, Inc., Chicago, IL, U.S.A.).
RESULTS
The mean age in the group evaluated was 62.9±14.5 years; 24 of the 39 (61.5%) patients were men. The principal etiology was gallstones in 21 of the patients (53.8%), followed by alcoholism in 13 patients (33.3%). The average length of hospital stay was 10.0±7.8 days.
The patients’ mean APACHE II score was 11.6±3.1, with a mean SOFA score of 3.2±2.0 and a mean Marshall score of 1.5±1.9. Eleven of these patients (28.2%) developed necrotizing pancreatitis, six with necrosis of up to 30%, three with necrosis between 30 and 50% and two with necrosis of more than 50%. The average tomographic index of severity was 3.5±2.9.
Eleven patients (28.2%) developed systemic complications. Pulmonary complications were the most common, present in six patients (15.4%), followed by renal and cardiovascular complications, present in three patients each (7.7%), and three patients (7.7%) had other complications (two had platelets less than 100,000 mm-3 and one had gastrointestinal bleeding); therefore, four patients out of eleven had more than one systemic complication. One patient (2.6%) with necrotizing pancreatitis received surgical treatment because of a worsening clinical situation and died; however, there was no proof of infected necrosis intraoperatively. The mortality rate was 3 out of 39 patients (7.7%). All three of these patients died during their first week of hospitalization as a result of complications related to SIRS followed by pulmonary and renal failure.
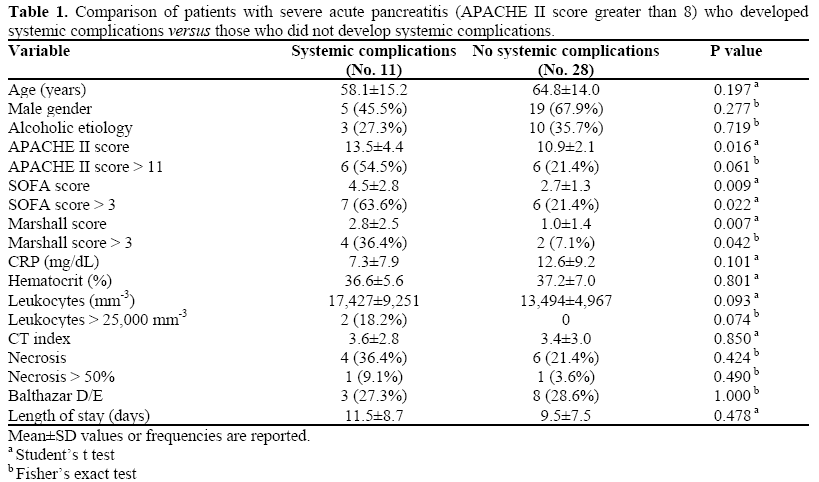
As shown in Table 1, the following variables were found to be significantly related to the development of systemic complications: APACHE II (13.5±4.4 in patients with systemic complications vs. 10.9±2.1 in those without; P=0.016), SOFA score (4.5±2.8 in patients with systemic complications vs. 2.7±1.3 in those without; P=0.009) and Marshall score (2.8±2.5 in patients with systemic complications vs. 1.0±1.4 in those without; P=0.007). Furthermore, a SOFA (P=0.022) or Marshall score (P=0.042) greater than 3 were predictive of development of systemic complications.
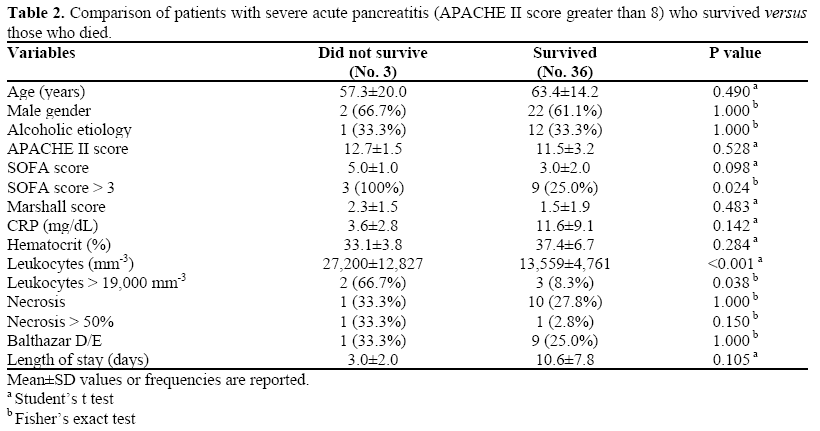
Leukocyte counts were higher in the patients who died (27,200±12,827 mm-3) than in those who survived (13,559±4,761 mm-3; P<0.001). Furthermore, an increased mortality rate was associated with a SOFA score greater than 3 (3/12, 25.0% vs. 0/27, 0%; P=0.024) as well as with leukocytosis greater than 19,000 mm-3 (2/5, 40.0% vs. 1/34, 2.9%; P=0.038) (Table 2).
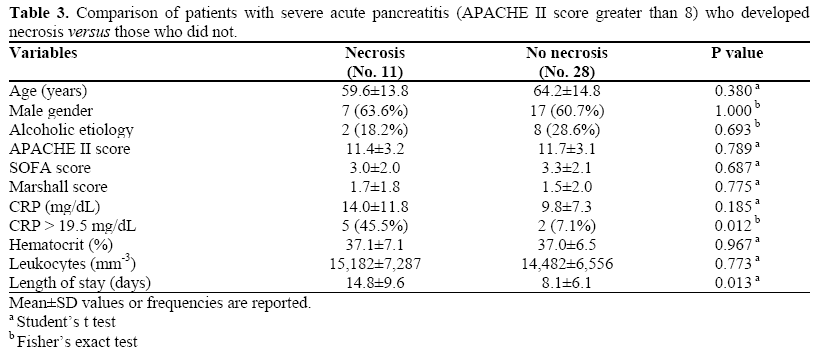
Comparing patients with and without necrosis, there was no relationship between the scoring systems for organ failure and the presence of necrotizing pancreatitis (APACHE II score 11.4±3.2 vs. 11.7±3.1, P=0.789; SOFA score 3.0±2.0 vs. 3.3±2.1, P=0.687; and Marshall score 1.7±1.8 vs. 1.5±2.0, P=0.775) (Table 3). However, necrosis was associated with a CRP greater than 19.5 mg/dL (5/7, 71.4% vs. 6/32, 18.8%; P=0.012) and with a longer hospital stay (14.8±9.6 vs. 8.1±6.1 in non-necrotic cases; P=0.013).
DISCUSSION
In addition to mortality in the second phase of acute pancreatitis caused by infectious complications principally related to the presence of necrosis, early mortality also needs to be considered, despite better care in treating organic dysfunctions in intensive care units [14, 15]. In this study, 3 out of 39 severe acute pancreatitis patients died during the first phase of the disease. Pulmonary complications were the most common and most worrisome problem to occur during the first phase of the disease; they were signaled by the development of acute lung injury and acute respiratory distress syndrome [16, 17]. Close to 70% of acute pancreatitis patients present with some degree of ventilatory dysfunction, and 30% of patients with severe acute pancreatitis develop acute lung injury and acute respiratory distress syndrome [18, 19]. Pulmonary complications were the most frequent in the present study group, affecting 6 out of 39 (15.4%) severe acute pancreatitis patients. New ventilatory strategies for pulmonary protection and specified care in intensive therapy can reduce and control such complications [20].
The use of scoring systems for organ failure aided in the identification of patients with organ failure. These systems are commonly used in intensive care units and have great clinical applicability in acute pancreatitis cases. The APACHE II is the most used system and was proposed in the Atlanta Classification scheme as an alternative to the Ranson criteria score for evaluating patients with acute pancreatitis, especially because it allows for the daily evaluation of patients’ conditions and does not require a 48-hour period for the calculation to be completed. Recently, the idea of temporary organ failure with acute pancreatitis has been gaining ground and, as a result, those systems which can evaluate the condition on a daily basis have been favored, such as the APACHE II, SOFA and Marshall scores, among others. Some authors have stated that organ failure that improves within 48 hours should be classified as temporary organ failure with an improved prognosis and without the need for intensive treatment [10, 21].
Various studies have compared these indicators for organ failure in intensive care units [22, 23, 24] in heterogeneous patient populations, but few studies have evaluated patients with acute pancreatitis. Gocmen et al. evaluated 58 patients with biliary acute pancreatitis and compared their Ranson, APACHE I, APACHE II, APACHE III, SAPS II (simplified acute physiology score) and MPM II (mortality probability model) scores. They concluded that the MPM II had the best performance at admission in predicting mortality among these patients [25].
In this study, we compared APACHE II with SOFA and Marshall scores in patients admitted with severe acute pancreatitis with the goal of predicting systemic complications and mortality. We only looked at patients with an APACHE II score greater than eight because the APACHE II has a tendency to overestimate severe cases; that is, it has a high sensitivity but low specificity when using the cutoff suggested by the Atlanta classification. This is one of the factors that has made the mortality of severe cases appear to be lower in the literature at the same time that the number of cases considered as severe has increased from 10% to 25%. For this reason, we looked at this population defined at admission as severe, with the intent of restricting it, but without omitting any patient whose condition was truly severe. We employed the SOFA and Marshall systems because these are the indicators of organ failure recommended by the Pancreas Club in the revised Atlanta Classification scheme currently being proposed. In addition, SOFA and Marshall scores are easier and simpler to calculate than APACHE II. In determining the development of systemic complications and organ failure, the three methods used in this study were found to be efficient, with a cutoff point greater than three being obtained for both SOFA and Marshall.
With respect to the mortality analysis, this study confronted a problem common to all studies analyzing severe acute pancreatitis: the small number of cases available for statistical analysis. Nevertheless, we found that a SOFA score greater than 3 and leukocytosis greater than 19,000 mm-3 were good criteria for defining the population most at risk of dying. These findings are very useful in clinical practice because they are simple to obtain, and they give us crucial information, that is, which patients are at greater risk of dying
Interestingly, these results showed no relationship between hematocrit levels, and indirectly hemoconcentration, with morbidity or mortality, in contrast with the literature [2, 8, 10].
It is important to consider the limited number of patients in order to obtain a conclusion regarding mortality. However, data relating the SOFA score and leukocytosis with mortality are interesting and should be considered in other studies in the future. We also compared patients who developed necrotizing pancreatitis with those without necrosis, and observed that there was no relationship between the indicators of organ failure evaluated upon admission and the development of necrotizing pancreatitis. In addition, the lack of a relationship between indicator scores for organ failure and for necrotizing pancreatitis confirms the independent course taken by these two complications of acute pancreatitis: SIRS and organ failure in the first phase, and necrotizing pancreatitis with a high risk of infection during the second phase.
The variable associated with the presence of necrosis was a CRP level which exceeded 19.5 mg/dL. This data is similar to that found in the literature, varying only in the cutoff point for necrosis which is usually between 12 and 18 mg/dL [4]. Other markers for pancreatic necrosis and infected necrosis have been used, such as procalcitonin [26]. However, the greater availability and ease of measuring CRP and its ability of diagnosing necrosis and infection make it the preferred marker for acute pancreatitis [4].
Necrosis has an impact on acute pancreatitis disease evolution, especially during the second phase of the disease when infectious complications begin to appear. Despite the fact that there was no statistical significance between necrosis and mortality (because only one patient out of 11 with necrosis died), in a larger series of patients, statistical significance could possibly be achieved. Two patients had necrosis greater than 50%, with 50% mortality.
The data presented here also revealed a significant difference related to a longer hospital stay for patients with necrotizing pancreatitis in comparison to patients without necrosis. This difference can be attributed to better clinical care, such as antibiotics and nutritional support, and surgical care in the event of infected necrosis. These data support the importance of the length of the hospital stay when considering the analysis of local complications in acute pancreatitis.
There are clearly problems in classifying patients with acute pancreatitis, especially using only an APACHE II score greater than eight, and this was the starting point of this paper. However, we can find distinguished papers in the literature which, for the most part, used this criterion to stratify patients with acute pancreatitis. Our aim in this study was to add other tools for determining which patient is really severe, starting with a cutoff of APACHE II greater than eight.
Our findings lead us to suggest that an initial triage with APACHE II should be undertaken; if the score obtained exceeds eight, the SOFA score should be calculated. The population at greatest risk of developing systemic complications and of dying can then be identified as those patients with a SOFA score greater than three and leukocytosis greater than 19,000 mm-3
In our study, 20 of the 39 patients with an APACHE II score greater than eight had a SOFA score greater than three, thus reducing the number of “severe” patients from 22.3 to 6.9%, and increasing the mortality rate of “severe” patients from 7.7 to 25%. In this way, we were able to identify the population of patients whose conditions were truly severe without omitting patients who died during the first phase of the disease. At the same time, levels of CRP play an important role in diagnosing necrotizing pancreatitis; when elevated, CRP levels indicate the need for a CT to confirm necrosis. If the amount of necrosis involves more than 30% of the pancreas, we believe that the early use of antibiotics can be beneficial in reducing infectious complications [6].
Undoubtedly, a limitation of this study is the number of patients analyzed (n=39). Thus, a statistical analysis with a small sample size should be evaluated cautiously, especially as regards mortality (n=3). Multicentric studies with a larger number of patients are still needed in order to come to a definitive conclusion about these criteria and their cutoff points. However, indicators such as the SOFA score, leukocytosis and CRP should be considered in future studies regarding severe acute pancreatitis.
CONCLUSIONS
This study demonstrates that, in patients with acute pancreatitis and an APACHE II score greater than eight, indicators of organ failure correlate with the development of systemic complications and with mortality, with SOFA being the best of these indicators in this population. The variable which bears a strong relationship to the development of necrotizing pancreatitis is CRP. No evidence of a relationship between scoring systems for organ failure and the presence of necrosis in cases of severe acute pancreatitis was found.
Conflict of interest
The authors have no potential conflicts of interest
References
- Clancy TE, Benoit EP, Ashley SW. Current Management of Acute Pancreatitis. J Gastrointest Surg 2005; 9:440-52. [PMID 15749609]
- Toouli J, Brooke-Smith M, Bassi C, Carr-Locke D, Telford J, Freeny P, et al. Guidelines for the management of acute pancreatitis. J Gastroenterol Hepatol 2002; 17 Suppl:S15-39. [PMID 12000591]
- Bradley EL 3rd. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993; 128:586-90. [PMID 8489394]
- Werner J, Hartwig W, Uhl W, Muller C, Buchler MW. Useful markers for predicting severity and monitoring progression of acute pancreatitis. Pancreatology 2003; 3:115-27. [PMID 12748420]
- Werner J, Feuerbach S, Uhl W, Büchler MW. Management of acute pancreatitis: from surgery to interventional intensive care. Gut 2005; 54:426-36. [PMID 15710995]
- De Campos T, Assef JC, Rasslan S. Questions about the use of antibiotics in acute pancreatitis. World J Emerg Surg 2006; 1:20. [PMID 16820058]
- Beger HG, Rau BM. New advances in pancreatic surgery. CurrOpinGastroenterol 2007; 23:522-34. [PMID 17762558]
- Ranson JH, Rifkind KM, Roses DF, Fink SD, Eng K, Localio SA. Objective early identification of severe acute pancreatitis. Am J Gastroenterol 1974; 61:443- 51. [PMID 4835417]
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985; 13:818-29. [PMID 3928249]
- Banks PA, Freeman ML, Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379-400. [PMID 17032204]
- Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (Sepsisrelated Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996; 22:707-10. [PMID 8844239]
- Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med 1995; 23:1638-52. [PMID 7587228]
- Villatoro E, Bassi C, Larvin M. Antibiotic therapy for prophylaxis against infection of pancreatic necrosis in acute pancreatitis. Cochrane Database Syst Rev 2006; 18:CD002941. [PMID 17054156]
- McKay CJ, Evans S, Sinclair M, Carter CR, Imrie CW. High early mortality rate from acute pancreatitis in Scotland, 1984-1995. Br J Surg 1999; 86:1302-5. [PMID 10540138]
- McKay CJ, Imrie CW. The continuing challenge of early mortality in acute pancreatitis. Br J Surg 2004; 91:1243-4. [PMID 15382103]
- De Campos T, Deree J, Coimbra R. From acute pancreatitis to end-organ injury: mechanisms of acute lung injury. Surg Infect 2007; 8:107-20. [PMID 17381402]
- Muhs BE, Patel S, Yee H, Marcus S, Shamamian P. Inhibition of matrix metalloproteinases reduces local and distant organ injury following experimental acute pancreatitis. J Surg Res 2003; 109:110-7. [PMID 12643851]
- Jacobs ML, Daggett WM, Civette JM, Vasu MA, Lawson DW, Warshaw AL, et al. Acute pancreatitis: analysis of factors influencing survival. Ann Surg 1977; 185:43-51. [PMID 831635]
- Shields CJ, Winter DC, Redmond HP. Lung injury in acute pancreatitis: mechanisms, prevention, and therapy. Curr Opin Crit Care 2002; 8:158-63. [PMID 12386518]
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301-8. [PMID 10793162]
- Gurusamy KS, Farouk M, Tweedie JH. UK guidelines for management of acute pancreatitis: is it time to change? Gut 2005; 54:1344-5. [PMID 16099804]
- Livingston BM, MacKirdy FN, Howie JC, Jones R, Norrie JD. Assessment of the performance of five intensive care scoring models within a large Scottish database. Crit Care Med 2000; 28:1820-7. [PMID 10890627]
- Katsaragakis S, Papadimitropoulos K, Antonakis P, Strergiopoulos S, Konstadoulakis MM, Androulakis G. Comparison of Acute Physiology and Chronic Health Evaluation II (APACHE II) and Simplified Acute Physiology Score II (SAPS II) scoring systems in a single Greek intensive care unit. Crit Care Med 2000; 28:426-32. [PMID 10708178]
- Arabi Y, Haddad S, Goraj R, Al-Shimemeri A, Al- Malik S. Assessment of performance of four mortality prediction systems in a Saudi Arabian intensive care unit. Crit Care 2002; 6:166-74. [PMID 11983044]
- Göçmen E, Klc YA, Yolda? O, Ertan T, Karaköse N, Koç M, Tez M. Comparison and validation of scoring systems in a cohort of patients treated for biliary acute pancreatitis. Pancreas 2007; 34:66-9. [PMID 17198185]
- Rau BM, Kemppainen EA, Gumbs AA, Buchler MW, Wegscheider K, Bassi C, et al. Early assessment of pancreatic infections and overall prognosis in severe acute pancreatitis by procalcitonin (PCT): a prospective international multicenter study. Ann Surg 2007; 245:745-54. [PMID 17457167]

