Keywords
Blind Loop Syndrome; Enteritis; Pancreatitis, Chronic; Digestion; Enzymes; Absorption
INTRODUCTION
Chronic pancreatitis is a multiple etiological disease characterized in major cases by progressive course with the development of exocrine and endocrine insufficiency of the pancreas [1, 2, 3].
In patients with exocrine insufficiency of pancreas as a result of chronic pancreatitis in some cases enzyme replacement therapy happens to be inefficient [4, 5, 6, 7]. Possible reasons may include inadequate dose of enzyme preparation, use after expiry date, great amount of fat in patient’s everyday meals, absence of compliance, or wrong diagnosis (for example, a case when a patient with celiac disease is diagnosed as a chronic pancreatitis patient) [8, 9]. The other reasons of malabsorption, concerning tropical countries especially, should be taken into account as well: infections of small intestine, protozoal, helminth infections, intestinal tuberculosis, inflammatory bowel diseases, celiac disease, immune deficiency, etc. [10]. One of the most frequent reasons for limited efficiency of enzyme preparations in chronic pancreatitis is combination of maldigestion resulting from pancreatic insufficiency and malabsorption resulting from secondary enteritis with the bacterial overgrowth syndrome in a small intestine. Bacterial overgrowth syndrome leads to acidification of duodenal contents and then to pancreatic enzymes inactivation [6, 7, 8, 11, 12, 13]. Bacterial overgrowth syndrome is associated with the disorders of small intestinal motility, frequently found to develop in acute pancreatitis and chronic pancreatitis. Duodenal motility is associated with glucose absorption. Propagated duodenal pressure wave sequences are proved to be positively related to glucose absorption [14]. These associations should be also taken into consideration in chronic pancreatitis therapy.
There exist other reasons for bacterial overgrowth syndrome in chronic pancreatitis, for instance combination of chronic pancreatitis with the small intestinal diverticulosis. In such cases, severe malabsorption is observed to develop [15, 16].
Secondary enteritis in chronic pancreatitis results from duodenal stasis, decrease of bactericidal property of duodenal contents and accompanying of bacterial overgrowth syndrome. Atrophy of small intestine mucosa gradually progresses causing malabsorption [11]. Another reason for bacterial overgrowth syndrome is long term administration of antibiotics in case of acute pancreatitis (including the recurrent one) often converted into chronic pancreatitis [17].
Pancreatic insufficiency and secondary enteritis also encourage a flow of a greater amount of bacterial allergens and toxins including specific lipopolysaccharide of Gram-negative intestinal flora from the bowel to the blood circulation.
Despite pathogenic and clinical significance of the above described mechanisms, the small intestine in chronic pancreatitis has not been investigated thoroughly. It would be important to understand fat metabolism in the course of this disease and this could be explained if the small intestine have some pathological conditions (for example bacterial overgrowth syndrome, secondary enteritis) and, due to this condition, pancreatic enzyme substitution does not work in all patients.
Aim of the Study
To investigate the pathophysiology of the small intestine in chronic pancreatitis and to show the reason why in some cases pancreatic enzyme substitution does not work properly.
MATERIALS AND METHODS
We have examined 33 patients with chronic pancreatitis including 27 (81.8±9.5%) males and 6 (18.2±8.2%) females with age ranging from 17 to 61 years (42.1±1.9 years; less than, or equal to, 25 years: 1 patient, 3.0±0.1%; 26-50 years: 30 patients, 90.9±0.3%; over 50 years: 2 patients, 6.1±0.2%); 23 (69.7±8.5%) were alcohol drinkers. Chronic pancreatitis was diagnosed in all the patients according to M-ANNHEIM criteria [18]. It means the patients had typical clinical history of chronic pancreatitis and one or more of the following additional criteria: pancreatic calcifications, moderate or marked ductal lesions (according to the Cambridge classification), marked and persistent exocrine insufficiency (defined as a pancreatic steatorrhea markedly reduced by enzyme supplementation), and typical histology of an adequate histological specimen [18]. M-ANNHEIM severity index in our patients was the following: А (minor severity level): 5 (15.2±1.2%); B: 12 (36.4±1.7%); C: 11 (33.3±1.6%): D: 4 (12.1±1.2%); E: 1 (3.0±0.9%). The course of disease was: less than 1 year: 5 patients, 15.2±1.8%; from 2 to 5 years: 13 patients, 39.4±2.1%; from 6 to 10 years: 11 patients, 33.3±2.0%; over 10 years: 4 patients, 12.1±1.3%. The examined patients with chronic pancreatitis have not clinical manifestations of small intestine involvement to the process.
According to the results of fecal elastase 1 test by immunoenzymatic method (kit: Schebo, Giessen, Germany; immunoenzyme analyzer: Sanofi, Paris, France) 22 (66.7±8.2%) patients had severe and 11 (33.3±8.2%) patients had moderate or mild pancreatic insufficiency. We investigated random stool samples in patients with watery diarrhea; these samples were lyophilized.
The control group includes 30 subjects without chronic pancreatitis similar for age (44.3±1.5 years; P=0.373), sex (25 males, 83.3±9.1%; 5 females, 16.7±8.1%; P=0.909) and alcohol consumption (20, 66.7±8.2%; P=0.800) to the patients with chronic pancreatitis patients.
Aspiration biopsy of the small intestine mucosa was performed in the morning pre-prandial (after 12-14 hours of fasting) 15-20 cm behind duodenojejunal ligament by means of a Masevich design probe, suggested for aspiration biopsy of stomach mucous membrane [19], but longer in length (to 150 cm). Probe capsule position before biopsy was monitored by Xray.
Immediately after taking off the probe the biopsied sample of jejunum mucosa was divided into parts (6-8 mg weight each), one of them was used for histological examination, all the rest was used for the study of enzymatic activity and metabolism at enterocytic level. We investigated just a single mucosa sample, considering the complexity of obtaining biopsy material from the jejunum mucosa. even if we realize that this may represent a limitation of the study. To study general structure of jejunum mucosa its samples were stained with hematoxylin and eosin. Detection of connective tissue and muscle fibers was carried out by samples staining with regard to Van Gison method, i.e. neutral mucopolysaccharides with regard to PASreaction [20].
To ensure validity of the results in the process of light microscopy of histological samples besides descriptive characteristics we also measured the following parameters by means of ocular micrometer and we have calculate mean values (in microns) for main structures of jejunum mucous membrane: height and breadth of villi, depth of crypts, thickness of proper layer, height of epithelium (middle third of villi). The mitotic index (the mean number of mitosis per one crypt), the index of leukopedesis in villi epithelium (the mean value of ratio between the number of leukocytes in epithelial cells and the number of the latter), the contents of goblet cells in epithelial villi tegument (in percent) and the number of neutrophils in the cellular infiltrate of jejunum mucosa proper layer (in percentage) were also calculated.
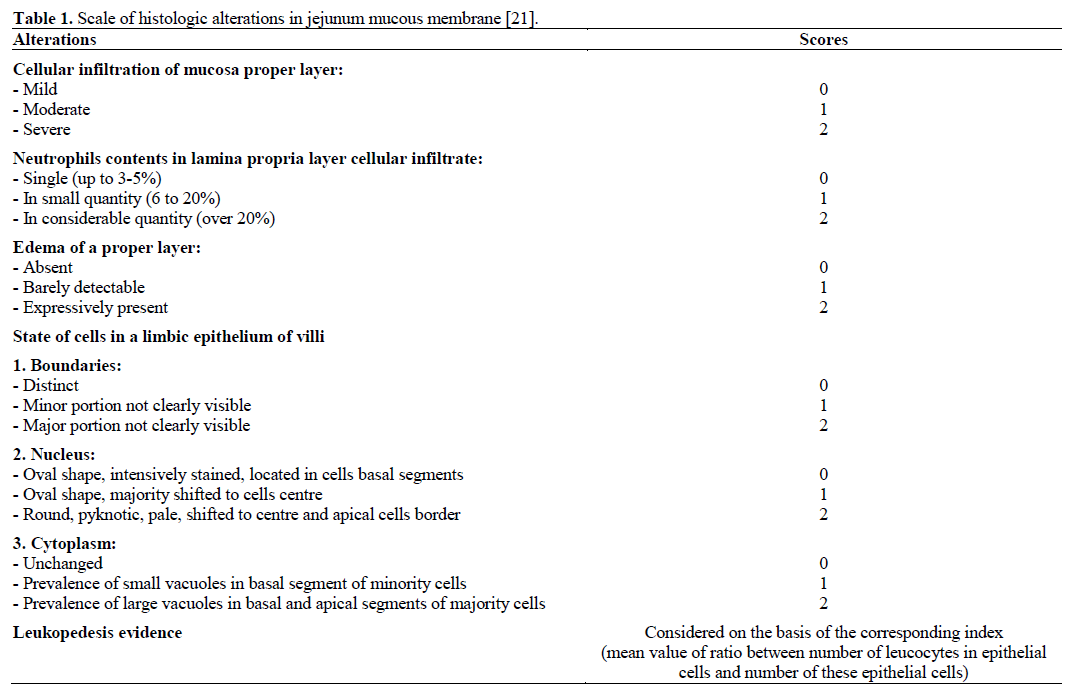
To characterize presence and evidence of jejunum mucosa atrophy height of villi was considered as the main point. We used a previously validated score (Table 1) [21] in order to evaluate evidence of inflammatory dystrophic changes in the mucosa. In order to estimate the evidence of inflammatory dystrophic changes in jejunum mucous membrane, we summed up the scores according to the above figure (Table 1). This overall index was used as morphological criterion of presence and evidence of chronic enteritis exacerbation [22]. At that we discriminated: 1) the mucosa of jejunum without pathohistological changes; and 2) chronic jejunitis stratified according two different criteria: i) the height of jejunum villi into types (without atrophy (>339 mm); with I degree atrophy (339-226 mm); with II degree atrophy (225-110 mm)); ii) the manifestations of inflammatory dystrophic changes into stages (phases) (no signs of exacerbation (score <1); mild exacerbation (scores 1-5); moderate exacerbation (scores 5-10); severe exacerbation (score >10) [22].
State of metabolism in enterocytes has been studied according to enzymatic activity of amylase and lipase enzmye activity in small intestine. Production of the most significant digestive enzymes (monoglyceride lipase, lactase, saccharase, maltase, glycyl-l-leucine dipeptidase) providing metabolism in enterocytes has been considered as for their activity in homogenates of biopsied jejunum mucosa. Participation of mucosa in intestinal digestion has been evaluated by alkaline phosphatase activity in secretion from proximal portion of jejunum.
Enzymatic activity of amylase has been determined by means of Ugolev method [23]. Enzymatic activity of lipase (providing early stages of triglycerides hydrolysis) was measured on the basis of a modified Ugolev and Nurks stalagmometric method [24]. Under consideration there were also rates reflecting absorptive capacity of small intestine and amylase and lipase activity in the sphere of parietal digestion in comparison with its activity in the cavity of small intestine. Monoglyceride lipase activity (providing final stages of triglyceride hydrolysis) has been measured on the basis of research technique described by Ugolev and Chernyakchovskaya [25]. Lactase and maltase activity of small intestine mucosa has been calculated according to Dahlgvist et al. [26] on the basis of our own modification [27]. Sacharase activity of small intestine mucosa was assessed on the basis of the Ugolev and Yezuitova technique [28] and dipeptidase activity of mucous membrane was assessed on the basis of the Ugolev and Timofeeva technique [29]. To study activity of alkaline phosphatase in secretion from initial portions of jejunum we used the technique suggested by Fomina et al. [30]. Lysosime activity in jejunal chyme was assessed by turbodimetric method [31].
To estimate the condition of jejunum mucosa we examined the contents of cellular elements in jejunal chyme detecting DNA in it. This test was performed by means of calorimetric method according to Barton [32]. The study of absorptive function of small intestine was performed on the basis of an updated Dxylose test [33]. To study intestinal enzyme activity and absorption we were forced to apply rather obsolete tools as standard kits were unavailable.
The inoculation of a different nutrient media (EndoTM, SaburoTM, PloskirevTM from Optimum, Lviv, Ukraine; bactagar, blood and salt agar) was made in order to study microbic flora in jejunal chyme, followed by the selection of pure cultures with the aim of identification and count of microbic bodies per 1 mL of jejuna chyme.
Levels of IgG, IgA, and IgM were evaluated by automatized method by using a biochemical analyzer (Kone, Espoo, Finland) [34]. Secretory IgA level in duodenal contents was studied using antiserum from Biomed (Moscow, Russia) by radial immunodiffusion method [35].
ETHICS
Written informed consent was obtained from each patient and the study protocol conforms to the ethical guidelines of the “World Medical Association (WMA) Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008, as reflected in a priori approval by the appropriate institutional review committee.
STATISTICS
Data are reported as mean and standard error (SE). Relative frequencies were reported as percentages and their SEs were also calculated [36]. The statistical analysis was performed by using the Student-t tests. The null hypothesis was rejected when two-tailed P values were less than 0.05. Data were analyzed by means of the software package Statistica 6.0 (Statsoft, Tusla, OK, USA).
RESULTS
Characteristics of Morphological State of Jejunum Mucosa in Chronic Pancreatitis Patients
Minor part of jejunum villi was slightly deformed (cone-shaped, club-shaped, fusiform, etc.). We failed to detect meaningful changes (P=0.075) in their height between patients with chronic pancreatitis (383.3±7.4 μm) and controls (404.6±13.3 μm). However, width of villi (125.4±5.4 μm vs. 112.6±3.4 μm) was considerably increased (P<0.001). Height of limbic villi epithelium (33.8±0.5 μm vs. 36.0±0.3 μm) was considerably decreased (P=0.004). Manifested signs of dystrophic changes were found (30 cases; 90.9±5.0%) those being mostly evident (boundaries inconspicuous, nucleus shape irregular, pale color, shifted to center and apical border, in basal and apical segments of cells large vacuoles prevailed). In major cases locally thinned brush edges (26 cases; 78.8±7.1%) and fuzzy basal membrane (27 cases; 81.8±6.7%) were noticed. Leukopedesis of villi epithelial tegument (ratio: 0.66±0.03) as well as a quantity of goblet cells in it (11.3±0.6%) was found to be reliably growing (P=0.001 vs. 6.7±0.4%). Most crypts had a regular shape showing no significant depth changes (140.4±5.1 μm vs. 132.0±5.2 μm; P=0.148). The quantity of Paneth cells in crypts (2.1±0.3 vs. 1.2±0.3) was considerable increased (P=0.031) while their mitotic index (1.6±0.2 vs. 2.8±0.2) was considerably decreased (P=0.001).
Thickness of jejunum mucosa propria layer (152.9±5.0 μm vs. 146.6±4.1 μm) did not undergo significant changes (P=0.198). This layer was characterized by evident or mild infiltration mostly with lymphoid and plasma cells with a small amount of eosinophils; a half of patients were having excessive amount of neutrophils. Fourteen patients (42.4±8.6%) had edema in jejunum mucosa mostly with barely detectable patients; 63.6±8.4%) there was found a sclerosis of jejunum mucosa proved by presence of collagen fibers either in small part (24 cases; 72.7±7.8%) or considerable quantity in rare cases (9 cases; 27.3±7.8%). The sum of scores (5.6±0.4), reflecting evidence of inflammatory dystrophic changes in mucous membrane, was significantly higher than in controls (0.49±0.06; P=0.001).
Illustrations of morphological picture of jejunum mucous membrane in one subject from the control group and in one chronic pancreatitis patient are represented in Figures 1 and 2.
Figure 1. Normal mucosa of jejunum in one patient of the control
group (staining by hematoxylin and eosin; magnification x40).
Figure 2. Chronic jejunitis without atrophy with manifested
exacerbation in chronic pancreatitis patient. Mild dystrophy of
jejunum villi epithelium. Lamina propria layer of mucous membrane
demonstrates evident cellular infiltration mostly in crypts area
(staining by hematoxylin and eosin; magnification x40).
Thus, in chronic pancreatitis patients having no clear clinical manifestations of the small intestine involvement into the process the alterations detected conformed chronic jejunitis without atrophy at the stage of mild or moderate exacerbation.
Enzymatic Indices of Jejunum Digestive Function in Patients with Chronic Pancreatitis
Examined patients were found to have an increase in enzymatic activity of amylase in jejunum (Table 2). They showed increase of activity indices both in the sphere of enterocytes and intestinal digestion. Index of amylase activity ratio in enterocytes and intestinal digestion in chronic pancreatitis patients did not undergo considerable changes (P=0.215). Increase in enzymatic activity of amylase in enterocytes was stipulated by increment of absorbed and enterocyteconnected amylase.
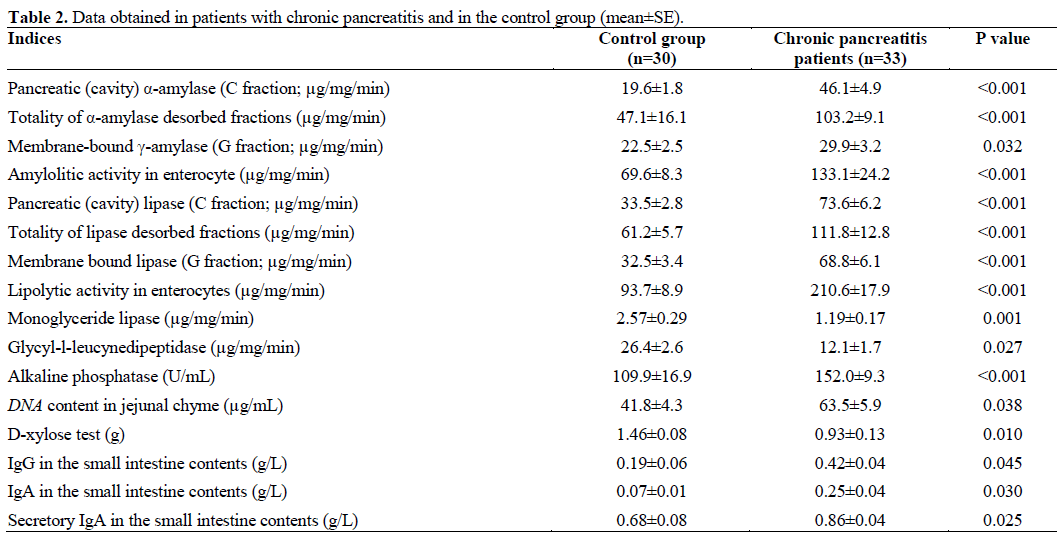
Chronic pancreatitis was characterized by the same changes in jejunum lipolytic activity (Table 2). Statistically reliable was the growth of jejunum lipase activity in the area of membrane and intestinal digestion. Increment of jejunum lipolytic activity in enterocyte can be explained by statistically increment of absorptive and membrane-connected lipase activity.
We did not observe considerable changes in indices of absorption capacity of jejunum mucous membrane to amylase and lipase and ratio of enzymatic activity of lipase and enzymatic activity of amylase in the sphere of membrane and intestinal digestion.
In chronic pancreatitis it has been revealed a decrease of monoglyceride lipase activity in jejunum mucosa providing final stages of triglyceride hydrolysis. Glycyl-l-leucine-dipeptidase production of jejunum in chronic pancreatitis patients was considerably decreased while alkaline phosphatase content in jejunal chyme was significantly increased in comparison with the controls (Table 2).
DNA content in a jejunal chyme in chronic pancreatitis patients was considerably increased and, according to the D-xylose test, the absorptive function of small intestine in chronic pancreatitis patients was considerably decreased (Table 2).
Lactase production in jejunum in chronic pancreatitis patients was not considerably decreased (1.79±0.31 μg/mg/min vs. 2.66±0.30 μg/mg/min; P=0.235). We also failed to observe a substantial impairment in saccharase production in jejunum of chronic pancreatitis patients (11.7±1.3 μg/mg/min vs. 9.9±0.9 μg/mg/min; P=0.120). It has not also been revealed a considerable change of maltase function of jejunum in chronic pancreatitis patients (6.6±0.9 μg/mg/min vs. 6.1±0.8 μg/mg/min; P=0.180). Study of lysoszyme in jejunal chyme in chronic pancreatitis has not shown its considerable decrease (1.6±0.2 μg/mL vs. 2.60±0.45 μg/mL; P=0.312).
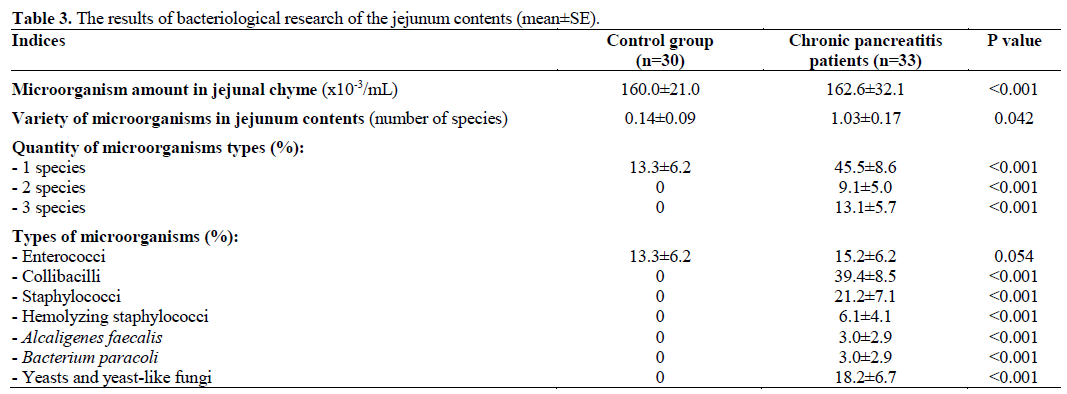
In chronic pancreatitis patients microbial flora in jejunum contents was found considerably (P<0.001) more frequent (67.7±8.2%) than in the controls (13.3±6.2%). In detail the results of bacteriological profile of the jejunum contents are shown in Table 3. The patients had not specific clinical signs of the small intestine involvement, so we could not estimate clinical difference in chronic pancreatitis patients with bacterial overgrowth syndrome and those without it.
Significantly marked increases of IgG and IgA levels in the small intestine contents was found in chronic pancreatitis patients when compared with controls, as well as, there was a significant difference in the secretory IgA contents between chronic pancreatitis patients and control group (Table 2).
DISCUSSION
Our study has demonstrated that chronic pancreatitis patients are characterized by changes in jejunum mucosa similarly with chronic jejunitis, mainly with no atrophy, at the stage of mild or evident exacerbation. Absence of clinical manifestations of small intestine impairment in this case is probably related to the fact that just limited portions of small intestine are involved or it is eclipsed by more vivid clinical manifestation of chronic pancreatitis.
We managed to reveal increase of enzymatic activity of amylase and lipase in the sphere of membrane and intestinal digestion, increase of alkaline phosphatase activity being the evidence of latent jejunitis. This enzyme activity rise is probably a result of compensatory tension in intestinal digestion in patients suffering from exocrine insufficiency of pancreas. On the other hand, it may occur due to stimulation of intestinal enzyme production with insufficiently hydrolyzed chyme components.
Production of saccharase and maltase by jejunum did not undergo vital changes. At the same time, lactase glycyl-l-leucine-dipeptidase activity in chronic pancreatitis was markedly decreased possibly being the reflection of primary atrophic processes in small intestine mucosa.
Increase of DNA amount in jejuna chyme is the evidence of hyperdesquamation of epithelium and reflection of mucous inflammation.
Decrease of D-xylose test index also contributes to existence of enteritis in chronic pancreatitis patients and it proves the development of malabsorption in such patients. In contrast to us, Lembcke et al. did not detect high incidence of lactase deficiency or D-xylose malabsorption in chronic pancreatitis patients [7].
We were deprived of technical resource to study the frequency of vitamin B12 deficiency in chronic pancreatitis patients, though it would have been of great significance and interest. Literature data regarding this topic are quite contradictory. Lembcke et al. failed to detect a high incidence of vitamin B12 depletion in chronic pancreatitis [7]. On the contrary, Wagner et al., detected an increased frequency of vitamin B12 deficiency in patients with chronic pancreatitis and bacterial overgrowth syndrome [37]. It should be pointed out that the first of the above mentioned authors studied the level of vitamin B12 in blood, while the second one carried out a 13C breath test.
Decrease of lysozyme level in jejunum chime was not statistical significant but correlates with the growth of microorganisms amount and variety of their types in jejunum. Obviously, lack of bactericidal properties of intestinal contents both due to drop in pancreatic enzymes activity and reduction of lysozyme amount in a lumen leads to bacterial overgrowth syndrome. It may also be contributed by lack of secretory IgA production in the small intestine. We can suppose penetration of serological IgG and IgA into intestinal cavity to provide antibodies-antigens contact may be just the result of bacterial overgrowth syndrome itself and does not impact probability of its development and evidence.
The data obtained by us truly proof concerning the development of secondary enteritis in chronic pancreatitis. At that, typical morphologic changes of jejunum mucous membrane, desquamation of epithelium, decrease in local immunity, bacterial overgrowth syndrome formation, alterations in membrane and intestinal digestion are often observed to occur. A substantial consequence of enteritis is a reduction of absorption in the small intestine, i.e. malabsorption. Our findings explain lack of efficacy of enzyme replacement therapy in some patients with chronic pancreatitis.
Data published in literature concerning mucous membrane morphology, enzymatic and absorptive activity of small intestine, and results of bacteriological examination in chronic pancreatitis are rather limited.
Danovskiy [38] detected chronic jejunitis of various intensity in histological studies of jejunum mucosa biopsy material of such patients. These authors did not carry out a semi-quantitative estimation of histological alterations, but they studied just enzymatic activity of lipase and amylase in the jejunum. The data obtained by these authors are different from our results. They revealed a decreased enzymatic activity in the sphere of intestinal digestion of jejunum in some chronic pancreatitis patients, while in others (patients with severe chronic pancreatitis) the decrease was accompanied by a sharp fall of activity in the sphere of membrane hydrolysis, primarily due to tenacious fractions and hardly desorbing amylase.
Archiy et al. [39] also observed (but, in this case, in the duodenum and just in a small number of chronic pancreatitis patients) a decrease of amylase activity in the sphere of enterocyte, especially due to tenacious fractions. Amylase activity in the sphere of intestinal digestion more often increased and rarely decreased. By means of carbohydrate loading the same authors revealed impairment in saccharase hydrolysis in majority of chronic pancreatitis patients [39].
Thus, the data of amylase and lipase activity of the jejunum obtained by various authors are rather contradictory. Strokova [40, 41] also found dystrophic changes in enterocytes in duodenum (but not jejunum) biopsy material, as well as, in case of alcoholic etiology of chronic pancreatitis, atrophic changes and impairment of limbus were also detected. This author revealed a decrease of saccharase, γ-amylase, and alanine-aminotransferase activity in biopsy material of duodenum mucosa in patients with biliary chronic pancreatitis, while deficiency of dipeptidases activity (alanine-aminopeptidase, maltase, saccharase, and amylase activity) in a intestinal digestion and membrane digestion was detected in patients with alcoholic chronic pancreatitis. A decrease of protein contents in duodenum mucosa biopsy material was observed both in patients with alcohol-related and biliary chronic pancreatitis.
We have earlier published the data on decrease of monoglyceride-lipase [42], glycyl-l-leucine-dipeptidase [43] and lactase activity in jejunum mucosa biopsy material [44], as well as absence of changes in maltase and saccharase activity in chronic pancreatitis patients [45]. It means that our data do not completely coincide with those obtained by Strokova [40, 41], perhaps due to the fact that we studied enzymatic activity of jejunum while Strokova examined activity of duodenum. Besides, Strokova compared the data of chronic pancreatitis patients with the data of healthy volunteers; this means that alterations found in such patients are rather related to alcohol abuse but not with chronic pancreatitis.
There have not been available any previous reports on lipase activity in small intestine providing final stages of triglyceride hydrolysis, production by small intestine of other enzymes involved into membrane digestion (peptidase, lactase, maltase, saccharase, etc.). It is also true concerning enzyme excretory activity of small intestine in chronic pancreatitis. We failed to find in the existing literature data regarding alkaline phosphatase activity in small intestine cavity other than our own data [46, 47, 48, 49].
Available data on a condition of absorptive function of small intestine in chronic pancreatitis patients seem to be rather contradictory. Vasilenko and Vinogradova [50], as well as Ishmuchametova [51], failed to reveal any impairment in resorption of labeled oleic acid. At the same time Trusov et al. [52] in some chronic pancreatitis patients, and Chey et al. [53] observed impaired resorption in intestine according to test with oleic acid marked with 131I. Balcerzak et al. [54] failed to find impairment of iron absorption in small intestine in chronic pancreatitis patients.
Study of resorptive function of small intestine by means of D-xylose test was carried out by us only [55]. We failed to find in literature data regarding the contents of lysozyme in jejunal chyme of chronic pancreatitis patients. But our data conform with the results of Lembcke et al. regarding considerable frequency of bacterial overgrowth syndrome in chronic pancreatitis [7]. These authors diagnosed bacterial overgrowth syndrome in 40% of chronic pancreatitis patients on the bases of 14 C-cholylglycine breath test. Therefore, occasionally this condition was associated with diarrhea and steatorrhea [7]. Lembcke et al. resolved that steatorrhea remaining after high-dosage pancreatin supplementation might sometimes be due to bacterial overgrowth syndrome [7]. Grigoreva et al. established that bacterial overgrowth in the small intestine is noted in the majority of patients with chronic pancreatitis. They found an association between clinical manifestations of chronic pancreatitis, active duodenitis, duodenal lymphangiectasia and papillitis and bacterial overgrowth syndrome in small intestine [56]. But these authors studied duodenal mucosa (not a jejunal one); therefore, they did not studied bacterial spectrum in the jejunum. Probably, this contributes to the fact that the authors revealed the association between clinical manifestations of chronic pancreatitis and bacterial overgrowth syndrome, while we failed to reveal such an association.
Mancilla et al. subjected chronic pancreatitis patients to a hydrogen breath test with lactulose and diagnosed bacterial overgrowth syndrome in 92% of patients but just in 7% of control persons (P<0.001) [6]. An unique patient with chronic pancreatitis without bacterial overgrowth syndrome was diagnosed; this patient had minimal morphologic alterations in computed tomography and endoscopic pancreatography [6]. It was concluded that bacterial overgrowth syndrome is common in chronic pancreatitis and may be responsible for persistent symptoms. Proper diagnosis and treatment could alleviate symptoms and improve quality of life [6]. We agree with this conclusion and the difference in bacterial overgrowth syndrome frequency according to Mancilla et al. versus our data is probably due to the fact that we used a direct method to diagnose bacterial overgrowth syndrome while Mancilla et al. used an indirect one, that may lead to hyperdiagnostics.
Trespi and Ferrieri used hydrogen breath test to diagnose bacterial overgrowth syndrome in chronic pancreatitis patients as well, but they used glucose instead of lactulose [13]. Bacterial overgrowth syndrome has been detected in 34% of chronic pancreatitis patients and in 21% of gastro-resected patients without pancreatic disease. In chronic pancreatitis patients bacterial overgrowth syndrome was most likely to be present in case of a high-ethanol intake, pancreatic microcalcifications, concomitant gallstones, diarrhea and a history of gastric resection. To improve the results of the replacement therapy the authors decided to use rifaximin, a nonabsorbed nonsystemic antibiotic with a broad spectrum of antibacterial action covering Gram-positive and Gramnegative organisms, both aerobes and anaerobes. Therefore, this antibiotic has little value outside the enteric area and this minimizes both antimicrobial resistance and systemic adverse events [57]. Trespi and Ferrieri prescribed rifaximin 400 mg t.i.d. for seven consecutive days each month for three months. Rifaximin administration normalized the hydrogen breath test results and reduced symptoms in all patients with bacterial overgrowth syndrome [13]. These results confirm the crucial importance of syndrome of bacterial overgrowth as a factor which decreases the replacement therapy efficacy in case of chronic pancreatitis [13].
On the contrary, Madsen et al. reported data suggesting that bacterial overgrowth syndrome is not of great significance as a cause for non-efficacy of enzymatic preparations in chronic pancreatitis. Bile acid absorption and small intestinal permeability might be affected in patients with exocrine pancreatic insufficiency who receive treatment with enzyme supplementation [58].
Bode and Bode believe that only alcohol abuse even without chronic pancreatitis in a patient may lead to malabsorption [59]. Alcohol abuse interferes with the absorption of glucose, aminoacids, lipids, water, sodium and vitamins (especially thiamine and folic acid) in the small intestine. This inhibition of absorption of nutrients may contribute to nutritional deficiencies frequently observed in alcoholics. Chronic alcohol abuse increases markedly the prevalence of bacterial overgrowth in the small intestine [59]. Bacterial overgrowth syndrome may become the reason of occult malabsorption in the elderly without pancreatic disease. Just meticulous differential diagnostics in such cases may become the basis for the unreasonability of administration and motivation for non-efficacy of enzymatic preparations [16].
Little is known about local immunity status in chronic pancreatitis. It may be related to problems arising from pancreas biopsy as well as probably to proteolysis of immunoglobulins by enzymes in the examined intestinal contents. The data on capacity of pancreas to synthesize immunoglobulins are of great importance [60]. The information on immunoglobulin levels in pancreatic juice is extremely contradictory, it varies from the idea of complete absence of secretory IgA [61] in this juice to the suggestion of using this index as a diagnostic criterion for chronic pancreatitis [62, 63, 64].
Thus, our study is the first complex examination of morphologic alterations of the small intestine mucosa, as well as of its enzymatic activity, absorption, and local immunity, in chronic pancreatitis patients.
CONCLUSIONS
Chronic pancreatitis patients experience the development of morphological alterations in the small intestine of jejunitis type without atrophy at the stage of mild or moderate exacerbation. These alterations are maintained by changes in enzymatic processes in the sphere of membranous and intestinal digestion, worsening of small intestine absorption, accelerated epithelial desquamation, drop in local immunity and bacterial overgrowth syndrome development. It means that in chronic pancreatitis there is a disorder of digestion and absorption in the small intestine, maldigestion is attached by malabsorption. It leads to the decrease of clinical efficacy of enzymatic agents. Bacterial overgrowth syndrome formed in chronic pancreatitis also disturb the action of these preparations.
These alterations explain the lack of efficacy of enzyme replacement therapy in some patients suffering from pancreatic exocrine insufficiency related to chronic pancreatitis. It is vitally important to carry out decontamination of small intestine and escalation of enzyme preparations dosage in order to optimize the therapy in such cases.
Conflict of interest
The authors have no potential conflict of interest
References
- Lankisch PG. Natural course of chronic pancreatitis. inBeger HG, Warshaw AL, Buchler MW, et al. The pancreas: An integrated Textbook of Basic Science, Medicine, and Surgery. 2nd ed: Massachusetts, USA; Blackwell Publ, 2008:484-494.
- Lankisch PG. Natural course of chronic pancreatitis. Pancreatology 2001;1(1):3-14.
- Dominguez-Munoz JE. Pancreatic exocrine insufficiency: diagnosis and treatment. J GastroenterolHepatol 2011;26Suppl 2:12-6.
- Lankisch PG. What to do when a patient with exocrine pancreatic insufficiency does not respond to pancreatic enzyme substitution, a practical guide. Digestion 1999;60(Suppl1):97-103.
- Dominguez-Munoz JE. Pancreatic enzyme replacement therapy for pancreatic exocrine insufficiency: When is it indicated, what is the goal and how to do it? Adv Med Sci 2011;56(1):1-5.
- Mancilla AC, Madrid S AM, Hurtado HC Orellana BC, Pena ZM, Tobar AE, Berger FZ. Small intestine bacterial overgrowth in patients with chronic pancreatitis. Rev Med Chil 2008;136(8):976- 80.
- Lembcke B, Kraus B, Lankisch PG. Small intestinal function in chronic relapsing pancreatitis. Hepatogastroenterology 1985;32(3):149-51.
- Lohr J-M. Exocrine Pancreatic Insufficiency. 2nd Ed. Bremen, Germany; UNI-MED, 2010.
- Dominguez-Munoz JE, Iglesias-Garcia J. Oral pancreatic enzyme substitution therapy in chronic pancreatitis: is clinical response an appropriate marker for evaluation of therapeutic efficacy? JOP 2010;11(2):158-62.
- Ramakrishna BS, Venkataraman S, Mukopadhya A. Tropical malabsorption. Postgrad Med J 2006;82(974):779-87.
- Korotyko GF. Physiology of Digestive System. Krasnodar, Russia; RCS BK “Group B”, 2009.
- Dominguez-Munoz JE. Pancreatic enzyme therapy for Pancreatic exocrine insufficiency. CurrGastroenterol Rep 2007;9(2):116-22.
- Trespi E, Ferrieri A. Intestinal bacterial overgrowth during chronic pancreatitis. Curr Med Res Opin;15(1):47-52.
- Smout AJ. Small intestinal motility. CurrOpinGastroenterol 2004;20(2):77-81.
- Mahida YR, Chapman RW, Jewell DP. Association of small intestinal diverticulosis with chronic pancreatitis leading to severe malabsorption. Report of three cases. Postgraduate Medical Journal 1988;64:893-896.
- McEvoy A, Dutton J, James O FW. Bacterial contamination of the small intestine is an important cause of occult malabsorption in the elderly. British Medical Journal 1983;287:789-93
- Lankisch PG, Breuer N, Bruns A, Weber-Dany B, Lowenfels AB, Maisonneuve P. Natural history of acute pancreatitis: a longterm population-based study. Am J Gastroenterol 2009; 104(11):2797-2805.
- Schneider AJ, Lohr M, Singer MV. The M-ANNHEIM classification of chronic pancreatitis: introduction of a unifying classification system based on a review of previous classifications of the disease. J Gastroenterol 2007;42:101-119.
- Masevich PG, Kudryashova GP, Ugolev AM. New complex method for intestinal disorders diagnostics. TerArkh 1976:48(3):96- 103.
- Bruce-Gregorios JH. Histopathologic Techniques. Quezon City, Philippines: JMC Press Inc., 1974.
- Linevsky YV. Diagnostics and treatment of chronic enteritis (methodic recommendations). Donetsk, Ukraine: Donbass, 1978.
- Linevsky YV, Vasilenko IV. Morphological changes in small intestine mucous in patients with chronic enteritis. LikarskaSprava 1988;4:3-5.
- Ugolev AM. Determination of amylolytic activity. In: Ugolev AM, Yezuitova NN, Masevich ZY Nadirova TY, Tymofeeva NM. The Study of the Human Alimentary Apparatus. Leningrad, Russia: Nauka, 1969:187-192.
- Ugolev AM, Nurks YY. Determination of the primary stages of tributyryn hydrolysis. In: Ugolev AM, Yezuitova NN, Masevich ZY Nadirova TY, Tymofeeva NM. The Study of the Human Alimentary Apparatus. Leningrad, Russia: Nauka, 1969:182-183.
- Ugolev AM, Chernyakhovskaya MY. Determination of final stages of tryglyzeridehydrohisis. In: Ugolev AM, Yezuitova NN, Masevich ZY Nadirova TY, Tymofeeva NM. The Study of the Human Alimentary Apparatus. Leningrad, Russia: Nauka, 1969:183- 187.
- Dahlqvist A, Hammond JB, Crane RK, Dunphy JV, Littman A. Assay of disaccharidase activities in peroral biopsies of the smallintestinal mucosa. ActaGastroenterol Belg. 1964; 27: 543-555.
- Linevskiy YV. The small intestine maltase activity in chronic enteritis. Vrachebnoyedelo, 1977; 1:17-19.
- Ugolev AM, Yezuitova NN. Determination of invertaze and other disaccharidases activity. In: Ugolev AM, Yezuitova NN, Masevich ZY Nadirova TY, Tymofeeva NM. The Study of the Human Alimentary Apparatus. Leningrad, Russia: Nauka, 1969:192- 196.
- Ugolev AM, Tymofeeva NM. Determination of peptidase activity. In: Ugolev AM, Yezuitova NN, Masevich ZY Nadirova TY, Tymofeeva NM. The Study of the Human Alimentary Apparatus. Leningrad, Russia: Nauka, 1969:178-181.
- Fomina LS, Myhlin SY, Shligin GK. Methods of intestinal phosphatase determination. Biochemistry 1952;17(2):134-138.
- Kagramanova KA, Yermolyeva ZV. Comparative characteristics of lyzosyme activity methods. Antibiotics 1966; 11(10):917-919.
- Burton K. A study of the conditions and mechanism of the diphenylamine reaction for the colorimetric estimation of deoxyribonucleic acid. Biochem J 1956;62:315-323.
- Butterworth CE JR, Perez-Santiago e, Martinez de Jesus J, Santini R. Studies on the oral and parenteral administration of D (+) xylose. N Engl J Med 1959; 23;261(4): 157-164.
- Bruver RM, Salkie ML. The automatic method of qualitate determination of immunoglobulines in biological liquors. ClinBiochem 1978;11:112-118.
- Mancini G, Carbonara AO, Heremans IF. A single radialdiffusion method for the immunological quantitation of proteins. In Peeter N (ed). Proceedings of the Biological Fluids. Amsterdam, The Netherlands: Elsevier, 1964:370-379.
- Lyah YE, Gur’yanov VG, Khomenko VN, Panchenko OA. Computer Biostatistics: Data Analysis in Biology, Medicine and Pharmacology. Donetsk, Ukraina: Papakitsa EK, 2006: 214.
- Wagner DA, Schatz R, Coston R, Curington C, Bolt D, Toskes PP. A new 13C breath test to detect vitamin B12 deficiency: a prevalent and poorly diagnosed health problem. J Breath Res 2011;5(4):046001.
- Danovskiy LV. Clinical Study of Membrane Digestion. Kazan, Russia: Kazan University Press, 1976.
- Archiy EI, Ganich ON, Vinnichuk EN. On the problem of membrane digestion state in chronic pancreatitis. In: Pancreatic and Salivary Glands (Physiology and Pathology: Thesis of the Report). Lviv, Ukraine: Medical Literature, 1975.
- Strokova OA. Intestinal digestion in chronic pancreatitis patients. Exper.clin.gastroenterology 2009;5:33-37.
- Strokova OA. State of intestinal digestion in chronic pancreatitis patients. Ulyanovsk, Russia: GOU VPO Mordov State University, 2009.
- Linevskiy YV. Monoglyzerilypase insufficiency of small intestine in patients with chronic digestive disorders. Clin med 1988;10:116-119.
- Linevskiy YV. Dipeptidase activity of small intestine mucous membrane in chronic digestive disorders. Sov Med 1988;7:9-10.
- Linevskiy YV, Zazimko AS, Linevskaya KY. Ill activity of small intestine disacharidases in some chronic disorders of digestive sustem. In: Gastroenterology, Vol 19. Kiev, Ukraine: Zdorovya, 1987:96-98.
- Linevskiy YV. Intestinal maltases activity in digestive disorders. In: Gastroenterology, Vol. 13. Kiev, Ukraine: Zdorovya, 1981:62-65.
- Gubergrits NB, Linevsky YV, Zagorenko YA. Morphological and functional changes of small intestine in patients with chronic pancreatitis (chronic pancreatitis). Pancreatology 2006;6(4):371-372.
- Gubergrits NB, Linevsky YV. Peculiarities of syndrome of bacterial overgrowth and its treatment in chronic pancreatitis. Pancreatology 2009;9(4):506.
- Gubergrits NB, Zagorenko YA, Belyayev VV. Pathogenetic aspects of enteropancreatic syndrome. Pancreatology 2003;3(3):230.
- Gubergrits NB, Zagorenko YA. Functional pathology of small intestine in patients suffering from chronic relapsing pancreatitis. Pancreatology 2003;3(3):231.
- Vasilenko VX, Vinogradova MA. On the problem of insufficient intake of nutrients and classification of its types. Clin med 1967;45(2):9-18.
- Ishmuhametova AI. Radioisotopic Study of Fats, Proteins and Vitamin B12 Intake in Digestive Disorders. Moscow, Russia: Medicine, 1970.
- Trusov VV, Plastilina RA, Ryabov VI. Complex study of small intestine intake function in clinical conditions by means of some chemical and radioactive markers. In: Tareev EM, Dembo AG. Works of Third Congress of Therapeutists. Leningrad, Russia: Medicine, 1970:288-294.
- Chey SY, Shay H, O’Leary DK. Absorption of fats and external pancreatic secretion. Gastroenterology 1963;45(2):196-202.
- Balcerzak SP, Peternel WW, Heinle BW. Iron absorption in chronic pancreatitis. Gastroenterology 1967;53(2):257-264.
- Gubergrits AY, Linevskiy YV. Disorders of Small Intestine. Moscow, Russia: Medicine, 1975.
- GrigorevaIuV, Iakovenko EP, Volosheinikova TV, Ovsiannikova IA, Lavrent’eva SA. The clinical manifestations and duodenal mucosa in the patients with chronic pancreatitis and bacterial overgrowth in the small intestine. EkspKlinGastroenterol2010;(11):29-34.
- Scarpignato C, Pelosini I. Rifaximin, a poorly absorbed antibiotic: pharmacology and clinical potential. Chemotherapy 2005;51Suppl 1:36-66.
- Madsen JL, Graff J, Philipsen EK, Scharff O, Rumessen JJ. Bile acid malabsorption or disturbed intestinal permeability in patients treated with enzyme substitution for exocrine pancreatic insufficiency is not caused by bacterial overgrowth. Pancreas 2003;26(2):130-3.
- Bode JC, Bode C. Alcohol, the gastrointestinal tract and pancreas. TherUmsch 2000;57(4):212-9.
- Crabbe PA, Heremans JF. The distribution of immunoglobulincontaining cells along human gastrointestinal tract. Gastroenterology 1966;51:305-316.
- Brasher GW, Dyck WP, Hall FF, Spiekermann A. Immunoglobulin characterization of human pancreatic fluid. Am J Dig Dis 1975;20(5):454-458.
- Laptev VV, Grivazyan GA, Shapovalyanz SG. Immunoregulation in acute pancreatitis patients therapy. News of Surgery n. a. Grekov 1987;3:40-42.
- Sanguigni S, Paparo BS, Meledandri G, Cifalelli F. Le IgA secroirenellepancreatitichroniche. Epatologia 1983;29(5):221-226.
- Soto J, Aufses AH Jr, Drelling DA. The pancreas and immunoglobulins. 2: Immunoglobulin levels in the pancreatic secretion of patients with chronic pancreatitis. Amer J Gastroenterol 1977;67(6):561-564.



