Makiko Ono, Terumi Kamisawa, Yuyang Tu, Naoto Egawa
Department of Internal Medicine, Tokyo Metropolitan Komagome Hospital, Tokyo, Japan
- *Corresponding Author:
- Makiko Ono
Department of Internal Medicine
Tokyo Metropolitan Komagome Hospital
3-18-22 Honkomagome, Bunkyo-ku
Tokyo
113-8677 Japan
Phone: +81-3.3823.2101
Fax: +81-3.3824.1552
E-mail: makiko-o@yg8.so-net.ne.jp
Received February 23rd, 2005 - Accepted March 1st, 2005
Keywords
Cholangiopancreatography, Endoscopic Retrograde; Cholangiopancreatography, Magnetic Resonance; Diverticulum
INTRODUCTION
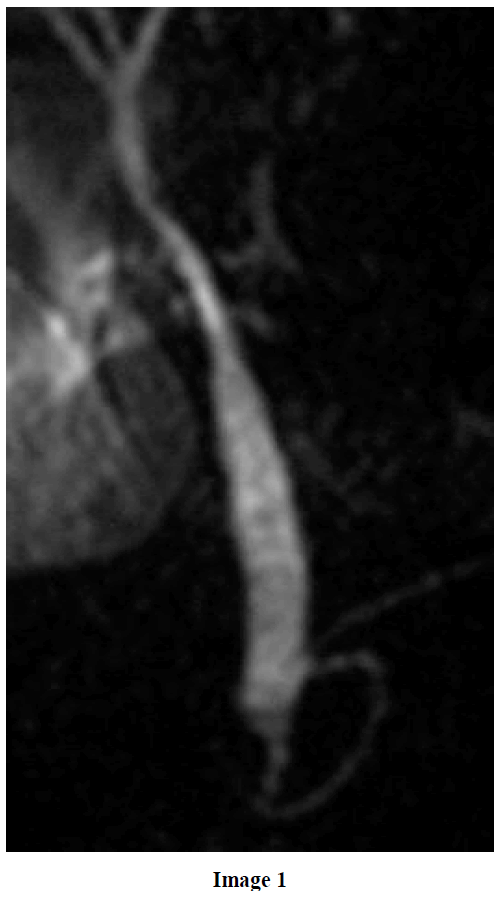
A 63-year-old male was referred for jaundice and general fatigue. Computed tomography of the abdomen showed several gallbladder stones and gallbladder wall thickening. The laboratory data was the following: total bilirubin 2.2 mg/dL (reference range: 0.2-1.1 mg/dL), direct-bilirubin 0.6 mg/dL (reference range: 0-0.2 mg/dL), SGOT 46 IU/L (reference range: 12-32 IU/L), SGPT 79 IU/L (reference range: 7-43 IU/L), GGT 254 IU/L (reference range: 9-70 IU/L). After admission, coronal heavily T2-weighted single-shot rapid acquisition with relaxation enhancement magnetic resonance cholangiopancreatography (MRCP), carried out without secretin injection, demonstrated a lateral compression of the distal common bile duct (Image 1).On duodenoscopy, the major duodenal papilla with a normal orifice was located in the periampullary duodenal diverticulum (Image 2). Endoscopic retrograde cholangiopancreatography (ERCP) with injection of contrast material into the diverticulum revealed that the distal common bile duct was laterally compressed by the diverticulum (Image 3). There were no findings of bile duct stones or dilatation of the common bile duct. His symptoms and laboratory data improved quickly after admission. We diagnosed him as having Lemmel syndrome.


Lemmel advocated that periampullary duodenal diverticulum often compressed the distal common bile duct and prevented the secretion of the bile [1]. Several reports have demonstrated an association between periampullary duodenal diverticulum and gallstone disease [2, 3]. MRCP is a noninvasive imaging modality which is useful for examination of patients with obstructive jaundice. Although MRCP with secretin stimulation could demonstrate a periampullary duodenal diverticulum which was filled with secreted pancreatic juice [4], a routine MRCP without secretin injection has low sensitivity for the detection of a periampullary duodenal diverticulum [5]. Lateral compression of the distal common bile duct on MRCP without secretin injection implies the possibility of periampullary duodenal diverticulum.
References
- Lemmel G. Die KlinischeBedeutung der Duodenal Divertikel. Arch Verdauungskrht 1934; 46:59-70.
- Egawa N, Kamisawa T, Tu Y, Sakaki N, Tsuruta K, Okamoto A. The role of juxtapapillary duodenal diverticulum in the formation of gallbladder stones. Hepatogastroenterology 1998; 45:917-20. [PMID 9755980]
- De Koster E, Denis P, Mante M, Otero J, Nyst J, Jonas C, et al. Juxtapapillary duodenal diverticula: Association with biliary stone disease. Acta Gastroenterol Belg 1990; 53:338-43. [PMID 2127651]
- Doai K, Uchiyama K, Kuniyasu Y, Saisyo H. MR cholangiopancreatography of Mirizzi syndrome and Lemmel syndrome. (in Japanese) Nippon Rinsho 1998; 56:2933-8. [PMID 9847624]
- Tsitouridis I, Emmanouilidou M, Goutsaridou F, Kokozidis G, Kalambakas A, Papastergiou C, Tsantiridis C. MR cholangiography in the evaluation of patients with duodenal periampullary diverticulum. Eur J Radiol 2003; 47:154-60. [PMID 12880997]

