Keywords
Pancreatic Fistula; Pancreatitis, Acute Necrotizing;
Retropneumoperitoneum
Abbreviation
PCFs pancreaticocolonic fistulas; WOPN walled-off
pancreatic necrosis
INTRODUCTION
Colonic fistulas occur in 3%– 10% of patients with severe
acute pancreatitis [1]. An air pocket in a necrotic area of the
pancreas usually indicates that infected necrosis is present and/
or there is a fistula to the gastrointestinal tract. The root of the
mesocolon serves as a potential route for spread of inflammatory
mediators to the colonic wall. This inflammation may lead to
thrombosis of mesenteric vessels and subsequently to necrosis of
the colonic wall [2]. The consequences of a colonic fistula may be
more severe than those of fistulas at other sites of gastrointestinal
tract because of the heavy load of multiple organisms [3]. We
report a complex case of multiple pancreaticocolonic fistulas
that was successfully treated with extended left hemicolectomy
along with pancreatic necrosectomy, drainage of all Walled-off
Pancreatic Necrosis collections.
CASE REPORT
A forty-three-years-old male patient presented to
an outside hospital, 10 weeks before he presented to us,
with biliary pancreatitis, for which he was admitted, at
that time his laboratory findings showed, leukocytosis
(12.3×10^9/L), Hemoglobin 8 g/dL, HCT 25%, ESR 60
mm/H, CRP >20 mg/dL (N: 0-0.3), S. Amylase 475 U/L (Figure 1).
Figure 1. Acute Pancreatitis with Peripancreatic Collection.
The treating physician referred the patient to another
institution where he had been admitted in ICU as the
patient developed Adult Respiratory Distress Syndrome
(ARDS) secondary to sepsis, and kept on ventilator for 12
days, after which he was discharged to general ward.
Gradually, he tolerated fat free diet. Before the patient
discharge (after 6 weeks of admission), CECT done
for him, Figure 2 showed WOPN along with paracolic
collection and there was no Pneumoretroperitoneum.
As the patient was asymptomatic at that time, no any
form of interventions had been done for the collections
by his treating physician.
Figure 2. CECT Abdomen Sagittal view; Walled-off Pancreatic Necrosis (WOPN), with Paracolic Collection.
After discharge by 4 weeks, the patient presented in
our emergency department with dull aching epigastric
pain, radiated to the back associated with anorexia and
repeated vomiting and intolerance to food, with recent
loss of about 25 kg of his weight.
His most distressing complaint was frequent diarrhea
which was purulent, yellowish in color with offensive
odor, about 5 times per day. No history of fever or night
sweating.
No past history of chronic illness but he had had gall
stones which had not been treated yet.
No past history of drugs or alcohol intake, and no
history of surgical intervention before.
On examination; the patient looked ill, tachypnic,
dehydrated and pale, but was not jaundiced Temp 37.2, P 125 b/m, RR 28/m, BP 127/75 mmHg,
Weight 79 kg (it was 125 kg before), Height: 175 cm. The
abdomen was distended, there was an ill-defined tender
epigastric mass about 20 × 20 cm which represented
the pancreatic phlegmon. The rest of the abdomen
was soft and lax. Hernia orifices were intact. Digital
rectal examination revealed yellowish colored loose
and offensive stool without blood. Lower limbs were
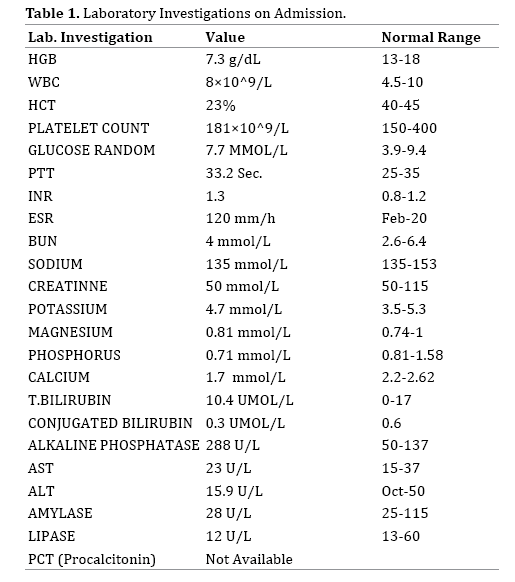
edematous, more in the left side, but not tender. Table
1 showed the laboratory data on admission.
CT chest, showed evidence of moderate left pleural
effusion. CT abdomen and pelvis with IV and oral
contrast showed WOPN (Figure 3). The peripancreatic
collection caused compression and narrowing of the
second part of duodenum. The midpart of transverse
colon was collapsed and closely related to the large
preipancreatic fluid collection. There was extensive
Pneumoretroperitoneum within a huge retroperitoneal
septated and multiloculated collection in the lesser sac,
which extended to left and right subhepatic and left
paracolic gutter up to left inguinal region (Figure 4).
Figure 3. Axial CECT Abdomen shows Necrotizing Pancreatitis with Extensive Pneumoretroperitoneum.
Figure 4. Abdominal CECT Coronal View shows Walled-off Paracolic Collections with Extensive Air Foci.
These extensive air foci were supposed to be due to
either superadded infection or the presence of PCF.
Lower limbs Duplex US showed left superficial
femoral and popliteal veins thrombosis so, IVC catheter
was inserted. The patient was admitted to the ICU and
parenteral nutrition started.
As the patient was in SIRS, and he had element
of gastric outlet obstruction along with extensive
pneumoretroperitoneum, within non amenable
multiseptated collections for percutaneous drainage, we
had prepared him for exploratory laparotomy aiming
for pancreatic necrosectomy, drainage of all collections,
relieving the gastric outlet compression and tackling the
possible colonic fistulas.
Operative Notes
Upon entry of the peritoneal cavity, there was a big
phlegmon in the region of the lesser sac, entry of the
lesser sac was quite difficult, a gush of foul smelled thick
pus came out, the pancreatic necrosis was already well
demarcated, necrosectomy done (Figure 5). Opening of
all sub hepatic and paracolic collections with removal of
all necrotic tissues from within the collections done. Total
amount of pus aspirated about 3 liters.
Figure 5. Necrosed Pancreatic and Parapancreatic Tissues.
Upon inspection of the transverse and descending
colon which looked dark in color and stenosed, there were
5 fistulas, 2 in numbers between the transverse colon and
the lesser sac collection (Figure 6), and 3 fistulas between
the descending colon and its corresponding left paracolic
collection (Figure 7). So extended left hemicolectomy
done with side to side colonic anastomosis, along with
protecting loop ileostomy. The sizes of the fistulas ranged
between 1 to 2.5 cm in diameter.
Figure 6. The 5 Instruments point to The 5 fistulas; 2 in The Transverse Colon and 3 in The Descending colon.
Figure 7. Close-up View of the 3 Fistulas in Left Colon.
Subtotal cholecystectomy done as there was extensive
adhesions, in the triangle of Calot. Four drains were
inserted, 2 in the region of pancreatic remnant, for planned
post operative saline irrigation, closure done but the skin
left open.
The patient shifted back to ICU, kept on total parenteral
nutrition. Cultures of pus and pancreatic necrosis showed
E.Coli and Enterococcus faecium, so appropriate antibiotics
started along with antifungal agent.
Continuous saline irrigation was started as the upper
drains brought remnant of necrotic tissues. Irrigation
stopped after couple of weeks.
Postoperative course was hectic, as the patient
developed the following complications:-
1. Wound infection, treated with frequent dressing.
2. Upper limb DVT involved left internal jugular,
subclavian and cephalic veins, although he was on
heparin.
3. HIT (Heparin induced thrombocytopenia), we
stopped heparin.
4. Right lower lobar pneumonia, resolved later on.
5. Biliary leak (Figure 8) as the gall bladder stump
gave way due to slipped CBD stone, for which ERCP
and sphinterotomy done. The fistula closed later on.
Figure 8. MRCP shows Biliary Leak.
6. Multiple splenic infarctions (Figure 9), resolved
later on, evidenced by MRI abdomen.
Figure 9. CECT Abdomen shows Multiple Splenic Infarctions
7. Prolonged intubation, invited for percutaneous
tracheostomy.
The patient discharged from the ICU after 8 weeks to
general ward.
Follow up CT abdomen done after 8 weeks of admission
showed complete resolution of the inflammatory process
of the pancreas, as well as all the loculated collection.
3 weeks later the patient discharged home on warfarin.
The loop ileostomy had been taken down later along
with excision of the remnant of the gall bladder to avoid
stone formation in the future.
DISCUSSION
Acute necrotizing pancreatitis is diagnosed when more
than 30% of the gland is affected by necrosis and accounts
for 5% to 10% of pancreatitis cases [4].
PCFs occur in 3% – 10% of patients with severe acute
pancreatitis [1]. An air pocket in a necrotic area of the
pancreas usually indicates that infected necrosis is present
and/or there is a fistula to the gastrointestinal tract [2].
In the current literature, there are several theories
concerning colonic involvement in the course of acute
necrotizing pancreatitis the most important mechanism is
the spread of pancreatic enzymes and arising necrosis of
surrounding tissues [5, 6].
The root of the mesocolon serves as a potential route
for spread of inflammatory mediators to the colonic wall.
This inflammation may lead to thrombosis of mesenteric
vessels and subsequently to necrosis of the colonic wall
with subsequent fistula formation [2].
PCFs can also be an adverse complication of
interventional treatment of acute necrotizing pancreatitis,
such as percutaneous drainage of pancreatic fluid
collections [7, 8].
Typically, the clinical manifestations of PCF include
diarrhea, hematochezia, and fever. Less frequently,
however, PCF may result in a large bowel obstruction,
which accounts for less than 1% of patients with PCF [1, 9, 10]. Mateusz et al. [11] reported symptoms likely related to
the presence of PCF only in 12 out of 21 patients (57.14%).
Melena was noted in seven patients, while hematochezia
with diarrhea was observed only in three patients.
In our patient, however, the most distressing complaint
was the frequent passage of foul smelled diarrhea but
there was no hematochezia or fever.
Unless kept in mind, the diagnosis of PCF is considered
to be difficult due to unspecified symptoms [10, 12, 13, 14].
Conventional CT is not considered a successful method
in demonstrating pancreatico-colonic fistulas and its
sensitivity is low as compared to ERCP [15]. The most
probable reason for its low sensitivity is the failure of the
oral contrast material to induce luminal distension and
pressure to fill the fistulous tracts. The sensitivity of the
CT in detecting fistulas can be increased by using rectally
administered contrast material [16].
Although in our case we had done preoperative CT
using rectal water-soluble contrast media we were not able
to directly detect the fistulous tracts, may be due to the
high pressure in the collection interfering with backward
flow of the contrast from the lumen of the colon back to the
collections. The only the indirect evidence for the presence of
PCF was the presence of extensive pneumoretroperitoneum.
ERCP is considered the best modality for the detection
of pancreatico-colonic fistulas [15].
In one study, ERCP was able to discover the presence
of PCF in all studied patients with WOPN and PCF [11].
The advantage of ERCP over other imaging modalities is
the added benefit of pancreatic stent placement in order to
bridge the disruption site [17, 18].
In our case, however we did not ask for ERCP as a
diagnostic tool, first as the patient was not jaundiced,
second the patient was just started on heparin drip for
the acute lower limb DVT, thirdly we concerned about
the possible added complications of ERCP to the already
complex presentation of the patient.
The diagnosis on infected WOPN is crucial for early
institution of antibiotics and further interventions as
needed. CT findings suggestive of an infection include the
presence of extra-luminal gas, but still some authorities
believe that a definitive diagnosis can only be confirmed
when a percutaneous image guided or endoscopic
ultrasound (EUS)-guided fine needle aspiration (FNA) is
positive for bacterial/fungal stain or culture [19].
In our case, infected WOPN was suspected indirectly by
the presence of extensive air foci within all collections, and
confirmed by the positive cultures which showed E.Coli
and Enterococcus faecium.
While sterile necrosis is associated with 5 % to 10 %
mortality rate, the mortality rate increases to 20%-30%
when necrosis becomes infected [20, 21, 22]. Thus, early
recognition and institution of appropriate therapy is
necessary.
Two thirds of necrotic pancreatic collections are sterile
and will resolve with conservative management, while the
remainder will become infected and will require further
intervention [23].
An infected pancreatic fluid collection dictates drainage.
Endoscopic drainage should be preferred over radiological
one whenever possible due to better drainage and
decreased risk of percutaneous fistula, and over surgery
because of high morbidity and mortality of the latter [24].
Accepted indications for surgical intervention of WOPN
include proven infected necrosis, clinical deterioration, or
persistent symptoms due to complications of pancreatic
infection.
Our patient, presented to us in sepsis manifested by
features of Systemic Inflammatory Response Syndrome
(SIRS), with Pulse 125 b/m and Respiratory Rate of
28 /m, beside the proved positive culture from the
collections which grown E. Coli and E. Faecium, the source
of sepsis.
There is a general consensus to delay intervention to
at least 3-4 weeks after onset of disease and preferably
as late as is feasible [25, 26], to allow better demarcation
of the necrosis and to avoid unnecessary removal of
normal pancreatic tissues which can cause post operative
endocrine and exocrine insufficiency.
Open necrosectomy used to be the standard approach
for treating infected pancreatic necrosis. This approach
is associated with high morbidity and mortality rates (up
to 95% and 25%, respectively), as well as debilitating
complications such as entero-cutaneous and pancreaticocutaneous
fistula formation [27, 28].
However, over the last decade, a variety of minimally
invasive interventions for the treatment of acute
necrotizing pancreatitis have been introduced as
alternatives to the traditional open necrosectomy [29].
Laparoscopic approaches for pancreatic necrosectomy
have proved efficacy with a survival rate as high as 85%
[30, 31], and is associated with a lower incidence of new
onset organ failure post-operatively when compared
to the open approach [32, 33]. The current technique
for laparoscopic necrosectomy is using a retrogastric
transmesocolic or retroperitoneal approach to the lesser
sac [34]. Another alternative after the placement of the
percutaneous drain would be a videoscopic-assisted
retroperitoneal debridement (VARD), where a small 5 cm
subcostal incision is made to allow larger pieces of solid
debris to be removed.
The PANTER trial (PAncreatitis, Necrosectomy versus
sTEp up appRoach) assigned patients with pancreatic
necrosis and infected necrosis to either primary
open necrosectomy or a step up approach, where a
percutaneous drain was initially placed followed by
minimally invasive retroperitoneal necrosectomy
when needed. It showed that a minimally invasive
step up approach was associated with a lower rate of
major complications and death when compared to
open necrosectomy [35]. The step up approach has
proven its efficacy since most necrotic collections are
percutaneously accessible and large pieces of necrosis
can be removed; however, there is risk of developing
a chronic pancreatico-cutaneous fistula with this
approach [36].
However, till date, there are no established guidelines
for the treatment of WOPN with colonic fistula.
There are recent reports of several cases of PCF have
been successfully treated by endoscopic interventions,
such as pancreatic stent, [37] endoscopic clip with
fibrin glue, [38, 39] and over-the-scope clip system.
While Renteln et al. [40] reported upon the efficacy of
conventional endoscopic clips for the closure of small
colonic perforations, endoscopic clips may not be sufficient
for the closure of larger perforations [41].
Mateusz et al. [11], studied the efficiency and
safety of endoscopic treatment in 21 patients with
WOPN complicated with PCF, where, transmural,
necrogastrostomy or necroduodenostomy, drainage was
attempted in all patients with symptomatic WOPN, but
drainage was not performed if the distance between the
wall of the fluid collection and the gastrointestinal wall
exceeded 15 mm.
The place of fistulotomy was chosen under EUS
guidance. Fistulotomy was performed on the top of the
largest protuberance of the necrotic collection into the
gastrointestinal wall. The opening between the lumen of
the gastrointestinal tract and the lumen of the necrotic
collection was widened with the use of a bougie dilator. A
nasocystic drain and several double-pigtail or 10 French stents were inserted into the cavity lumen of the collection,
through which postproceural saline irrigation of the
necrotic collection was done.
Complete therapeutic success of WOPN complicated
with PCF was achieved in 16 of the 21 patients (76.19%),
while the closure of PCF was confirmed by CECT imaging
in 17 of the 21 patients (80.95%), The recurrence of WOPN
was observed in six of the 21 (28.57%) patients during
follow-up, but no PCFs were found in any of the patients
with recurrence of pancreatic fluid collection.
In our case, however, we have taken the decision for
surgical intervention. First, as the patient had multiseptated
multiple collections in the lesser sac, right and left paracolic
gutter up to the left inguinal region, which were not
amenable to percutaneous drainage, beside, we don’t have
the facility of endoscopic drainage. Second, we couldn’t
exclude the existence of the multiple PCFs preoperatively.
Thirdly, the patient could not tolerate orally with repeated
vomiting, as he had an element of gastric outlet obstruction
as the duodenum was compressed by the peripancreatic
collection.
Till date, we don’t know whether the endoscopic
drainage with or without over the scope clipping of the
multiple large fistulas (more than 10 mm) could succeed
with our patient or not.
Shuhei et al. [42] treated one patient with solitary PCF at
the splenic flexure of the transverse colon after Endoscopic
Ultrasound-Guided Cyst Drainage for Pancreatic
Pseudocyst, surgically with a diverting colostomy and
abscess drainage. After the surgery, the patient’s condition
improved and was discharged on the 37th day.
Although, In our patient the option of extended
left hemicolectomy with diverting ileostomy was an
aggressive option, we have chosen it as we doubted the
healing of these multiple wide fistulas if we did only
drainage with diverting ileostomy or colostomy and to
the best of our knowledge we couldn’t find a similar
case in the literature with multiple large PCFs treated
conservatively or with other minimally invasive or
surgical approaches.
CONCLUSION
Despite the aggressive surgical strategy and number
of following complications, our patient discharged home
safely, and on follow up, he had no recurrence of the WOPN
or the PCFs.
Although PCF could be diagnosed during ERCP, in our
humble opinion, the presence of PCF should be suspected
in cases of WOPN with recent history of persistent
diarrhea, the presence of air foci within the collection,
the isolation of Enterococcus faecium or E- faecalis from
WOPN aspirate, and if open drainage and necrosectomy
was decided it would be wise to check the nearby colon for
the presence of PCF.
Conflicts of Interest
There are no conflicts of interest.
References
- Suzuki A, Suzuki S, Sakaguchi T, Oishi K, Fukumoto K, Ota S, et al. Colonic fistula associated with severe acute pancreatitis: report of two cases. Surg Today 2008; 38: 178-183. [PMID: 18239882]
- Aldridge MC, Francis ND, Glazer G, Dudley HA. Colonic complications of severe acute pancreatitis. Br J Surg 1989; 76: 362-367. [PMID: 2655821]
- Rerknimitr R, Lakananurak N, Prueksapanich P, Sallapant S, Angsuwatcharakon P, Kongkam P, et al. A fatal case of a colonic fistula communicating with a walled- off area of pancreatic necrosis. Endoscopy 2014; 46(Suppl 1 UCTN): E30-E31. [PMID: 24523168]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62:102–111. [PMID: 23100216]
- Doberneck RC. Intestinal fistula complicating necrotizing pancreatitis. Am J Surg 1989; 158:581–584. [PMID: 2589594]
- Van Minnen LP, Besselink MG, Bosscha K, Van Leeuwen MS, Schipper ME, Gooszen HG. Colonic involvement in acute pancreatitis: a retrospective study of 16 patients. Dig Surg 2004; 21:33–38. [PMID: 14707391]
- Shankar S, vanSonnenberg E, Silverman SG, Tuncali K, Banks PA. Imaging and percutaneous management of acute complicated pancreatitis. Cardiovasc Intervent Radiol 2004; 27:567–580. [PMID: 15578132]
- Wolfsen HC, Kozarek RA, Ball TJ, Patterson DJ, Traverso LW, Freeny PC. Pancreaticoenteric fistula: no longer a surgical disease? J Clin Gastroenterol 1992; 14:117–121. [PMID: 1556424]
- Gandjour A. Simplifying rules for optimal allocation of preventive care resources. Expert Rev Pharmacoecon Outcomes Res 2012; 12:231-5. [PMID: 22458624]
- Abcarian H, Eftaiha M, Kraft AR, Nyhus LM. Colonic complications of acute pancreatitis. Arch Surg 1979; 114:995–1001. [PMID: 485850]
- Mateusz J, Marian S, and Krystian A. Endoscopic treatment of walled-off pancreatic necrosis complicated with pancreaticocolonic fistula. Surg Endosc 2018; 32:1572–1580. [PMID: 29344783]
- Heeter ZR, Hauptmann E, Crane R, Fotoohi M, Robinson D, Siegal J, et al. Pancreaticocolonic fistulas secondary to severe acute pancreatitis treated by percutaneous drainage: successful nonsurgical outcomes in a single-center case series. J Vasc Interv Radiol 2013; 24:122–129. [PMID: 23176965]
- Alsumait AR, Jabbari M, Goresky CA. Pancreaticocolonic fistula: a complication of pancreatitis. Can Med Assoc J 1978; 119:715–719. [PMID: 709471]
- Thomas CT, Hinton PJ, Thomas E. Spontaneous pancreatic duct-colon fistula. J Clin Gastroenterol 1986; 8:69–73. [PMID: 3517133]
- Shim KS, Suh JM, Yang YS, Choi JY, Park YH. Three-dimensional demonstration and endoscopic treatment of pancreaticoperitoneal fistula. Am J Gastroenterol 1993; 88:1775–1779. [PMID: 8213724]
- Tüney D, Altun E, Barlas A, Yegen C. Pancreatico-Colonic Fistula after Acute Necrotizing Pancreatitis. Diagnosis with Spiral CT Using Rectal Water Soluble Contrast Media. JOP. J Pancreas (Online) 2008; 9:26-29. [PMID: 18182739]
- Shrode CW, Macdonough P, Gaidhane M, Northup PG, Sauer B, Ku J, et al. Multimodality endoscopic treatment of pancreatic duct disruption with stenting and pseudocyst drainage: how efficacious is it? Dig Liver Dis 2013; 45:129–133. [PMID: 23036185]
- Varadarajulu S, Noone TC, Tutuian R, Hawes RH, Cotton PB. Predictors of outcome in pancreatic duct disruption managed by endoscopic transpapillary stent placement. Gastrointest Endosc 2005; 61:568–575. [PMID: 15812410]
- Banks PA, Gerzof SG, Langevin RE, Silverman SG, Sica GT, Hughes MD. CT-guided aspiration of suspected pancreatic infection: bacteriology and clinical outcome. Int J Pancreatol 1995; 18:265–270. [PMID: 8708399]
- Dervenis C, Johnson CD, Bassi C, Bradley E, Imrie CW, McMahon MJ, et al. Diagnosis, objective assessment of severity, and management of acute pancreatitis. Santorini consensus conference. Int J Pancreatol 1999; 25:195–210. [PMID: 10453421]
- Beger HG, Rau B, Isenmann R. Natural history of necrotizing pancreatitis. Pancreatology 2003; 3:93–101. [PMID: 12774801]
- Werge M, Novovic S, Schmidt PN, Gluud LL. Infection increases mortality in necrotizing pancreatitis: a systematic review and meta-analysis. Pancreatology 2016; 16:698–707. [PMID: 27449605]
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013; 13(4 Suppl 2):e1–e15. [PMID: 24054878]
- Freeman ML, Werner J, van Santvoort HC, Baron TH, Besselink MG, Windsor JA, et al. Interventions for necrotizing pancreatitis: summary of a multidisciplinary consensus conference. Pancreas 2012; 41:1176–1194. [PMID: 23086243]
- Uhl W, Warshaw A, Imrie C, Bassi C, McKay CJ, Lankisch PG, et al. IAP Guidelines for the Surgical Management of Acute Pancreatitis. Pancreatology 2002; 2:565-73. [PMID: 12435871]
- Besselink MG, Verwer TJ, Schoenmaeckers EJ, Buskens E, Ridwan BU, Visser MR, et al. Timing of surgical intervention in necrotizing pancreatitis. Arch Surg 2007; 142:1194-201. [PMID: 18086987]
- Rau B, Bothe A, Beger HG. Surgical treatment of necrotizing pancreatitis by necrosectomy and closed lavage: changing patient characteristics and outcome in a 19-year, single-center series. Surgery 2005; 138:28–39. [PMID: 16003313]
- Connor S, Alexakis N, Raraty MG, Ghaneh P, Evans J, Hughes M, et al. Early and late complications after pancreatic necrosectomy. Surgery 2005; 137:499–505. [PMID: 15855920]
- Navaneethan U, Vege SS, Chari ST, Baron TH. Minimally invasive techniques in pancreatic necrosis. Pancreas 2009; 38:867-75. [PMID: 19855233]
- Adamson GD, Cuschieri A. Multimedia article. Laparoscopic infracolic necrosectomy for infected pancreatic necrosis. Surg Endosc 2003; 17:1675. [PMID: 14973724]
- Parekh D. Laparoscopic-assisted pancreatic necrosectomy: a new surgical option for treatment of severe necrotizing pancreatitis. Arch Surg 2006; 141:895–902. discussion 902-903. [PMID: 16983033]
- van Santvoort HC, Besselink MG, Bollen TL, Buskens E, van Ramshorst B, Gooszen HG. Case-matched comparison of the retroperitoneal approach with laparotomy for necrotizing pancreatitis. World J Surg 2007; 31:1635–1642. [PMID: 17572838]
- Raraty MG, Halloran CM, Dodd S, Ghaneh P, Connor S, Evans J, et al. Minimal access retroperitoneal pancreatic necrosectomy: improvement in morbidity and mortality with a less invasive approach. Ann Surg 2010; 251:787–793. [PMID: 20395850]
- Alsfasser G, Hermeneit S, Rau BM, Klar E. Minimally invasive surgery for pancreatic disease - current status. Dig Surg 2016; 33:276–283. [PMID: 27216738]
- van Santvoort HC, Besselink MG, Bakker OJ, Hofker HS, Boermeester MA, Dejong CH, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med 2010; 362:1491–1502. [PMID: 20410514]
- van Grinsven J, van Santvoort HC, Boermeester MA, Dejong CH, van Eijck CH, Fockens P, et al. Timing of catheter drainage in infected necrotizing pancreatitis. Nat Rev Gastroenterol Hepatol 2016; 13:306–312. [PMID: 26956064]
- Howell DA, Dy RM, Gerstein WH, Hanson BL, Biber BP. Infected pancreatic pseudocysts with colonic fistula formation successfully managed by endoscopic drainage alone: report of two cases. Am J Gastroenterol 2000; 95:1821-3. [PMID: 10925992]
- Will U, Meyer F, Hartmeier S, Schramm H, Bosseckert H. Endoscopic treatment of a pseudocystocolonic fistula by band ligation and endoloop application: case report. Gastrointest Endosc 2004; 59:581-583. [PMID: 15044905]
- Karvonen J, Gullichsen R, Salminen P, Grönroos JM. Endoscopic treatment of pseudocystocolonic fistula with fibrin glue. Gastrointest Endosc 2010; 72:664-665. [PMID: 20421099]
- von Renteln D, Schmidt A, Vassiliou M, Rudolph HU, Gieselmann M, Caca K. Endoscopic closure of large colonic perforations using an over the-scope clip: a randomized controlled porcine study. Endoscopy 2009; 41:481–486. [PMID: 19533550]
- Familiari P, Marci A, Consola P, Angiò L, Scaffidi MG, Famulari C, Familiari L. Endoscopic clipping of a colocutaneous fistula following necrotizing pancreatitis: case report. Dig Liver Dis 2003:907–910. [PMID: 14703889]
- Oana S, Shibata S, Matsumoto T. Pancreatico-Colonic Fistula after Endoscopic Ultrasound-Guided Cyst Drainage for Pancreatic Pseudocyst: Report of Three Cases. JOP. J Pancreas (Online) 2016; 17:334-339.










