Keywords
Drug Therapy; Evidence-Based Medicine; Meta- Analysis as Topic; Neoadjuvant Therapy; Pancreatic Carcinoma; Pancreatic Neoplasms; Radiotherapy
Abbreviations
NCCN: National Comprehensive Cancer Network; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RECIST: Response Evaluation Criteria in Solid Tumors
INTRODUCTION
The rationale for delivering preoperative treatment to patients with borderline resectable tumors, as defined originally by Varadhachary et al. in 2006, and subsequently endorsed by Americas HepatoPancreato-Biliary Association (AHPBA) and National Comprehensive Cancer Network (NCCN) guidelines [1, 2, 3], is based on: a) potential downstaging to maximize R0 resections; b) selecting for surgery patients with stable or responding disease; c) early treatment of micrometastatic disease; and d) giving therapy in a neoadjuvant setting, when it is expected to be better tolerated.
Although this strategy has a sound rationale, its merits have not been demonstrated yet. A number of randomized controlled trials were unable to show a benefit of neoadjuvant chemo-radiotherapy for the subset of patients with locally-advanced pancreatic cancer. However, these studies enrolled heterogeneous groups of patients, as they included either those with a truly unresectable lesions and those with borderline resectable cancers [4, 5].
Objective of the present investigation was to evaluate the effectiveness of chemo-radiotherapy delivered pre-operatively in downstaging the disease in patients with borderline resectable pancreatic cancer, with emphasis on tumor response, resectability, and survival.
METHODS
Trial Selection
We included studies with a prospective design, where the pre-operative administration of chemotherapy, alone or in combination with radiotherapy, was considered in patients with preoperatively staged borderline resectable pancreatic cancer. To refine the selection, we considered only trials carried out according to predefined protocols, approved by institutional boards, and those with the following design: neoadjuvant therapy followed by re-staging, and surgical exploration/resection. We excluded retrospective studies, reports of identical patient cohorts, and those available only in abstract form. Further exclusion criteria were: trials including patients with different stages of the disease from which separate results were irretrievable, trials that administered intra-operative radiotherapy, and reports lacking information on pancreatic resection rates.
Search Strategy
Trials were identified by searching MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials from 1966 to September 2012. The search strategy included the following: (pancreatic AND (neoplasm OR cancer)) OR "pancreatic neoplasms" [MeSH Terms] AND ((chemotherapy OR irradiation OR neoadjuvant OR radiotherapy) AND (surgery OR resectable OR unresectable)) AND therapy/broad [FILTER] NOT ((animals [MH] NOT humans[MH]) OR (review [PT] NOT (systematic OR pooling OR pooled OR metaanalysis))). Manual searching included reading through reference lists of relevant papers to capture missing studies that met our inclusion criteria.
Methods of the Review
Three reviewers (A.A., V.F., and G.U.) scanned the abstract of identified studies to determine eligibility. Full articles were then selected for further assessment if the abstract suggested the study was relevant. Papers not meeting inclusion criteria were excluded and reasons for their omission listed. Disagreements were resolved through discussion. Although no randomized phase III trial on this topic has been published so far, general recommendations from the Quality of Reporting of Metaanalyses (QUOROM) [6] and the Preferred Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA) revision [7] were adopted. Extracted data included publication date, location of study, length of follow up, patient inclusion and exclusion criteria, mean age, male and female proportion, schedule, dose and duration of chemoradiotherapy, morbidity related to therapy, restaging and surgical exploration/resection, histological status of surgical margins (R0 vs. R1/R2), and survival rates. Resectability was determined according to NCCN criteria [3]; if resectability criteria were not clearly stated, tumors were considered according to the stated resectability category. The results of our search and selection of studies are shown in Figure 1.
Figure 1. PRISMA 2009 flow diagram of our selection of studies.
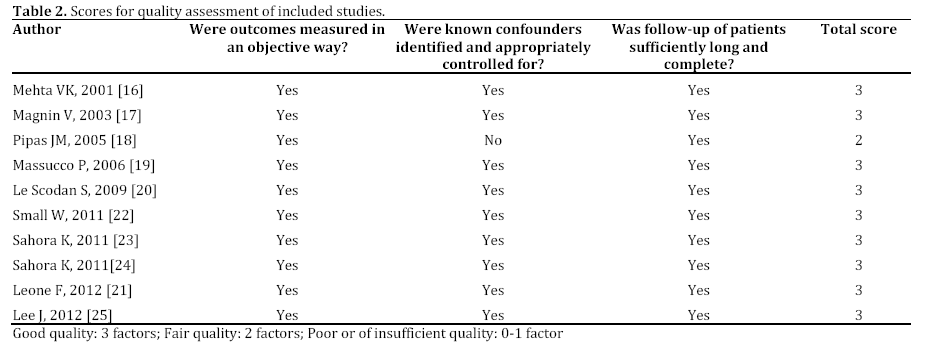
Methodological Quality Assessment
Quality of each study was evaluated by means of the Evidence Evaluation Process elaborated by the 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science, for assessing non randomized trials [8], which uses three quality items with a maximum score of 3 points. The quality terms are defined as “good” if they had all of the relevant quality items (score=3), “fair” if they had some of the items (score=2), and “poor” if they had only a few items but insufficient quality to include for further review (score=0-1).
Assessment of Bias Risk
Due to the risk of overestimating a beneficial intervention, we assessed the influence of the risk bias on our results by using the following domains: trial design (phase II and cohort studies), single or multi-institutional trials, sample size (cut-off: n=30), response criteria (Response Evaluation Criteria in Solid Tumors (RECIST) vs. all others) [9], resectability criteria (NCCN vs. all others), and therapeutic regimen (gemcitabine vs. other regimens as well as chemo/radiotherapy vs. chemotherapy alone).
Outcome Measures
Primary outcome was the proportion of patients explored, resected and of those with R0 margins. Secondary outcomes included survival, toxicity of therapies, and proportions of complete/partial response, stable disease, and progressive disease.
STATISTICS
Data were analyzed using the Comprehensive Meta- Analysis statistical software (version 1.0.25; Biostat, Englewood, NJ, USA) and were presented as proportions along with corresponding 95% confidence intervals (95% CIs), which were calculated by the Wilson score interval [10]. To estimate pooled proportions we used random rather than fixed effects models in order to take into account the heterogeneity of the estimates [11]. Statistical heterogeneity across studies was stated by using the Cochran’s test, and quantified by I2 (percentage of total variation across studies that is attributable to heterogeneity rather than chance) [12]; values were considered statistically significant when P was less than 0.1. Subgroup analyses were performed to identify possible sources of heterogeneity [13]. Bias of publication was assessed by Egger and Begg tests [14, 15].
RESULTS
We identified 4,337 references: 136 were duplicate records and 4,094 abstracts were excluded as being irrelevant. Of the 107 full articles retrieved for further assessment, 97 were excluded because they were retrospective trials (n=7), lacked institutionally approved protocols (n=3), included metastatic disease (n=82), or because separate data for borderline resectable disease were irretrievable (n=5). In total, 10 studies, published between 2001 and 2012, fulfilled the inclusion criteria [16, 17, 18, 19, 20, 21, 22, 23, 24, 25] (Figure 1).
Characteristics of Selected Studies (Table 1)
The reviewed trials included 182 patients. Seven studies originated from a single centre. Five of the studies selected were phase II trials, and the remaining were cohort studies run under a prospective design and with approved protocols.
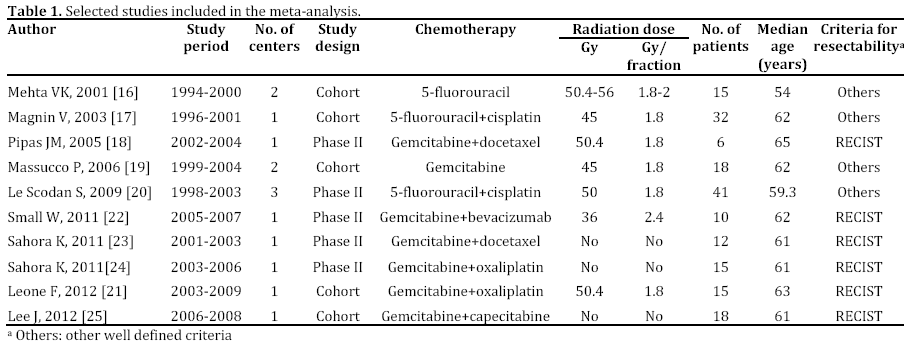
In seven studies, the protocols contemplated combination of radiotherapy with gemcitabine, provided as single agent or with other cytotoxic agents. In the remaining studies, 5-fluorouracil either alone or in combination with cisplatin was administered with radiotherapy. Radiotherapy was given at a dose ranging from 36 to 50.4 Gy with most patients receiving 1.8 Gy per fraction. In three studies no radiotherapy was provided.
According to quality evaluation, nine studies reached the score of 3 points (good quality), and one single trial only scored 2 points (fair quality) (Table 2)
Participants
The average age of the 182 patients was 61 years. All patients had a histological diagnosis of pancreatic adenocarcinoma. Three studies [16, 17, 20] enrolled exclusively patients with borderline resectable disease (n=88), whereas data for the remaining patients could be retrieved from the other trials on patients with mixed stages of disease [18, 19, 21, 22, 23, 24, 25]. Only two centers published more than one study, so the potential for an overlapping bias was minimal.
Exploration and Resection
Of the 180 restaged patients, the weighted frequency of those who underwent surgery was 69% (95% CI: 56-80%) (Figure 2 and Table 3); data were statistically heterogeneous (I2=59%; P=0.009). Four studies [18, 21, 22, 25] explicitly used the NCCN guidelines of resectability for pancreatic cancer [3]; 5 studies [16, 19, 20, 23, 24] followed different, but clearly defined, criteria and in a single study [17] criteria were ill-defined. For the 128 surgically explored patients, the estimated fraction of resected patients was 80% (95% CI: 66-90%) (Figure 3 and Table 3). Data across trials were homogeneous (I2=39%). Finally, for the 107 resected patients, the weighted proportion of R0 resection amounted to 83% (95% CI: 74-90%) (Figure 4). Data were homogeneous across the trials (I2=0%).
Figure 2. Estimates of surgical exploration proportions in
patients following neoadjuvant/pre-operative therapy and restaging.
Figure 3. Estimates of resection proportions in patients
following neoadjuvant/pre-operative therapy and re-staging.
Figure 4. Estimates of R0 resection proportions in patients
following neoadjuvant/pre-operative therapy and re-staging.
Tumor Response
Tumor response following neoadjuvant therapy was evaluated according the RECIST criteria [9] in 6 studies, whereas different, but clearly stated, criteria were used in the remaining studies. The weighted fraction of patients with complete/partial response at restaging (Figure 5 and Table 4) was 16% (95% CI: 9-28%); 69% (95% CI: 60-76%) of patients were documented to have stable lesions, and 19% (95% CI: 13-25%) a progressive disease. When previous figures were subjected to the analysis of heterogeneity, the respective I2 values equaled 48%, 15% and 0%, suggesting consistent homogeneity of data across the trials (Table 4).
Figure 5. Estimates of complete/partial response proportions in
patients following neoadjuvant/pre-operative therapy and restaging.
Toxicity
Grade 3-4 toxicity was estimated at 32% (95% CI: 21-45%) for all patients, with a corresponding I2 value of 58% (P=0.010) (Table 4). In the three studies where radiotherapy was not given, the gemcitabine plus docetaxel combination was associated with 46% rate of toxicity, and the gemcitabine plus oxaliplatin and gemcitabine plus capecitabine regimens with a rate of 30%.
Publication Bias
For all previous analyses, publication bias assessments, evaluated by the Egger’s regression intercept, were not significant.
Survival Analysis
Among studies reporting median survival rates [16, 17, 19, 20, 23, 24, 25], only a few included values for confidence intervals, P values, or analysis of variance were reported. Therefore, we were unable to run a meta-analysis of median survival times, and we simply calculated the mean of median survival times weighing by the number of patients at risk in each study. The weighted mean of median survival amounted to 12.4 months (range: 9 to 16 months) for the overall cohort of patients, 22.0 months (range: 12-32 months) for those who were resected, and 9.7 months (range: 8-41 months) for unresected patients. The weighted fractions of resected patients alive at 1 and 2 years were 61% (95% CI: 48-100%) and 44% (95% CI: 32-59%), respectively.
Analysis of Heterogeneity (Tables 3 and 4)
Although only a few meta-analytical results yielded data of moderate heterogeneity (I2>50%), multivariable meta-regression analyses for different variables were run to explore the likely sources of heterogeneity across the studies. For the complete/partial response at restaging, the only characteristic that could explain the heterogeneity was the sample size of the studies: small (≤30 patients) studies reported a downstaging rate higher than the rate reported in larger studies: 21% (95% CI: 12-33%) vs. 6% (95% CI: 1-26%). As compared to gemcitabine monotherapy, the administration of gemcitabine with other cytotoxic drugs tended to be associated with either higher downstaging rate and a lower progression rate: 22% (95% CI: 12-36%) vs. 9% (95% CI: 4-19%), and 12% (95% CI: 6-20%) vs. 24% (95% CI: 16- 34%).
The heterogeneity for the toxicity data could only be related to the different design of the included studies, with phase II studies reporting more severe toxicity than cohort studies: 46% (95% CI: 33-60) vs. 22% (95% CI: 14-35%) (P=0.011). In small-size studies patients were less likely to undergo surgical exploration than those evaluated in larger-size studies: 57% (95% CI: 44-69%) vs. 78% (95% CI: 65-87%) (P=0.024). Of relevance, higher rates of pancreatic resection were reported in cohort studies in comparison to the rates given in phase II studies: 91% (95% CI: 69-98%) vs. 72% (95% CI: 54-85%) (P=0.115).
DISCUSSION
The benefit of preoperative therapy for patients with pancreatic carcinoma is still unclear. Three recent meta-analyses [4, 5, 26] failed to support a benefit of neoadjuvant therapies. Gillen et al. [4] demonstrated that in resectable patients, neoadjuvant treatment did not impact on resectability, resection margins status or patients’ outcome, compared to upfront resection. On the contrary, in locally advanced patients, about 1/3 of the tumors became resectable at restaging. Our previous meta-analysis [5] did not support the benefit of preoperative therapy for patients with resectable lesions, and indicated a potential advantage only for a minority of those with unresectable cancers. On the same line, the metaanalysis by Assifi et al. [26] documented a benefit only for patients with locally advanced disease.
Current investigation considered only trials on patients with borderline resectable pancreatic adenocarcinoma who received neoadjuvant therapy, later restaged, and eventually resected. Relying on the results of the three previous meta-analyses [4, 5, 26], we were expecting neoadjuvant therapy to impact positively on the anatomic extent and overall outcome of patients. Contrary to our expectation, downstaging the lesion was accomplished in only 16% (95% CI: 9-28%) of the whole study cohort (Figure 5). Of more concern were data from large (>30 patients) size trials, where the weighted estimate of downstaging dropped to 6% (95% CI: 1-26%). The vast majority of patients with borderline resectable cancer had the lesion stable (69%; 95% CI: 60-76%) or progressive (19%; 95% CI: 13-25%) at restaging following neoadjuvant therapies. Thus, 2/3 of patients did not change his status, and 1/5 progressed despite therapy. On the basis of anatomic definitions of disease stage, this metaanalysis shows that radiographic downstaging is an uncommon event following neoadjuvant treatment, even among patients with borderline resectable disease, who had to experience significant (grade 3/4) toxicity in a considerable number of cases (32%; 95% CI: 21-45%). These data are in line with a recent study by Katz et al. [27] where a borderline resectable cancer was converted by preoperative therapy to a resectable lesion in only 1 of 129 evaluated patients.
Only a minority of patients with borderline resectable cancer were downstaged by therapy: whether this represents an actual benefit of preoperative chemoradiation or an over/under estimate of unresectability by cross-imaging at presurgical staging remains unclear. It is well known that current imaging modalities understage pancreatic cancers [28], as some patients undergo laparotomy but they have not resection because of local disease spread. The extent of over-staging of pancreatic cancers by preoperative computed tomography or magnetic resonance remains unknown and would be difficult to quantify, given that patients staged as locally advanced are denied surgery and consequently do not undergo objective verification of the preoperative staging.
A distinct advantage of this treatment approach is to allow selection for surgery of patients without disease progression. Presently, these two distinct groups of patients, i.e. those with progressive and those with non-progressive disease, cannot be differentiated at the time of diagnosis by current staging modalities. Efforts to separate these two categories by evaluating some biological characteristics of either the tumor or the patients seem most rewarding.
One major strength of the present study was the homogeneity of the meta-analytical data. In the most recent years, sub-categories of patients with borderline cancers in respect to the degree and type of vessel involvement have been delineated and emerged as a new issue to be taken into consideration when discussing therapies for patients with borderline resectable. Despite the definition of subcategories of borderline pancreatic cancers might have varied from one to the other study, our data resulted homogeneous at the statistical evaluation, indirectly suggesting a homogeneous definition of the borderline cancer stage, adopted in the selected studies. Notwithstanding that, two factors which could partly explain some differences appearing across the studies were identified: small size trials tended to either over-report the benefit of the preoperative treatment and to surgically explore less frequently patients; composite chemotherapeutic regimens seem to double the rate of complete/partial response without a significant increase in severe toxicity profile.
In summary, present investigation lends support to the results of previous meta-analyses showing that the promises of neoadjuvant therapies are partially fulfilled for either patients with resectable pancreatic cancers, for those initially deemed marginal for operative intervention, and for patients with truly locally-advanced disease. We acknowledge that marginally better results emerged from studies that administered combined chemo-radiotherapy over gemcitabine monotherapy, suggesting that the value of neoadjuvant therapies should be worth exploring in future trials with new chemotherapeutic drugs.
Conflict of interest
All the Authors state that this meta-analysis was designed and results were analyzed without financial support from producers of any drugs used in the study
References
- Varadhachary GR, Tamm EP, Abbruzzese JL, Xiong HQ, Crane CH, Wang H, et Al. Borderline resectable pancreatic cancer: definitions, management, and role of preoperative therapy. Ann Surg Oncol 2006;13:1035- 46.
- Callery MP, Chang KJ, Fishman EK, Talamonti MS, William Traverso L, Linehan DC. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: expert consensus statement. Ann Surg Oncol 2009;16:1727-33.
- National Comprehensive Cancer Network (NCCN) guidelines. Available at: www.nccn.org (Accessed on October 13, 2011).
- Gillen S, Schuster T, Meyer Zum Büschenfelde C, Friess H, Kleeff J. Preoperative/neoadjuvant therapy in pancreatic cancer: a systematic review and meta-analysis of response and resection percentages. PLoS Med 2010;7(4):e1000267.
- Andriulli A, Festa V, Botteri E, Valvano MR, Koch M, Bassi C, et Al.Neoadjuvant/Preoperative Gemcitabine for Patients with Localized Pancreatic Cancer: A Meta-analysis of Prospective Studies. Ann Surg Oncol 2012;19:1644-62.
- Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Quality of Reporting of Meta-analyses. Lancet 1999;354:1896–1900.
- Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097
- Morley PT, Atkins DL, Billi JE, Bossaert L, Callaway CW, de Caen AR, et Al. Part 3: Evidence evaluation process: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122 (16 Suppl 2):S283-90.
- Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et Al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000,92:205-216.
- Wilson E.B. Probable inference, the law of succession, and statistical inference. J Am Stat Ass 1927; 22: 209–212.
- Greenland S. Quantitative methods in the review of epidemiologic literature. Epidemiol Rev. 1987; 9:1-30.
- Higgings JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539-1558.
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629-34.
- Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50:1088–101.
- van Houwelingen HC, Arends LR, Stijnen T. Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med 2002;21:589–624.
- Mehta VK, Fisher G, Ford JA, Poen JC, Vierra MA, Oberhelman H, et al. Preoperative chemoradiation for marginally resectable adenocarcinoma of the pancreas. J Gastrointest Surg 2001;5:27-35.
- Magnin V, Moutardier V, Giovannini MH, Lelong B, Giovannini M, Viret F, et Al. Neoadjuvant preoperative chemoradiation in patients with pancreatic cancer. Int J Radiat Oncol Biol Phys 2003;55:1300-4.
- Pipas JM, Barth RJ Jr, Zaki B, Tsapakos MJ, Suriawinata AA, Bettmann MA, et Al. Docetaxel/Gemcitabine followed by gemcitabine and external beam radiotherapy in patients with pancreatic adenocarcinoma. Ann Surg Oncol 2005;12:995-1004.
- Massucco P, Capussotti L, Magnino A, Sperti E, Gatti M, Muratore A, et Al. Pancreatic resections after chemoradiotherapy for locally advanced ductal adenocarcinoma: analysis of perioperative outcome and survival. Ann Surg Oncol 2006;13:1201-8.
- Le Scodan R, Mornex F, Girard N, Mercier C, Valette PJ, Ychou M, et Al. Preoperative chemoradiation in potentially resectable pancreatic adenocarcinoma: feasibility, treatment effect evaluation and prognostic factors, analysis of the SFRO-FFCD 9704 trial and literature review. Ann Oncol 2009;20:1387-96.
- Leone F, Gatti M, Massucco P, Colombi F, Sperti E, Campanella D, et Al. Induction gemcitabine and oxaliplatin therapy followed by a twice-weekly infusion of gemcitabine and concurrent external-beam radiation for neoadjuvant treatment of locally advanced pancreatic cancer: A single institutional experience. Cancer. 2012 Jul 6. doi: 10.1002/cncr.27736. [Epub ahead of print]
- Small W Jr, Mulcahy MF, Rademaker A, Bentrem DJ, Benson AB, Weitner BB, et Al. Phase II trial of full-dose gemcitabine and bevacizumab in combination with attenuated three-dimensional conformal radiotherapy in patients with localized pancreatic cancer. Int J Radiat Oncol Biol Phys 2011;80:476-82.
- Sahora K, Kuehrer I, Schindl M, Koelblinger C, Goetzinger P, Gnant M. NeoGemTax: gemcitabine and docetaxel as neoadjuvant treatment for locally advanced nonmetastasized pancreatic cancer. World J Surg 2011;35:1580-9.
- Sahora K, Kuehrer I, Eisenhut A, Akan B, Koellblinger C, Goetzinger P, et Al. NeoGemOx: Gemcitabine and oxaliplatin as neoadjuvant treatment for locally advanced, nonmetastasized pancreatic cancer. Surgery 2011;149:311-20.
- Lee JL, Kim SC, Kim JH, Lee SS, Kim TW, Park DH, et Al. Prospective efficacy and safety study of neoadjuvant gemcitabine with capecitabine combination chemotherapy for borderline-resectable or unresectable locally advanced pancreatic adenocarcinoma. Surgery 2012 Jun 6. [Epub ahead of print]
- Assifi MM, Lu X, Eibl G, Reber HA, Li G, Hines OJ. Neoadjuvant therapy in pancreatic adenocarcinoma: a meta-analysis of phase II trials. Surgery 2011;150:466-73.
- Katz MHG, Fleming JB, Bhosale P, Varadhachary G, Lee JE, Wolff R, et Al. Response of borderline resectable pancreatic cancer to neoadjuvant therapy is not reflected by radiographic indicators. Cancer 2012 May 17. [Epub ahead of print]
- Zhang Y, Huang J, Chen M, Jiao LR. Preoperative vascular evaluation with computed tomography and magnetic resonance imaging for pancreatic cancer: A meta-analysis. Pancreatology 2012;12:227-33.






