Keywords
Neonatal; Congenital heart disease; Emergencies
Presentation of Neonate with Congenital Heart Disease
The timing of presentation and severity depends on
1. Nature and severity of defect
2. The alteration in cardiovascular physiology secondary to the effect of the transitional circulation as
a) Closure of ductus / restriction of patent foramen ovale (PFO)
b) Fall in pulmonary vascular resistance (PVR)
Structural heart disease presenting as cardiac emergency in neonatal period can be broadly categorized into:
Ductal dependent circulations
In a normal neonate ductus use to close in the first few days of life without causing any hemodynamic compromise. In neonates with heart disease requiring ductul flow for survival, closure or constriction of ductus may be associated with profound circulatory compromise. Ductul dependent congenital heart diseases (CHD) requiring patency of ductus are:-
A) To maintain adequate systemic blood flow in left sided obstructive lesions
• Critical aortic stenosis
• Severe coarctation of aorta / Interrupted aortic arch
• Hypoplastic left heart syndrome.
B) To maintain adequate pulmonary blood flow with right sided obstructive lesions
• Critical pulmonary stenosis / pulmonary atresia with intact ventricular septum
• Pulmonary atresia with ventricular septal defect
• Tricuspid atresia with pulmonary atresia
• Univentricular heart with pulmonary atresia
• Severe Ebstein’s anomaly of tricuspid valve(functional pulmonary atresia)
C) To ensure adequate mixing as in conditions with parallel circulation
• Transposition of great vessels
Restriction at foramen ovale
Wide open atrial communication is require to maintain hemodyanamic stability in new-born with certain heart defects as:-
A) To relieve pulmonary congestion in
• Hypoplastic left heart
• Mitral stenosis / atresia
B) To relief right sided congestion and maintain systemic blood flow in
• Pulmonary atresia with intact septum
• Tricuspid atresia
• Total anomalous pulmonary venous connection (TAPVC)
Obstructed Total anomalous pulmonary venous connection
Presents as surgical cardiac emergency in neonatal period.
The pediatrician or neonatologist, if familiar with the clinical manifestations of these circulatory changes, is in better position to organize prompt stabilization and early referral so that a speedy medical, catheter intervention or surgical solution whenever possible can be instituted.
Pulse oximetry and an arterial blood gas determination should be performed initially on room air to serve baseline. Subsequent measurements should be obtained on 100% oxygen and may help to differentiate between cardiogenic and non-cardiogenic causes of cyanosis. Neonates with neurogenic or primary pulmonary causes of cyanosis demonstrate substantial rise in partial pressure of oxygen (pO2 > 250 mmHg) in both upper and lower extremities. This virtually eliminates critical structural cyanotic heart disease. An arterial pO2 of less than 100 mmHg in the absence of lung disease is most likely to be due to intracardiac right to left shunting and is virtually diagnostic of congenital cyanotic heart disease involving ductal dependent systemic or pulmonary blood flow, and should receive prostaglandin infusion until anatomic definition can be accomplished [1, 2]. Patients who have an arterial pO2 between 100 and 250 mmHg may have structural heart disease classified as admixture lesions with increased pulmonary blood flow [2].
Neonate Presenting with Circulatory Collapse
These are the congenital heart defects where systemic circulation is dependent on the patency of the ductus arteriosus for survival. All these patients typically present in cardiovascular collapse as the ductus arteriosus closes / constricts, with resulting systemic hypoperfusion [3]. Although all infants with significant left sided obstructive lesions and ductal dependent systemic blood flow require prostaglandin infusion to maintain patency of ductus arteriosus as initial part of management, additional care varies with each lesion.
Critical aortic stenosis
Patients with critical aortic stenosis have severe obstruction present in utero with accompanying left ventricular hypertrophy and endocardial fibroelastosis. After birth, with ductal closure left ventricle has to maintain systemic blood flow, this acute increase in after load causes left ventricle function to compromise, with severe myocardial dysfunction, clinical congestive heart failure or shock will become apparent. The less severe forms present later in life.
Critical coarctation
Critical narrowing of the aortic isthmus in the new born results in the lower body becoming duct dependent, upper part of body is unaffected by duct closure. It is believed that some of the ductal tissue that surrounds the aorta in the region of coarctation, may also constrict along with the closing ductus and may actually increase the severity of the coarctation. Additional cardiac abnormalities are common, including bicuspid aortic valve (about 80%), and ventricular septal defect (40%). The spectrum of severity varies, as with aortic stenosis, milder forms present later in life.
Aortic arch interruption
Arch interruption is usually associated with major intracardiac defect as ventricular septal defect, truncus arteriosus, transposition complex with ventricular septal defect (VSD), double outlet right ventricle with subpulmonary VSD. The hemodyanamics are similar to critical coarctation of aorta.
Hypoplastic left heart syndrome
All the left sided structures including mitral valve apparatus, left ventricle, ascending aorta, arch are too small to maintain entire systemic output. As a result the entire systemic output is dependent on the right side of heart and the patency of ductus arteriosus (PDA).
Diagnosis
Clinical scenario-Heart failure / shock in first two weeks of life
Physical examination
• Reduced peripheral pulses
• All limbs-Critical aortic stenosis (AS) / hypoplastic left heart syndrome (HLHS)
• Reduced femoral pulses-Coarctation / Interruption
• Mild cyanosis-Single ventricle physiology (HLHS)
• Single second heart sound
Electrocardiography
• Right ventricular hypertrophy
• Left ventricular hypertrophy with strain (critical AS)
• Poor / absence of left ventricle forces (HLHS)
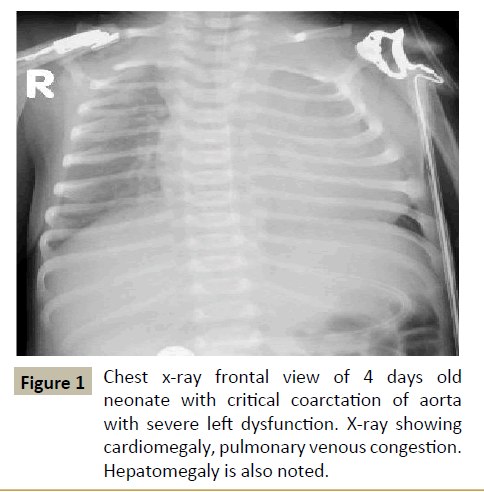
Figure 1: Chest x-ray frontal view of 4 days old neonate with critical coarctation of aorta with severe left dysfunction. X-ray showing cardiomegaly, pulmonary venous congestion. Hepatomegaly is also noted.
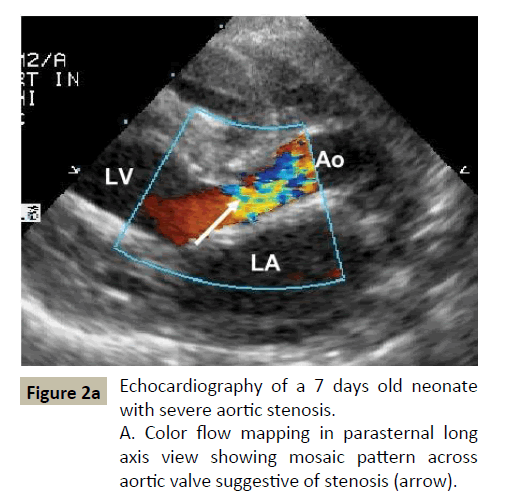
Figure 2a:Echocardiography of a 7 days old neonate with severe aortic stenosis.
A. Color flow mapping in parasternal long axis view showing mosaic pattern across aortic valve suggestive of stenosis (arrow).
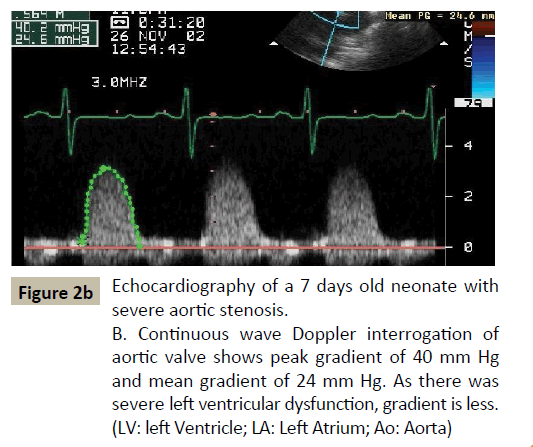
Figure 2b:Echocardiography of a 7 days old neonate with severe aortic stenosis.
B. Continuous wave Doppler interrogation of aortic valve shows peak gradient of 40 mm Hg and mean gradient of 24 mm Hg. As there was severe left ventricular dysfunction, gradient is less. (LV: left Ventricle; LA: Left Atrium; Ao: Aorta).
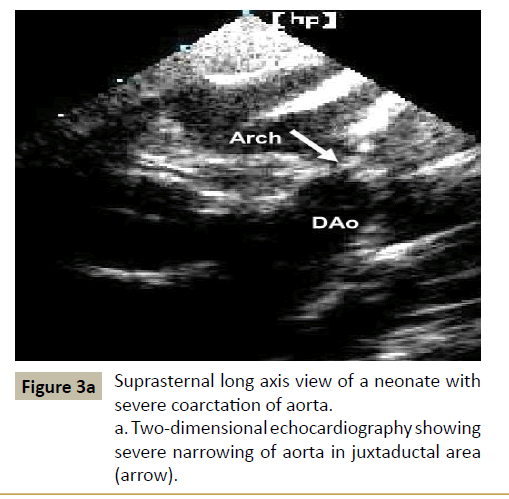
Figure 3a:Suprasternal long axis view of a neonate with severe coarctation of aorta.
a. Two-dimensional echocardiography showing severe narrowing of aorta in juxtaductal area (arrow).
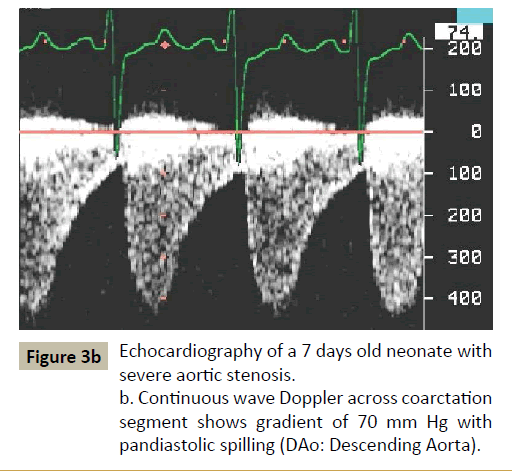
Figure 3b:Echocardiography of a 7 days old neonate with severe aortic stenosis.
b. Continuous wave Doppler across coarctation segment shows gradient of 70 mm Hg with pandiastolic spilling (DAo: Descending Aorta).
Chest x-ray (Figure 1)
• Cardiomegaly
• Pulmonary venous hypertension
• Increased pulmonary blood flow with HLHS
Echocardiography-Echocardiography plays crucial role in establishing the diagnosis, its severity, hemodynamic effects as pulmonary artery pressure and ventricular dysfunction (Figures 2a, 2b, 3a, 3b and 4).
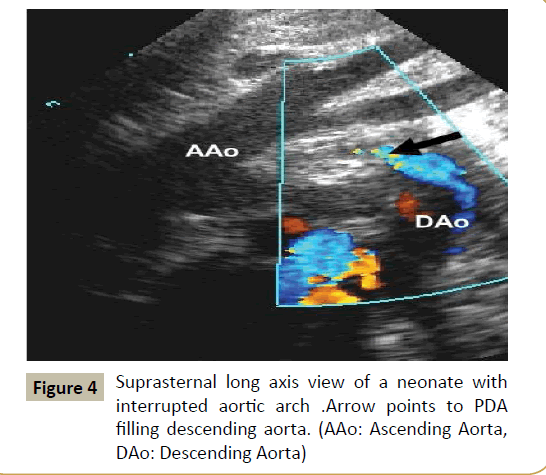
Figure 4:Suprasternal long axis view of a neonate with interrupted aortic arch .Arrow points to PDA filling descending aorta. (AAo: Ascending Aorta, DAo: Descending Aorta).
Management
Initial management of the severely affected new-born includes treatment of shock, stable vascular access, and attention to airway and breathing, correction of metabolic acidosis. These babies should be started on prostaglandin E1 infusion. The initial dose of PGE1 is 0.05 mcg/kg/minute continuous intravenous infusion; the dose may be increased to 0.1 mcg/kg/minute if desired effect is not obtained within ten minutes. Once the desired effect is obtained the doses may be reduced to 0.01 mcg/kg/minute. PGE1 causes apnea in 10-12% of cases, usually within 6 hrs of infusion, continuous cardiorespiratory monitoring is required during infusion. Other adverse effects include fever (14%), cutaneous flush (10%), bradycardia (7%), seizures (4%), cardiac arrest (1%), and edema (1%) are uncommon [4].
Until a definitive procedure is planned, it is important to maintain a balance between systemic and pulmonary blood flow and it is important to avoid any maneuver that reduces pulmonary vascular resistance because systemic perfusion is dependent on pulmonary vascular resistance (PVR). These include avoidance of hyperventilation (pO2=40-50 mmHg, oxygen saturation in range of 70-80%) and injudicious use of ionotropes which will increase systemic vascular resistance (SVR).
Definitive treatment
In neonates with critical aortic stenosis who presents as duct dependent systemic circulation, after initial stabilization, echocardiography should be done to assess left ventricle size to determine its adequacy to sustain systemic circulation. If yes, balloon dilatation of aortic valve is treatment of choice [5].
For new born with coarctation of aorta, surgery is treatment of choice, but if baby is having additional problem i.e. sepsis, multiorgan dysfunction, then balloon dilatation is an alternative. Balloon dilation gives immediate good result however there is an extremely high risk of restenosis (> 80%) [6]. For newborn with arch interruption surgery is only available option.
The treatment options for newborn with hypoplastic left heart include, staged surgery for Norwood operation and cardiac transplantation [7-9].
Neonates Presenting with Cyanosis
Duct dependent pulmonary circulation
This group includes newborn presenting with cyanosis which if unrecognized leads to severe hypoxemia, metabolic acidosis and finally death. Systemic perfusion is usually maintained till the very end. The rapidity of progression of disease is partly dependent on how soon and severely the pulmonary blood flow is compromised with ductal closure. This group consist of newborn where there is anatomical / functional discontinuity between ventricle and pulmonary artery, ductul patency is required to maintain pulmonary flow, except in patients with multiple aortopulmonary collateral’s.
Pulmonary atresia or severe stenosis of pulmonary blood flow: The condition is well tolerated in utero. After birth, with fall in PVR, pulmonary blood flow is sustained through the PDA. With ductal closure / restriction the baby become deeply cyanosed, develops metabolic acidosis and if left untreated may die. Rarely flow through the duct remains unrestricted and the child present with heart failure with minimal cyanosis, later as the PVR falls.
Ebstein’s anomaly of tricuspid valve: Severe tricuspid regurgitation causes failure of forward flow through the pulmonary valve. In neonatal period as pulmonary artery pressure is high so pulmonary valve fails to open causing functional pulmonary atresia. With fall in pulmonary artery pressure and PVR, pulmonary valve opens maintaining forward flow and decrease in tricuspid regurgitation causing improvement in baby’s condition.
Diagnosis
• Clinical scenario
• Cyanosis
Physical examination
• Quiet precordium
• No significant murmur, rarely continuous murmur of PDA
• Single second heart sound
Arterial blood gas
• Metabolic acidosis, low pO2, normal pCO2, failure of 100% oxygen to increase pO2 > 100 mmHg
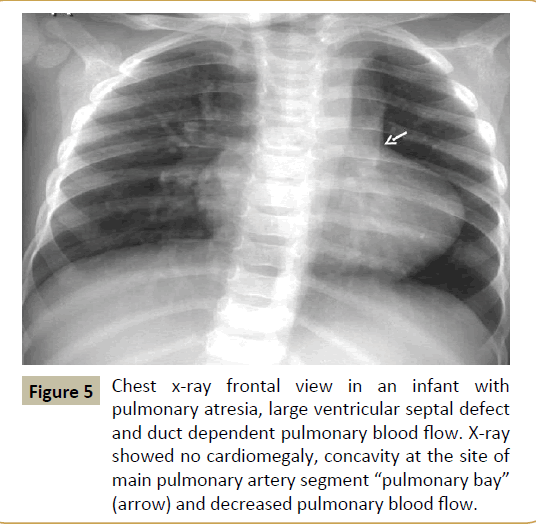
Figure 5:Chest x-ray frontal view in an infant with pulmonary atresia, large ventricular septal defect and duct dependent pulmonary blood flow. X-ray showed no cardiomegaly, concavity at the site of main pulmonary artery segment “pulmonary bay” (arrow) and decreased pulmonary blood flow.
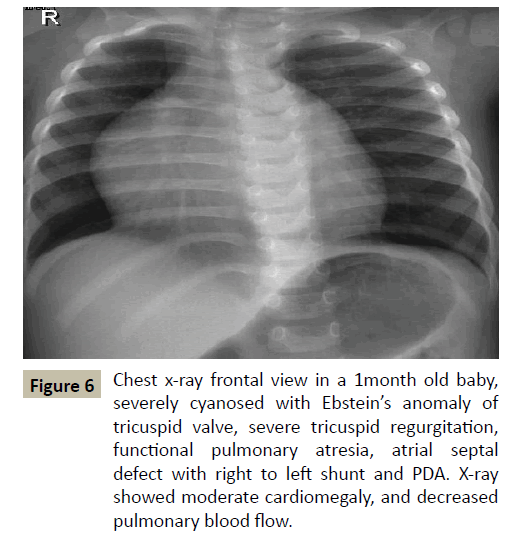
Figure 6:Chest x-ray frontal view in a 1month old baby, severely cyanosed with Ebstein’s anomaly of tricuspid valve, severe tricuspid regurgitation, functional pulmonary atresia, atrial septal defect with right to left shunt and PDA. X-ray showed moderate cardiomegaly, and decreased pulmonary blood flow.
Chest X-Ray (Figures 5 and 6)
• Absence of cardiomegaly except when there is associated valvar regurgitation as dysplastic tricuspid valve and in Ebstein’s anomaly
• Dark lung fields
• Absence of main pulmonary artery segment segment
Electrocardiography
• Right axis deviation
• Right ventricular forces
• Except-Tricuspid atresia with hypoplastic right ventricle- left axis deviation with left ventricle forces.
• Ebstein’s anomaly-Tall P wave, low voltage QRS complexes, conduction defects.
Echocardiography
This is mainstay of diagnosis which define the basic anatomy, status of ductus (Figures 7a and 7b). Depending on size of right ventricle further plan about two ventricle repair or single ventricle repair can be decided.
Management: The guidelines for management of a newborn with cyanosis are as follows:
Establish the accurate anatomical diagnosis by echocardiography. In the absence of that, at least physiological diagnosis should be made with the combination of clinical, electrocardiography, chest X-ray, and blood gas with hyperoxia test. Correction of metabolic abnormalities as acidosis, dehydration, hypoglycemia.
Temperature maintenance: If the saturation dropped below 70%, the baby should be started on PGE1 infusion (doses and side effects described earlier). PGE1 infusion can be given even before the complete anatomical diagnosis is established in all cyanotic newborn
Ionotropic agents are rarely required. Some routinely start a combination of renal doses of Dopamine (3-5 mcg/kg/minute) to increase renal perfusion and Dobutamine (5 mcg/kg/minute) as an ionotrope to correct myocardial depressant effect of severe metabolic acidosis.
Feeding: The severely hypoxic and acidotic newborn should be kept Figure 6 Chest x-ray frontal view in a 1month old baby, severely nil orally till stabilization. While the baby on PGE1 infusion wide open ductus causes steal phenomena in gut vessels predisposing it for risk of necrotizing enterocolitis. In view of this while the baby is on PGE1 infusion oral feeding should be avoided.
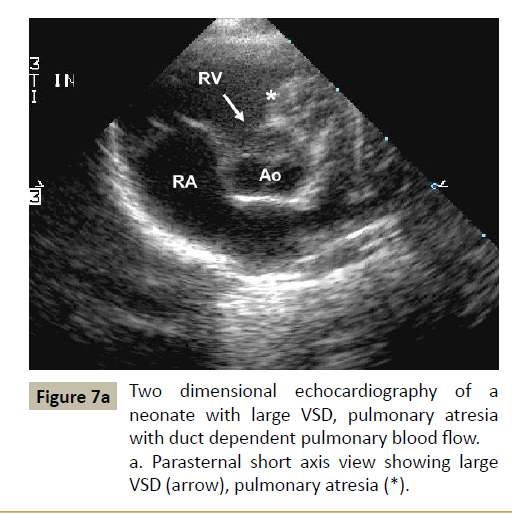
Figure 7a:Two dimensional echocardiography of a neonate with large VSD, pulmonary atresia with duct dependent pulmonary blood flow. a. Parasternal short axis view showing large VSD (arrow), pulmonary atresia (*).
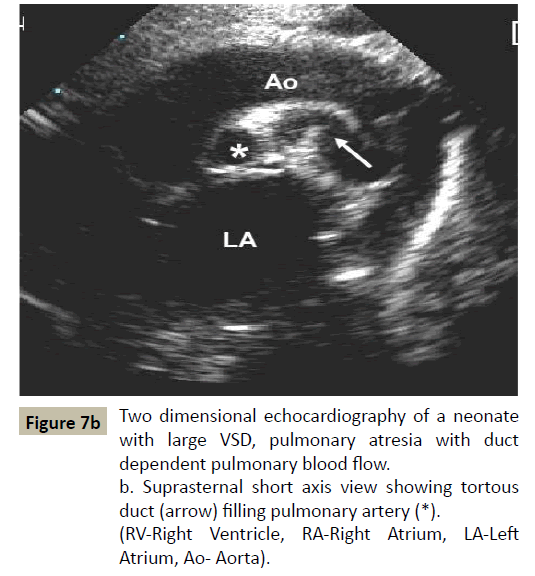
Figure 7b:Two dimensional echocardiography of a neonate with large VSD, pulmonary atresia with duct dependent pulmonary blood flow.
b. Suprasternal short axis view showing tortous duct (arrow) filling pulmonary artery (*). (RV-Right Ventricle, RA-Right Atrium, LA-Left Atrium, Ao- Aorta).
Definitive treatment
a) Critical pulmonary stenosis
Balloon pulmonary valvotomy is treatment of choice [10].
b) Pulmonary atresia with intact ventricular septum
Definitive management of it depends upon size of right ventricle and coronary circulation (whether RV dependent or not). If right ventricle is of adequate size than opening of right ventricle outflow tract (RVOT) by surgery or catheter intervention is treatment of choice [11]. In some neonates when right ventricle is borderline, one needs additional source of pulmonary blood flow in form of Blalock-Taussig shunt or ductal stenting after balloon dilatation of pulmonary valve [12, 13]. In patients with hypoplastic right ventricle or right ventricle coronary circulation, baby becomes candidate for single ventricular physiology [14].
In Pulmonary atresia / critical pulmonary stenosis with ventricular septal defect-Blalock Taussig operation followed by total correction at later age is the treatment plan [14].
Transposition complex
Complete transposition of great vessels (d-TGA) is a complex group of condition, wherein severe hypoxemia occurs as a result of peculiar anatomical connection. Systemic venous (deoxygenated) blood return to right side of heart and goes to systemic circulation as aorta arises from right ventricle while pulmonary venous return (oxygenated blood) goes again to pulmonary circulation as pulmonary arteries arises from left ventricle. This does not cause any deleterious effect on fetal wellbeing but after birth for survival there has to be adequate mixing between these circulation, intracardiac (atrial septal defect / PFO or VSD) or extra cardiac (PDA / collaterals). This mixing actually determines the clinical presentation, prognosis and management.
Transposition complexes have been grouped as:
a) Transposition of great vessels with poor mixing (intact ventricular septum or restrictive VSD)- These babies usually presents in neonatal period with severe hypoxemia occuring after ductal closure. The atrial communication which is usually a PFO, is also restrictive and will not be able to maintain adequate mixing.
b) Transposition with adequate mixing- Patients with VSD / PDA presents with congestive heart failure (CHF) at 4-6 weeks with mild cyanosis as ventricular septal defect / patent ductus acts as site of adequate mixing with increase pulmonary blood flow. These patients are at high risk for early development of pulmonary vascular disease as early as 8 weeks of age, but usually do not present in neonatal period with symptoms.
d-TGA with large atrial septal defect (ASD) has most favourable presentation as ASD act as a site of adequate mixing without causing pulmonary hypertension, and as ASD is low pressure site of mixing the chances of CHF and development of pulmonary edema are low.
c) Transposition with VSD / pulmonary stenosis physiology- This subset presents beyond the neonatal period as tetralogy of Fallot but cyanosis is deeper and presentation is earlier in comparison to tetralogy of Fallot (TOF).
Diagnosis
Clinical scenario:
Cyanosis
Features of CHF with large VSD / PDA:
• Physical examination
• Quiet precordium
• Single second heart sound
• No significant murmur, rarely continuous murmur of PDA
• Arterial blood gas- Metabolic acidosis, low pO2,normal pCO2,failure of 100% oxygen to increase pO2 > 100 mm Hg
Chest x-ray (Figure 8):
Unremarkable at birth, typical egg on side appearance evolves over a period of few days.
Cardiomegaly with increased pulmonary blood flow in TGA with large VSD
Increase pulmonary blood flow along with evidence of pulmonary venous congestion in patients with d-TGA, VSD with restrictive atrial communication.
Electrocardiography: Right axis deviation, right ventricle forces.
Echocardiography: Definitive tool of diagnosis and defines the anatomical connections, site of mixing and associated defects (Figures 9a and 9b).
Management
Treatment strategies include: Initial stabilization with correction of metabolic derangement including temperature maintenance, treatment of hypoglycemia, correction of acidosis.
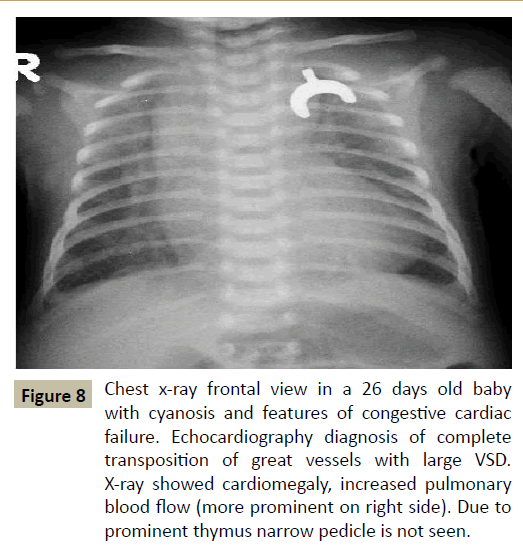
Figure 8:Chest x-ray frontal view in a 26 days old baby with cyanosis and features of congestive cardiac failure. Echocardiography diagnosis of complete transposition of great vessels with large VSD. X-ray showed cardiomegaly, increased pulmonary blood flow (more prominent on right side). Due to prominent thymus narrow pedicle is not seen.
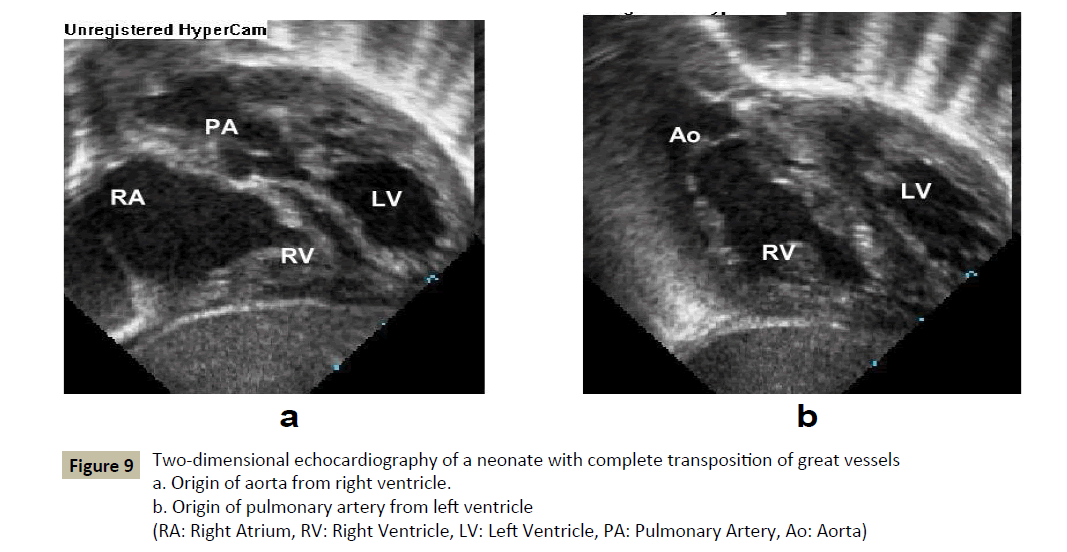
Figure 9:Two-dimensional echocardiography of a neonate with complete transposition of great vessels
a. Origin of aorta from right ventricle.
b. Origin of pulmonary artery from left ventricle
(RA: Right Atrium, RV: Right Ventricle, LV: Left Ventricle, PA: Pulmonary Artery, Ao: Aorta)
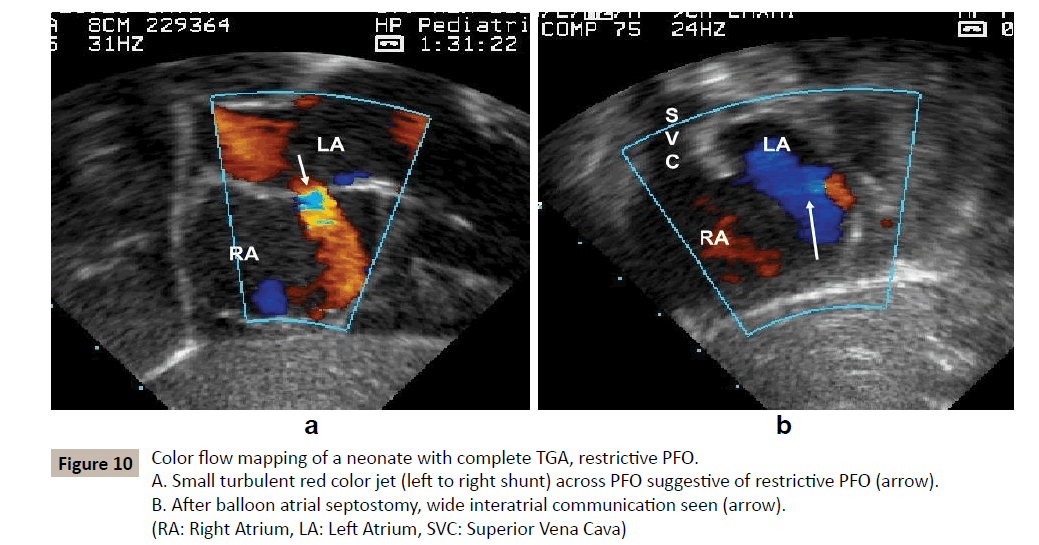
Figure 10:Color flow mapping of a neonate with complete TGA, restrictive PFO. A. Small turbulent red color jet (left to right shunt) across PFO suggestive of restrictive PFO (arrow). B. After balloon atrial septostomy, wide interatrial communication seen (arrow). (RA: Right Atrium, LA: Left Atrium, SVC: Superior Vena Cava).
Prostaglandin is life saving and should be started as soon as baby is diagnosed as having congenital cyanotic heart disease without waiting for the morphological diagnosis
Palliation-Balloon atrial septostomy should be performed in patients with restrictive PFO with intact ventricular septum as well as with VSD. In babies with VSD, septostomy is not an emergency procedure as with intact ventricular septum (Figures 10a and 10b).
Septostomy serves the following purposes: If septostomy is adequate, Prostaglandin infusion can be withdrawn which is a potentially harmful drug.
In patients with VSD or babies on Prostaglandin infusion, septostomy helps to relieve left atrial pressure and pulmonary venous congestion, further causing improvement in oxygenation.
In rare instances when arterial switch cannot be performed because of sepsis or centers not practicing arterial switch, it is essential to palliate the child beyond the age of 8 weeks till the alternative atrial switch can be performed.
Definitive treatment: Arterial switch is the operation of choice, which should be performed within 2 weeks, maximum by 4 weeks [15]. In late presenters (beyond 4 weeks of age), currently, the 3 main options proposed in this situation are: a) preparatory surgery using pulmonary artery banding and BT shunt, followed by arterial switch in a second stage [16, 17]; b) arterial switch with ECMO support until ventricular remodeling occurs [18, 19]; c) discharge of the patient and atrial switch operation (Senning, Mustard) after a few months [19, 20].
Obstructed total Anomalous Pulmonary Venous
Connection
The pulmonary veins are anomalously connected to right side of heart (as superior vena cava, Vertical vein, coronary sinus, directly to right atrium, inferior vena cava or a combination of these), only source of blood flow to left side is through interatrial communication. If the pathway from pulmonary veins to left atrium is unobstructed, the child presents with features of CHF beyond the neonatal period with mild cyanosis. However if there is obstruction in this pathway, which is always with infradiaphragmatic TAPVC and about one third of cases to superior vena cava, than child presents on day 1 or 2 of life with cyanosis and respiratory distress.
The obstruction to pulmonary venous pathway leads to:
• Pulmonary arterial and pulmonary venous hypertension
• Severely restricted pulmonary blood flow
If there is wide open ductus, pulmonary blood flow further compromises as PDA causes R-L shunting at ductul level causing hypoxia. This is one cardiac emergency wherein prostaglandins will not benefit the neonate and may cause further deterioration in condition.
Diagnosis
Clinical scenario:
• Cyanotic newborn, with tachypnea and CHF
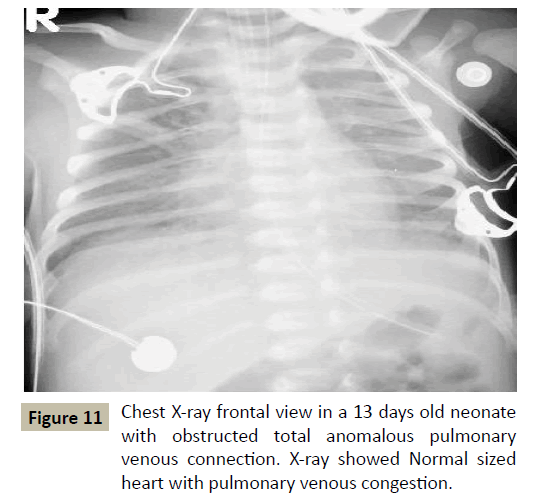
Figure 11: Chest X-ray frontal view in a 13 days old neonate with obstructed total anomalous pulmonary venous connection. X-ray showed Normal sized heart with pulmonary venous congestion.
• Physical examination
• No cardiomegaly
• Loud P2
• Continuous murmur- venous hum, ejection systolic murmur
• Arterial blood gases- Metabolic acidosis, low pO2,normal or elevated pCO2, failure of 100% oxygen to increase pO2 > 100 mmHg
Chest x-ray (Figure 11):
• Absence of cardiomegaly
• Prominent pulmonary artery segment
• Hazy lung fields-pulmonary edema (this may mimic the X-ray chest finding of neonatal respiratory distress syndrome).
Electrocardiography: Not specific
• Right axis deviation with RV forces
• May get right atrial enlargement
Echocardiography- Diagnostic which reveals site of anomalous connection and level of obstruction (Figures 12a and 12b).
It is imperative that in all patients diagnosed as so called primary hypertension in neonatal ICU, should have a very strong suspicion of obstructed TAPVC
Management: Immediate surgical correction of the defect is the treatment of choice.
Neonatal Heart Failure
Some neonates present with features of congestive heart failure in insidious manner. Causes of neonatal CHF can be congenital heart disease or acquired:
Congenital
Heart failure with mild cyanosis (Admixture lesions)
A) Truncus arteriosus:
• Single ventricle physiology without pulmonary stenosis
• Large left to right shunt
B) Large VSD:
• Complete atrioventricular canal defect with valve regurgitation
• Large PDA / Aortopulmonary window
C) Arteriovenous malformations:
• Especially vein of Galen malformation
• Anomalous origin of pulmonary artery from ascending aorta
• Tetralogy of Fallot with absent pulmonary valve syndrome
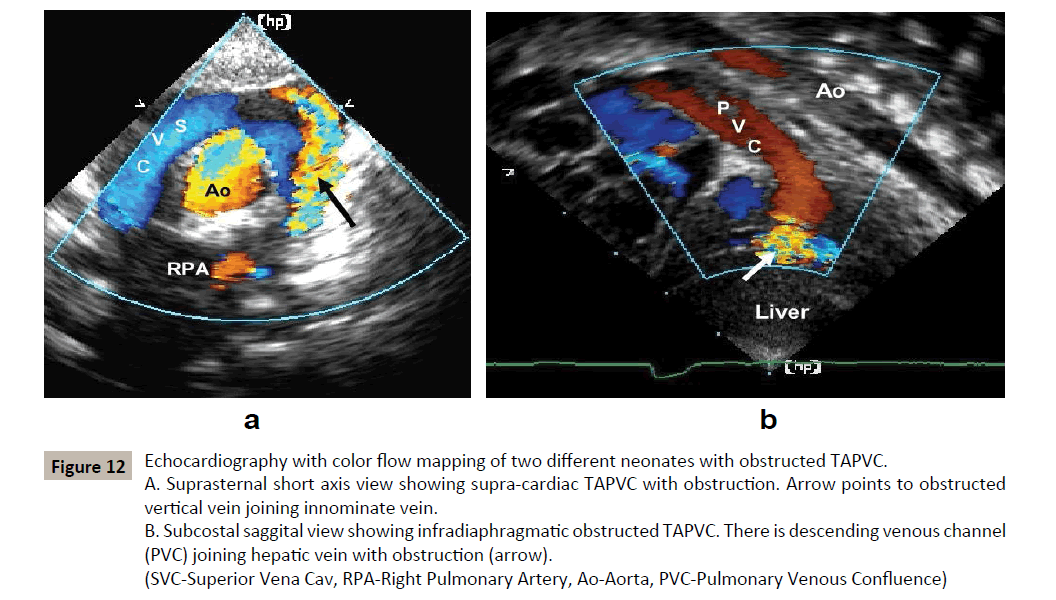
Figure 12:Echocardiography with color flow mapping of two different neonates with obstructed TAPVC. A. Suprasternal short axis view showing supra-cardiac TAPVC with obstruction. Arrow points to obstructed vertical vein joining innominate vein.
B. Subcostal saggital view showing infradiaphragmatic obstructed TAPVC. There is descending venous channel (PVC) joining hepatic vein with obstruction (arrow).
(SVC-Superior Vena Cav, RPA-Right Pulmonary Artery, Ao-Aorta, PVC-Pulmonary Venous Confluence)
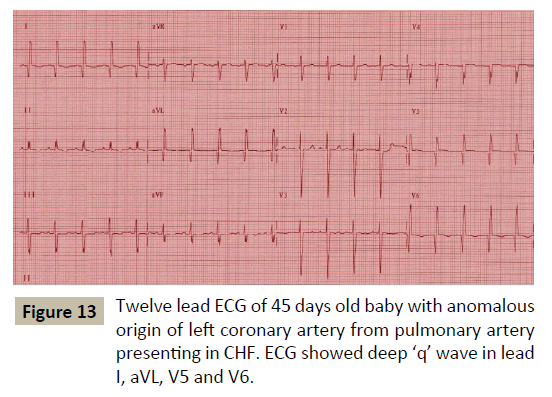
Figure 13:Twelve lead ECG of 45 days old baby with anomalous origin of left coronary artery from pulmonary artery presenting in CHF. ECG showed deep ‘q’ wave in lead I, aVL, V5 and V6.
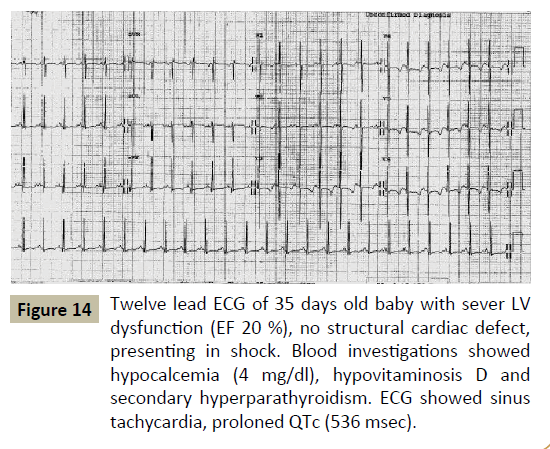
Figure 14:Twelve lead ECG of 35 days old baby with sever LV dysfunction (EF 20 %), no structural cardiac defect, presenting in shock. Blood investigations showed hypocalcemia (4 mg/dl), hypovitaminosis D and secondary hyperparathyroidism. ECG showed sinus tachycardia, proloned QTc (536 msec).
D) LV dysfunction:
Anomalous origin of left coronary artery from pulmonary artery (Figure 13).
Acquired
• Acquired ventricular dysfunction secondary to:
• Myocarditis
• Dilated cardiomyopathy
• Septicemia
• Metabolic causes-Hypoglycemia, hypocalcemia (Figure 14)
• Asphyxia
• Arrhythmias (Figures 15 and 16)
Neonate with septal defects usually presents between 2-8 weeks of age with CHF due to pulmonary overcirculation as there is fall in pulmonary vascular resistance causing increase in pulmonary blood flow, rarely there can be an early presentation as in preterm child where precipitous fall in PVR occurs causing large left to right shunt. In any newborn presenting with CHF, one should always look for other causes contributing to heart failure in addition to septal defects as:
A. Associated obstructive lesion specially coarctation of aorta, interrupted aortic arch or rarely aortic stenosis.
B. Multiple levels of shunts, e.g. at atrial, ventricular and great artery level
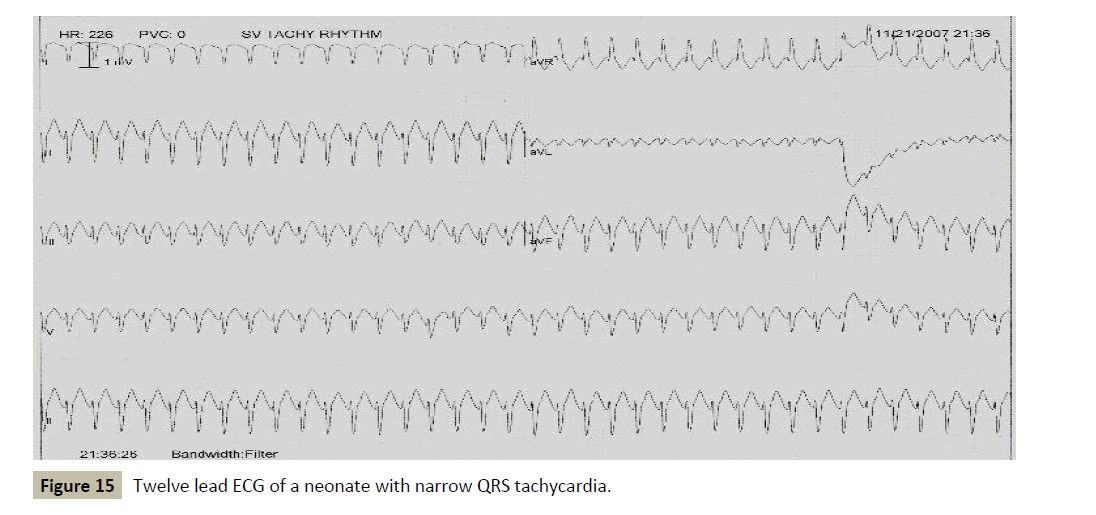
Figure 15:Twelve lead ECG of a neonate with narrow QRS tachycardia.
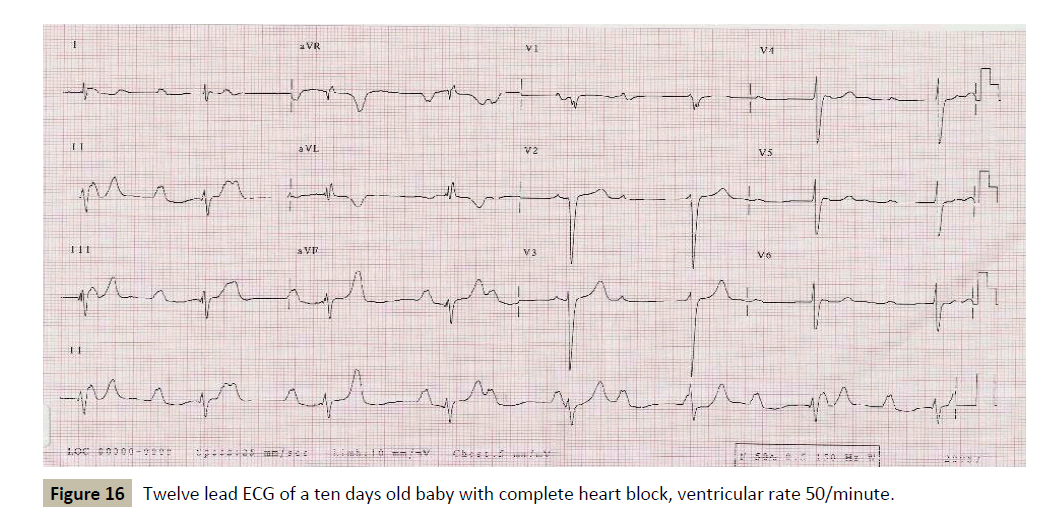
Figure 16:Twelve lead ECG of a ten days old baby with complete heart block, ventricular rate 50/minute.
Arrhythmia
Arrhythmias though rare, are not uncommon in full term and preterm newborns. Maternal diabetes, toxemia and other post natal conditions e.g. asphyxia, hypothermia, metabolic and electrolyte imbalances all contribute to rhythm disturbances. High index of suspicion in all neonates with left ventricular dysfunction is necessary to diagnose this condition. A critical evaluation of electrocardiography (ECG) is essential especially because many of these ECGs may casually interpreted as sinus tachycardia, which is commonly associated with LV dysfunction. It is not necessary to have very fast heart rate to diagnose this condition. Suspicion is aroused when
A) The heart rate shows no variability and is fixed between 150 to 180 per minute.
B) Abnormal P wave axis
C) Atrioventricualr dissociation
Prompt control of heart rate or return to sinus rhythm causes complete return of LV function to normal.
Tachyarrhythmia
Classified into two groups-
Narrow QRS tachycardia and wide QRS tachycardia
A) Narrow QRS tachycardia:
Although paroxysmal supraventricular tachycardia (SVT) caused by accessory pathway (WPW syndrome) is the commonest mechanism in the neonatal period, this condition rarely causes heart failure because it is rarely sustained. The much rarer varieties of sustained supraventricular tachycardia (called Junctional ectopic tachycardia) is more often responsible for heart failure because of its sustained nature. Atrial arrhythmias, like atrial flutter or atrial fibrillation, very common in adults, are very rarely seen in pediatric practice, more so in neonate. Structural heart defects are uncommon in this group of tachycardia.
B) Wide QRS tachycardia:
This is relatively rare in neonatal period and is usually associated with some structural damage to the heart (e.g. Myocarditis, cardiac tumor etc.) Wide QRS tachycardia is relatively rare in neonates
Management
Early management: Initial management, based on the guidelines of the advanced pediatric life support group, depends on the general condition of the infant.
A) Circulatory collapse with a tachycardia whether broad or narrow complex requires DC cardioversion, which should be synchronized
B) If the compromise is not critical, try adenosine first
C) In the infant with a narrow complex tachycardia who is not compromised, facial immersion can be tried. With the infant wrapped in a towel and connected to an ECG, the face is immersed for approximately five seconds into a bowl of cold water. It is safe and effective [21]. Ocular pressure is not recommended at any age, and carotid massage does not work and compresses the airway.
Adenosine at an initial dose of 200 mcg/kg can be given rapidly intravenously into a large vein (such as the antecubital fossa). Up to 500 mcg/kg is occasionally required [22]. Failure of adenosine to terminate the tachycardia may be due to:
1) Inadequate dosage or too slow administration of the drug.
2) The mechanism being atrial tachycardia; as adenosine blocks the AV node, it may reveal atrial flutter or atrial tachycardia as the cause of the problem.
3) The mechanism being ventricular tachycardia (VT)
Transient termination of a conduction system dependent tachycardia, with a few beats of sinus rhythm before restarting, is not uncommon. In this case, additional antiarrhythmic treatment is required. Intravenous amiodarone is increasingly used. Reasons being:
1) It will work if the diagnosis is SVT or VT.
2) It has little negative inotropic effect, so it is relatively safe when myocardial function may be compromised.
3) It is effective with atrial flutter and safer than intravenous flecainide because it slows atrioventricular (AV) nodal conduction as well as slowing and eventually interrupting the flutter circuit.
Maintenance therapy
Various pharmaceutical agents are used in the management of neonatal tachycardias. The standard classification of commonly used drugs is the Vaughan Williams’ classification of antiarrhythmics. Commonly used medications are beta blocker, amiodarone, flecainide and sotalol.
Digoxin is sometimes used as adjunctive treatment to provide some AV block in combination with another agent, particularly flecainide, but also sotalol and amiodarone.
The natural history of SVT presenting in the neonate suggestss that spontaneous resolution usually occurs in the first year of life [22, 23].
Bradyarrhythmias
Depending on the heart rate bradyarrythmias (commonest being Complete heart block) can cause heart failure even in fetal life. Careful and regular heart evaluation of these neonates is essential in order to advise pacemaker. The current recommendation for permanent in neonates are:
• Symptoms- Most commonly heart failure
• Heart rate less than 55 beats per minute and 70 per minute with structural heart defect.
• Left ventricular dysfunction on echocardiography.
Summary
Today a medical, catheter intervention or surgical option can be offered to:
A sick neonate with satisfactory early and long term outcomes. For that purpose, early recognition of a neonate with a cardiac problem, immediate stabilization and timely intervention are essential.
References
- Gardner TH (1971) Cardiac emergencies in the newborn period. Radiology clinic of North America 9: 385-397.
- Wechsler SB,Wernovsky G (1998) Cardiac disorders.In:John PC,Ann RS (edr)Manual of Neonatal Care-Joint program in neonatology.Lippincott-Raven, Philadelphia.
- Schamberger M (1996) Cardiac emergencies in Children.Pediatr Ann 25:339-344.
- Coceani F (1974) Prostaglandins and the central nervous system.Arch Interm Med 133:119.
- Lee C, Mason LJ (2001)Pediatric cardiac emergencies.Anesthesiology Clinic of North America 19: 286-309.
- Gewitz M,Vetter V (2000) Cardiac Emergencies.In:Fleisher GR,Ludwig S(edr)Text book of Pediatric Emergency Medicine. Lippincott Williams & Wilkins,Philadelphia.
- Rao P,StreipeV,Merrill W (1994) Hypoplastic left heart syndrome.In:Kambam J(edr) Cardiac Anesthesia for Infants and Children.St Louis,Mosby.
- Helton JG, Aglira BA, Chin AJ, Murphy JD, Pigott JD, et al. (1986) Analysis of potential anatomic or physiologic determinants of outcome of palliative surgery for hypoplastic left heart syndrome. Circulation 74: 170-176.
- Norwood WI, Kirklin JK, Sanders SP (1980) Hypoplastic left heart syndrome: Experience with palliative surgery. Am J Cardiol 45:87-91.
- Colli AM1 Perry SB, Lock JE, Keane JF,et al. (1995) Balloon dilation of critical valvar pulmonary stenosis in the first month of life.JAm Coll Cardiol34:23-28.
- Justo RN, Nykanen DG, Williams WG, Freedom RM, Benson LN, et al. (1997)Transcatheter perforation of the right ventricular outflow tract as initial therapy for pulmonary valve atresia and intact ventricular septum in the newborn. Cathet Cardiovasc Diagn 40:408-413.
- Schranz D, Michel-Behnke I, Heyer R, Vogel M, Bauer J, et al. (1998) Stent implantation of the arterial duct in newborns with duct-dependent circulation. Eur Heart J 19:1401-1409.
- Rosenthal E, Qureshi SA, Tynan M (1994) Percutaneous pulmonary valvotomy and arterial duct stenting in neonates with right ventricular hypoplasia. Am J Cardiol 74:304-306.
- Hugh DA (2001) Moss and Adams' Heart Disease in Infants, Children, and Adolescents: Including the Fetus and Young Adult.Wolters Kluwer Health, Philadelphia.
- Idriss FS, Ilbawi MN, DeLeon SY, Duffy CE, Muster AJ,et al. (1988)Arterial switch in simple and complex transposition arteries.J Thorac Cardiovasc Surg 95:29-36.
- Jonas JA, Giglia TM, Sanders SP, Wernovsky G, Nadal-Ginard B, et al. (1989)Rapid, two-stage arterial switch for transposition of the great arteries and intact ventricular septum beyond the neonatal period. Circulation80:I203-1208.
- Dabritz S, Engelhardt W, Von Bernuth G, Messmer BJ (1997)Trial of pulmonary artery banding: a diagnostic criterion for “one-stage”arterial switch in simple transposition of the great arteries beyond the neonatal period. Eur J Cardiothorac Surg 11: 112-116.
- Kang N, De leval MR, Elliott M, Tsang V, Kocyildirim E, et al. (2004)Extending the boundaries of the primary arterial switch operation in patients with transposition of the great arteries and intact ventricular septum. Circulation 110: 123-127.
- Bisoi AK, Sharma P, Chauan S, Reddy SM, Das S, et al. (2010)Primary arterial switch operation in children presenting late with d-transposition of great arteries and intact ventricular septum. When is it too late for a primary arterial switch operation? Eur J Cardiothorac Surg 38:707-713.
- Williams WG, Trusler GA, Kirklin JW, Blackstone EH, Coles JG, et al. (1988) Early and later protocol for simple transposition leading to an atrial switch repair.J Thorac Cardiovasc Surg 95:717-726.
- Sreeram N,Wren C (1990) Supraventricular tachycardia in infants:response to initial treatment.Arch Dis Child65:127-129.
- Dixon J,Foster K,Wyllie J, Wren C (2005) Guidelines and adenosine dosing in supraventricular tachycardia.Arch Dis Child 90:1190-1191.
- Van Engelen AD,Weijtens O,Brenner Jl, Charles SK, Joshua AC, et al. (1994) Managment,outcome and follow up of fetal tachycardia.Jam Coll Cardiol24:1371-1375.

