Keywords
Gemcitabine; Pancreatic Neoplasms; Polymorphism, Single Nucleotide; Radiotherapy, Intensity-Modulated; Receptor, IGF Type 1; Tumor Necrosis Factor-alpha
Abbreviations
ECOG: Eastern Cooperative Oncology Group; FFCD-SFRO: Federation Francophone de Cancerologie Digestive- Societe Francaise de Radiotherapie Oncologique; GERCOR: Groupe Cooperateur Multidisciplinaire en Oncologie; GITSG: Gastrointestinal Tumor Study Group; IGFR: insulin-like growth factor receptor; PU: particle unit; SNP: single nucleotide polymorphism
INTRODUCTION
Locally advanced pancreatic cancer is defined as the presence of a surgically unresectable tumor (involving the celiac axis or the superior mesenteric artery) without evidence of distant metastases [1]. While surgery is the only means of cure for pancreatic cancer, fewer than 10% of patients are eligible for resection based on the extent of disease at presentation. According to the Surveillance, Epidemiology and End Results (SEER; https://seer.cancer.gov/statfacts/html/pancreas.html) database, 26% of pancreatic cancer cases are locally advanced at the time of diagnosis, with a 5-year survival rate of 8.7% [2].
What Did We Know before ASCO 2009?
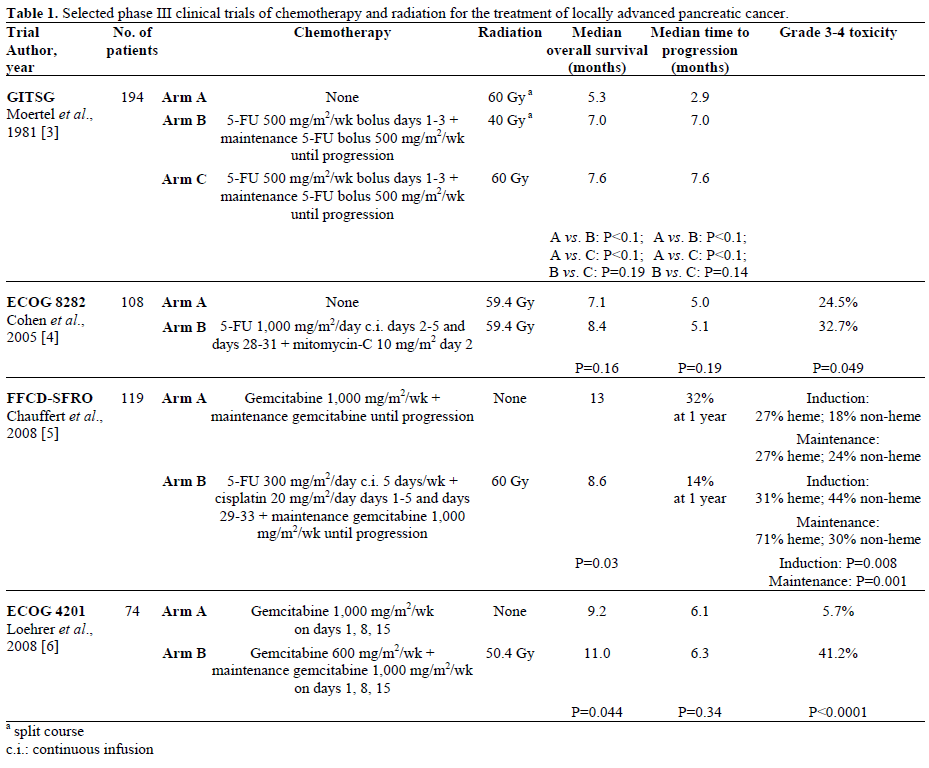
Chemoradiotherapy with 5-fluorouracil (5-FU) and radiotherapy to a total dose of 50 Gy increases overall survival and quality of life of patients with locally advanced pancreatic cancer, as supported by the Gastrointestinal Tumor Study Group (GITSG) [3] and the Eastern Cooperative Oncology Group (ECOG) 8282 [4] trials. Most studies have investigated 5-FUbased chemotherapy regimens with radiotherapy. Over the last 10 years, gemcitabine has become the standard of chemotherapy in advanced pancreatic carcinoma and is also a potent radiosensitizer of epithelial cells. Many phase I and II trials have demonstrated the feasibility of combining radiotherapy (to total doses ranging from 24 to 61 Gy) with gemcitabine at weekly doses ranging from 100 to 1,000 mg/m2, however results of randomized phase II studies are not sufficient or consistent to recommend such a regimen. Therefore, 5- FU is still the reference chemotherapy in association with radiotherapy for locally advanced pancreatic cancer. The optimal protocol to deliver 5-FU has not been evaluated in comparative trials, and multiple administration schedules have been reported, including weekly bolus (250 to 600 mg/m2), bolus on the first three days of radiotherapy (350 to 600 mg/m2), continuous infusion on the first and fifth weeks of radiotherapy (1,000 mg/m2), and continuous infusion (200 to 300 mg/m2/day).
Even if chemoradiotherapy were widely used to treat patients with locally advanced pancreatic cancer, its superiority compared to chemotherapy has never been proven. In the Federation Francophone de Cancerologie Digestive-Societe Francaise de Radiotherapie Oncologique (FFCD-SFRO) trial [5], although the chemoradiotherapy regimen used was not optimal (5-FU and cisplatin with 60 Gy external beam radiation therapy) and produced unacceptable toxicity rates, results of this trial were consistent with older studies published in the 1980s. The results of the ECOG E4201 phase III trial [6] were in favor of chemoradiotherapy, however these results should be considered cautiously because of the insufficient number of patients included.
Table 1 summarizes selected phase III randomized clinical trials of chemotherapy and radiation in the treatment of locally advanced pancreatic cancer.
What Did We Learn at ASCO 2009?
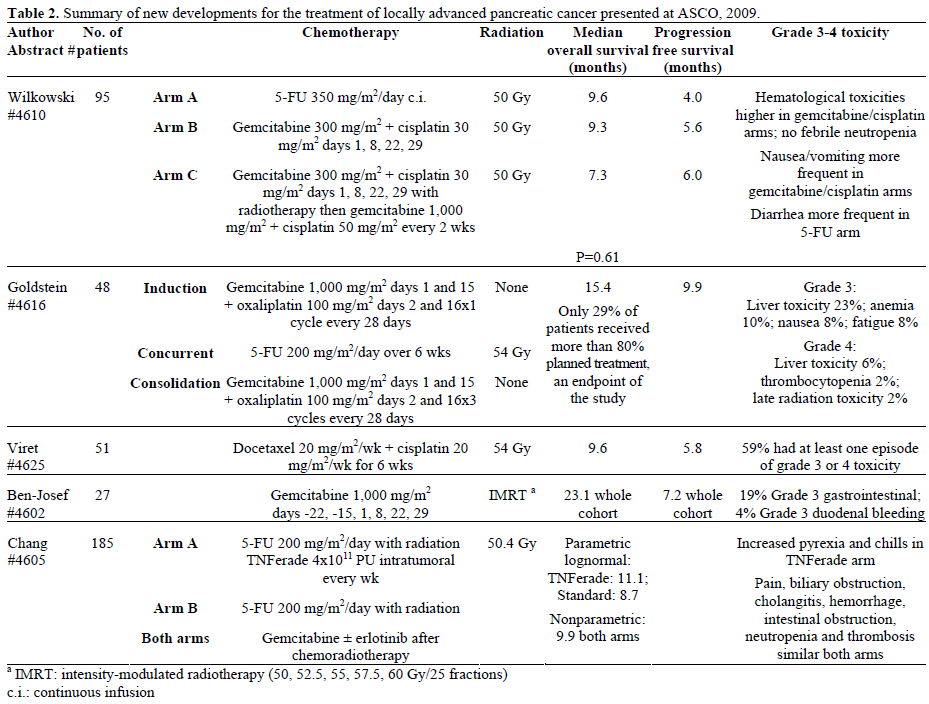
Table 2 summarizes the findings of studies presented at this year’s ASCO annual meeting.
Abstract #4610. Final analysis of a multicenter, randomized phase II trial comparing three different chemoradiotherapy regimens in the treatment of patients with locally advanced, nonmetastatic pancreatic cancer. [7]
Wilkowski et al. reported the final analysis of a phase II multicenter trial in Germany comparing three different concurrent chemoradiotherapy regimens for locally advanced pancreatic cancer [7]. All patients received 50 Gy of EBRT in combination with one of three chemotherapy regimens: 1) 5-FU as a 24-hour infusion (350 mg/m2 on each day of radiation); 2) low lowdose gemcitabine 300 mg/m2 and cisplatin 30 mg/m2 on days 1, 8, 22, and 29; or 3) the same low-dose gemcitabine and cisplatin regimen followed by sequential chemotherapy with full-dose gemcitabine 1,000 mg/m2 and cisplatin 50 mg/m2 every two weeks until disease progression or unacceptable toxicity. Seventy patients were evaluable out of a total of 95 who were recruited. There was no difference among the three treatment arms with respect to the primary endpoint of overall survival at nine months (P=0.61). Response rate, a secondary endpoint, was 19% in the radiotherapy/5-FU arm, 22% in the radiotherapy/low dose gemcitabine/cisplatin arm, and 13% in the radiotherapy/low dose gemcitabine/cisplatin with sequential full dose gemcitabine/cisplatin arm. Grade 3 and 4 hematologic toxicities as well as rates of nausea and vomiting were higher in the two gemcitabine/cisplatin arms compared to 5-FU. The authors concluded that radiotherapy with gemcitabine/cisplatin was not more clinically efficacious than radiotherapy with 5-FU. The findings of this trial, as with previously reported studies, should be interpreted with caution due to the small sample size. Although combined modality therapy was not associated with improved outcome in this trial, the rates of increased hematologic and nonhematologic toxicities remain important observations.
Abstract #4616. GOFURTGO trial (GFG): An AGITG multicenter phase II study of fixed dose rate gemcitabine-oxaliplatin (Gem-Ox) integrated with concomitant 5-FU and 3-D conformal radiotherapy (5- FU-3-DRT) for the treatment of locally advanced pancreatic cancer. [8]
Goldstein et al. reported the findings of a phase II multicenter trial of fixed dose rate gemcitabine and oxaliplatin integrated with concomitant 5-FU and three-dimensional conformal radiotherapy [8]. The authors previously published the results of a regimen consisting of induction gemcitabine followed by continuous 5-FU with concurrent radiotherapy followed by consolidation gemcitabine [9]. The phase II trial presented this year used this same paradigm and added oxaliplatin to gemcitabine induction and consolidation. Forty-eight patients were enrolled and received induction treatment with gemcitabine 1,000 mg/m2 days 1 and 15 and oxaliplatin 100 mg/m2 days 2 and 16 of a 28-day cycle, followed by 5-FU 220 mg/m2/day over 6 weeks during radiotherapy of 54 Gy. Three consolidation doses of gemcitabine and oxaliplatin (as given for induction) were administered four to six weeks after completion of 5- FU/radiotherapy. The study endpoints were feasibility (defined as more than 80% patients completing treatment), safety/toxicity, regimen activity as defined by objective response, progression free survival, and overall survival, as well as quality of life. Only 24 patients (50%) completed all planned cycles of treatment, with 29% completing more than 80% of all treatment. Treatment was discontinued due to toxicity (16%), progressive disease (21%), or doctor/patient preference (4%/2%). The most common treatmentrelated toxicity affected liver function (grade 3: 23%; grade 4: 6%). Grade 3 cytopenias, fatigue, and GI effects including nausea were also observed. Median progression free survival was 9.9 months, and median overall survival was 15.4 months at a median follow up of 29.7 months. The authors concluded that the addition of oxaliplatin to the previously described gemcitabine-5FU/radiotherapy-gemcitabine regimen improved progression free survival (previously 7.1 months) and overall survival (previously 11.7 months) without significant offset by toxicity. Despite the observed improvement in these parameters compared to the authors’ prior study, it should be noted that less than a third of enrolled patients completed more than 80% of the planned treatment, primarily due to progressive disease or toxicity, thus making it difficult to generalize these findings.
Abstract #4625. A phase II study of radiation and docetaxel and cisplatin in the treatment of locally advanced pancreatic carcinoma: FNCLCC-ACCORD 09/0201 trial [10].
Viret et al. presented the results of a phase II trial evaluating the efficacy and toxicity of radiation with docetaxel and cisplatin for the treatment of locally advanced pancreatic cancer [10]. Fifty-one patients were enrolled and received a total of 54 Gy EBRT in 1.8 Gy fractions with docetaxel and cisplatin 20 mg/m2 each weekly for six weeks. The objective response rate was 16%, with a median duration of 7.6 months. Nearly 60% of patients experienced at least one episode of grade 3 or 4 toxicity, with asthenia, anorexia, vomiting, and nausea being the most common adverse effects. Median progression free survival was 5.8 months. Median overall survival was 9.6 months with a median of 21 months of follow up. The authors concluded that the combination of docetaxel and cisplatin with radiotherapy had limited effect in patients with locally advanced pancreatic cancer. As observed in other trials, the rates of significant treatment-related toxicities were quite high.
Abstract #4602. Phase I radiation dose-escalation trial of intensity-modulated radiotherapy with concurrent fixed dose-rate gemcitabine for unresectable pancreatic cancer [14].
Intensity-modulated radiotherapy is a radiation therapy technique that allows for dose intensification with concurrent improved sparing of normal tissues. By dividing the radiation beams into thousands of “pencil beams” of varying intensities, concave dose distributions and very sharp regions of dose fall-off can be created. Gemcitabine is known to be a potent radiation sensitizer, with potential for both enhanced anti-tumor effects and increased toxicity. Early studies of concurrent gemcitabine and radiotherapy for locally advanced pancreatic cancer showed substantial doserelated gastrointestinal toxicity [11]. More recent studies have demonstrated the feasibility of treating only the gross tumor volume with full-dose weekly gemcitabine, omitting the uninvolved lymph node beds and thereby decreasing the amount of normal tissue treated, as summarized in Table 3 [12, 13].

At this year’s ASCO annual meeting, Ben-Josef et al. presented results from a radiation dose-escalation study using intensity-modulated radiotherapy and fixed dose rate gemcitabine [14]. Patients with unresectable localized pancreatic cancer were treated with fixed dose-rate gemcitabine 1,000 mg/m2 in a 100-minute infusion on days -22 and -15 and then days 1, 8, 22, and 29. Radiation was started on day 1. Gross tumor volume was defined using a pancreas-protocol CT scan and expanded by 1 cm to create a planning target volume. Active breathing control or 4D simulation was used to account for organ motion. The radiation dose levels were 50, 52.5, 55, 57.5, and 60 Gy, all delivered in 25 fractions. Up to four cycles of fixed dose-rate gemcitabine were given after chemoradiotherapy. The objective was to determine the maximum tolerated radiation dose with concurrent intensity-modulated radiotherapy and fixed dose-rate gemcitabine. Twentyseven patients were enrolled, and the median overall survival was 23.1 months, with a median progressionfree survival of 7.2 months and a response rate of 52.4%. Grade 3 dose-limiting toxicities were seen in six patients, including five patients with nausea, vomiting, dehydration or anorexia and one patient with a duodenal bleed. Only one patient had local progression, and two patients underwent R0 resections, revealing complete and near-complete pathological responses respectively. The authors concluded that high dose intensity-modulated radiotherapy with concurrent fixed dose-rate gemcitabine was tolerable and produced encouraging response rates and survival in locally advanced pancreatic cancer.
Using sophisticated radiotherapy techniques to minimize the dose to normal tissues and account for organ motion, the authors were able to reach a dose of 60 Gy, significantly above the tolerance of the small bowel, which is 45-50 Gy, although further follow-up is needed to accurately evaluate late effects. A detailed account of failure patterns was not included, but local control seems to be quite good. The 23-month median survival is encouraging, given that historically, patients with locally advanced pancreatic cancer survive only 10 months even with chemoradiotherapy. Attempts to intensify local therapy in locally advanced pancreatic cancer by combining hypofractionated stereotactic body radiotherapy (25 Gy in one fraction) and gemcitabine resulted in increased duodenal toxicity without an improvement in survival [15]. Combining fractionated intensity-modulated radiotherapy with concurrent fixed dose-rate gemcitabine may represent a more tolerable and effective approach.
Abstract #4605. Multicenter randomized controlled phase III clinical trial using TNFerade (TNF) with chemoradiation in patients with locally advanced pancreatic cancer: interim analysis of overall survival [18].
Tumor necrosis factor alpha (TNF-alpha) is a multifunctional tumoricidal cytokine that is released by macrophages. TNF-alpha can induce cell death through several mechanisms, including caspase-triggered apoptosis, obliteration of tumor vasculature, and augmentation of immune response to tumor cells. TNFalpha has also been found to be a radiosensitizing agent [16]. TNFerade is a nonreplicating adenovirus vector that delivers human tumor necrosis factor. A phase II dose-escalation trial of TNFerade in combination with 50.4 Gy radiation and 200 mg/m2/day continuous infusion 5-FU demonstrated that the maximum tolerated dose of TNFerade was 4x1011 particle units (PU) [17]. The median survival was 9.8 months, although three of eleven patients survived over 18 months. Chang and colleagues presented an interim analysis of a phase III study of TNFerade [18]. Patients with locally advanced pancreatic cancer were randomized 1:2 to either a standard arm with chemoradiotherapy to 50.4 Gy with concurrent continuous infusion 5-FU or the same regimen with the addition of weekly intra-tumoral injections of 4x1011 PU TNFerade. Both arms received adjuvant gemcitabine with the option of erlotinib. A total of 330 patients were enrolled, and an interim analysis of overall survival was planned to occur after 92 deaths. Of the number of patients enrolled, 185 were evaluable for survival analysis, with 117 in the TNFerade arm and 68 in the standard arm. A parametric lognormal analysis showed a median survival of 11.1 months for the TNFerade arm, compared to 8.7 months for the standard arm. A nonparametric analysis showed a median survival of 9.9 months for both arms, with a “late effect” seen in the TNFerade arm. Toxicity was similar in both arms with the exception of increased pyrexia and chills in the TNFerade arm. The authors concluded that there was an encouraging trend in favor TNFerade use. A second interim analysis is planned after 184 deaths have occurred.
TNFerade represents a novel approach to intensifying local therapy in locally advanced pancreatic cancer. Although the concept of combining radiation with a locally targeted radiosensitizing and tumor necrosing agent is appealing, the interim analysis presented did not demonstrate a significant survival benefit with the addition of TNFerade to standard chemoradiotherapy. Although the trial planned to enroll 330 patients, only 185 subjects were available for the interim analysis. TNFerade appears tolerable; however there is no evidence at this point that it represents an improvement over standard therapies. Results of the next interim analysis are expected in 2010.
Abstract #4500. The prognostic value of polymorphisms in the insulin-like growth factor receptor (IGFR) pathway in patients with locally advanced pancreatic cancer [23].
The IGFR pathway is upregulated in pancreatic cancer and represents an important potential therapeutic target. In normal cells as well as cancer cells, the insulin-like growth factors IGF-I and IGF-II and their regulatory binding proteins influence cell growth and metabolism. By binding to the IGFR, IGF-I and IGF-II modulate cell survival and progression through the cell cycle via the PI3/AKT pathway as well as through extracellular signal-regulated kinase pathways by means of insulin receptor substrate, Src homology and collagen adapter proteins [19]. IGFR is expressed at high levels in pancreatic cancers [20], and recent preclinical studies have shown that inhibition of IGFR can inhibit growth and survival of pancreatic cell lines [21]. IGFR inhibitors have also demonstrated anti-tumor synergy with gemcitabine against pancreatic cancer xenografts [22]. Table 4 shows IGFR inhibitors currently in clinical trials for pancreatic cancer.

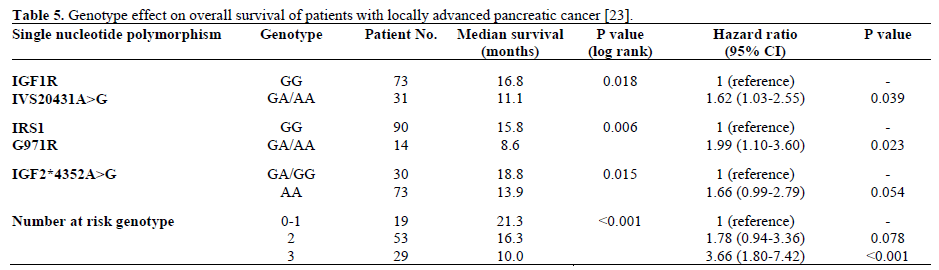
At this year’s ASCO meeting, Shroff et al. presented results of a study of the prognostic value of single nucleotide polymorphisms (SNPs) of the IGFR pathway in locally advanced pancreatic cancer [23].
Thirty-nine SNPs from seven candidate genes from the IGFR pathway were investigated using DNA samples extracted from 105 patients with locally advanced pancreatic cancer. Genotyping was performed using the Sequenom method. Kaplan-Meier, log-rank, and Cox regression analyses were used to compare overall survival of patients with different genotypes, taking into account clinical factors including performance status, CA 19-9, induction chemotherapy, LDH, albumin, and hemoglobin. The median survival time for the cohort was 15 months. Three SNPs were significantly associated with survival, and two remained significant after Cox regression analysis. Patients who were heterozygous and homozygous with regard to these polymorphisms had lower median survival than those who did not have the polymorphism. In addition, patients with two or three deleterious alleles had poorer survival than those who had none or only one (Table 5). These results were validated in an additional cohort of 42 patients. The authors suggested that SNPs in the IGFR pathway may have prognostic value in locally advanced pancreatic cancer. While the findings of this study are interesting, they will take on added significance if the SNPs that were identified can predict response to therapy in addition to offering prognostic information. Further investigation is required to determine whether a panel of SNPs can select patients with locally advanced pancreatic cancer who will respond to IGFR inhibitors.
Discussion
The treatment of locally advanced pancreatic cancer remains a formidable challenge in oncology due to the aggressive nature of the disease as well as the, at best, modestly effective treatments, which are in many cases limited by significant toxicities. The use of chemoradiotherapy for locally advanced pancreatic cancer is based on data from studies with relatively small numbers of patients and with varying methodologies. Thus, the use of an evidence-based standard approach remains controversial. Chemoradiotherapy is superior to best supportive care and exclusive radiotherapy alone and leads to a similar outcome when compared to modern chemotherapy with gemcitabine but with added toxicity. Induction chemotherapy before concurrent chemoradiotherapy improves survival of patients with locally advanced pancreatic cancer. In addition to sparing patients with rapidly progressive disease from potentially toxic radiotherapy, such a therapeutic strategy may help to define the subset of patients benefiting from chemoradiotherapy.
The value of induction chemotherapy before chemoradiotherapy needs to be validated in prospective controlled trials, and the Groupe Cooperateur Multidisciplinaire en Oncologie (GERCOR) LAP07 phase III trial has been designed to evaluate this therapeutic approach. LAP07 is an international trial in which patients receive induction chemotherapy (randomly assigned to gemcitabine or gemcitabine plus erlotinib) for the first 4 months of treatment. Patients with a controlled tumor after this first phase of treatment will be randomly assigned to two additional cycles of chemotherapy or chemoradiotherapy (conformal radiotherapy to a total dose of 54 Gy in five fractions of 1.8 Gy per week and concomitant oral capecitabine with a total dose of 1,600 mg/m2 per day, 5 days a week). After the end of this second phase, patients who have received erlotinib during induction chemotherapy will continue erlotinib as maintenance treatment until progression (Figure 1).
Figure 1. Schema for GERCOR LAP07 trial.
Conflict of interest
The authors have no potential conflicts of interest
References
- American Joint Committee on Cancer. Exocrine Pancreas. In: AJCC Cancer Staging Manual. 6th ed. New York, NY: Springer, 2002, pp 157-164. [ISBN 387952713]
- Horner MJ, Ries LAG, Krapcho M, et al. (eds). SEER Cancer Statistics Review, 1975-2006, National Cancer Institute. Bethesda, MD, USA: 2006.
- Moertel CG, Frytak S, Hahn RG, O'Connell MJ, Reitemeier RJ, Rubin J, et al. Therapy of locally unresectable pancreatic carcinoma: a randomized comparison of high dose (6000 rads) radiation alone, moderate dose radiation (4000 rads + 5-fluorouracil), and high dose radiation + 5-fluorouracil: The Gastrointestinal Tumor Study Group. Cancer 1981; 48:1705-10. [PMID 7284971]
- Cohen SJ, Dobelbower R Jr, Lipsitz S, Catalano PJ, Sischy B, Smith TJ, et al. A randomized phase III study of radiotherapy alone or with 5-fluorouracil and mitomycin-C in patients with locally advanced adenocarcinoma of the pancreas: Eastern Cooperative Oncology Group study E8282. Int J Radiat Oncol Biol Phys 2005; 62:1345-50. [PMID 16029791]
- Chauffert B, Mornex F, Bonnetain F, Rougier P, Mariette C, Bouché O, et al. Phase III trial comparing intensive induction chemoradiotherapy (60 Gy, infusional 5-FU and intermittent cisplatin) followed by maintenance gemcitabine with gemcitabine alone for locally advanced unresectable pancreatic cancer. Definitive results of the 2000-01 FFCD/SFRO study. Ann Oncol 2008; 19:1592-9. [PMID 18467316]
- Loehrer PJ, Powell ME, Cardenes HR, Wagner L, Brell JM, Ramanathan RK, et al. A randomized phase III study of gemcitabine in combination with radiation therapy versus gemcitabine alone in patients with localized, unresectable pancreatic cancer: E4201. J Clin Oncol 2008, 26(15 Suppl.): Abstract 4506.
- Wilkowski R, Boeck S, Ostermaier S, Sauer R, Herbst M, Fietkau R, et al. Final analysis of a multicenter, randomized phase II trial comparing three different chemoradiotherapy regimens in the treatment of patients with locally advanced, nonmetastatic pancreatic cancer. J Clin Oncol 2009, 27(15 Suppl.): Abstract 4610.
- Goldstein D, van Hazel G, Selva-Nayagam S, Ackland S, Shapiro J, Carroll S, et al. GOFURTGO trial (GFG): An AGITG multicenter phase II study of fixed dose rate gemcitabine-oxaliplatin (Gem-Ox) integrated with concomitant 5FU and 3-D conformal radiotherapy (5FU-3DRT) for the treatment of locally advanced pancreatic cancer (LAPC). J Clin Oncol 2009, 27(15 Suppl.): Abstract 4616.
- Goldstein D, Van Hazel G, Walpole E, Underhill C, Kotasek D, Michael M, et al. Gemcitabine with a specific conformal 3D 5FU radiochemotherapy technique is safe and effective in the definitive management of locally advanced pancreatic cancer. Br J Cancer 2007; 97:464-471. [PMID 17653074]
- Viret F, Ychou M, Baey C, Bennouna J, Adenis A, Peiffert D, et al. A phase II study of radiation and docetaxel and cisplatin in the treatment of locally advanced pancreatic carcinoma. FNCLCCACCORD 09 /0201 trial. J Clin Oncol 2009, 27(15 Suppl.): Abstract 4625.
- Wolff RA, Evans DB, Gravel DM, Lenzi R, Pisters PW, Lee JE, et al. Phase I trial of gemcitabine combined with radiation for the treatment of locally advanced pancreatic adenocarcinoma. Clin Cancer Res 2001; 7:2246-53. [PMID 11489798]
- Talamonti MS, Small W Jr, Mulcahy MF, Wayne JD, Attaluri V, Colletti LM, et al. A multi-institutional phase II trial of preoperative full-dose gemcitabine and concurrent radiation for patients with potentially resectable pancreatic carcinoma. Ann Surg Oncol 2006; 13:150-8. [PMID 16418882]
- Murphy JD, Adusumilli S, Griffith KA, Ray ME, Zalupski MM, Lawrence TS, Ben-Josef E. Full-dose gemcitabine and concurrent radiotherapy for unresectable pancreatic cancer. Int J RadiatOncolBiol Phys 2007; 68(3):801-8. [PMID 17379445]
- Ben-Josef E, Griffith K, Francis IR, Khan G, Lawrence TS, Abrams R, et al. Phase I radiation dose-escalation trial of intensitymodulated radiotherapy (IMRT) with concurrent fixed dose-rate gemcitabine (FDR-G) for unresectable pancreatic cancer. J Clin Oncol 2009, 27(15 Suppl.): Abstract 4602.
- Schellenberg D, Goodman KA, Lee F, Chang S, Kuo T, Ford JM, et al. Gemcitabine chemotherapy and single-fraction stereotactic body radiotherapy for locally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys 2008; 72:678-86. [PMID 18395362]
- Balkwill F. Tumor necrosis factor and cancer. Nat Rev Cancer 2009; 9:361-71. [PMID 19343034]
- Senzer N, Hanna N, Chung T, Nemunaitis J, Rosemurgy A, Javle M, et al. Updated response and survival data for TNFerade combined with chemoradiation in the treatment of locally advanced pancreatic cancer (LAPC) . J Clin Oncol 2005, 23(16 Suppl.): Abstract 4097.
- Chang KJ, Fisher W, Kenady D, Klapman J, Posner M, Reid T, et al. Multicenter randomized controlled phase III clinical trial using TNFerade (TNF) with chemoradiation (CRT) in patients with LAPC (LAPC): Interim analysis (IA) of overall survival (OS). J Clin Oncol 2009, 27(15 Suppl.): Abstract 4605.
- Pollak MN, Schernhammer ES, Hankinson SE. Insulin-like growth factors and neoplasia. Nat Rev Cancer 2004; 4:505-18. [PMID 15229476]
- Bergmann U, Funatomi H, Yokoyama M, Beger HG, Korc M. Insulin-like growth factor I overexpression in human pancreatic cancer: evidence for autocrine and paracrine roles. Cancer Res 1995; 55:2007-11. [PMID 7743492]
- Beltran PJ, Mitchell P, Chung YA, Cajulis E, Lu J, Belmontes B, et al. AMG 479, a fully human anti-insulin-like growth factor receptor type I monoclonal antibody, inhibits the growth and survival of pancreatic carcinoma cells. Mol Cancer Ther 2009; 8:1095-105. [PMID 19366899]
- Maloney EK, McLaughlin JL, Dagdigian NE, Garrett LM, Connors KM, Zhou XM, et al. An anti-insulin-like growth factor I receptor antibody that is a potent inhibitor of cancer cell proliferation. Cancer Res 2003; 63:5073-83. [PMID 12941837]
- Shroff RT, Javle MM, Dong X, Kumar VS, Krishnan S, Wolff RA, et al. The prognostic value of polymorphisms in the insulin-like growth factor receptor (IGFR) pathway in patients with locally advanced pancreatic cancer (LAPC). J Clin Oncol 2009, 27(15 Suppl.): Abstract 4500.


