Keywords
Adenocarcinoma; Carcinoma, Pancreatic Ductal; Fluorouracil; gemcitabine; oxaliplatin; Pancreatic Neoplasms; Radiotherapy; Salvage Therapy; Treatment Failure
Abbreviations CONKO:
Charité Onkologie; FA: folinic acid or leucovorin
INTRODUCTION
Pancreatic cancer remains a major therapeutic challenge in 2008. The annual incidence rate of pancreatic cancer is almost identical to the mortality rate; approximately 37,000 new cases are diagnosed each year in the United States, and approximately 33,000 patients die from this disease [1, 2]. Poor prognosis has been attributed to an inability to diagnose pancreatic cancer at an early stage. Majority of patients have advanced pancreatic cancer at the time of diagnosis. Advanced disease is associated with a dismal outcome, with a median survival of 3-6 months. Below is a summary of the data on pancreatic cancer presented at the 44th ASCO Annual Meeting’, Chicago, IL, USA, May 30 - June 3, 2008 (Table 1).

Adjuvant Therapy of Pancreatic Cancer
A minority of patients (15-20%) present with resectable disease as pancreatic cancer tends to metastasize to regional lymph nodes early in the course of the disease and many patients have subclinical liver metastases at the time of diagnosis. Despite following curatively intended resection, prognosis of patients with pancreatic cancer is dismal. Whereas gemcitabine-based chemotherapy is standard in advanced pancreatic cancer, the role of adjuvant chemotherapy is still under discussion [7].
Final results of the randomized, prospective, multicenter phase III trial of adjuvant chemotherapy with gemcitabine versus observation in patients with resected pancreatic cancer so called the CONKO-001 were presented at the meeting [3].
CONKO-001. A Multicenter Phase III Trial of Adjuvant Chemotherapy with Gemcitabine versus Observation in Patients with Resected Pancreatic Cancer
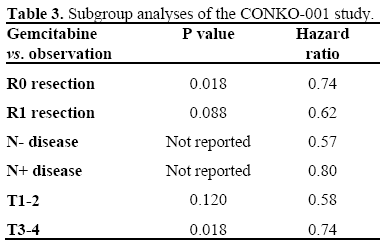
Study Design. A prospective, open, multicenter, controlled phase III study was designed to evaluate the efficacy and toxicity of gemcitabine in pancreatic cancer patients after complete (R0 or R1) resection (Figure 1). After stratification for R0/R1, nodal tumor involvement and tumor stage patients were randomized to receive either gemcitabine (1 g/m2 days 1, 8, and 15 every 4 weeks) for 6 months or observation. Objectives. Primary study endpoint was disease free survival; secondary endpoints included overall survival and toxicity. The study was powered to detect a significant difference in disease free survival with 90% probability at a significance level of 0.05 on all eligible patients. Results. The results of this study were recently published in JAMA 2007 showing that postoperative gemcitabine is well tolerated and significantly delays the development of recurrent disease after complete resection of pancreatic cancer. At this meeting, 3-year and 5-year overall survival was presented (Table 2). Subgroup analyses also presented at the meeting demonstrate significant increased disease free survival for gemcitabine in all subgroups of stratification as shown in Table 3.
Figure 1. Study design CONKO-001: adjuvant
chemotherapy in patients with resected pancreatic
cancer.
URL: upper reference limit
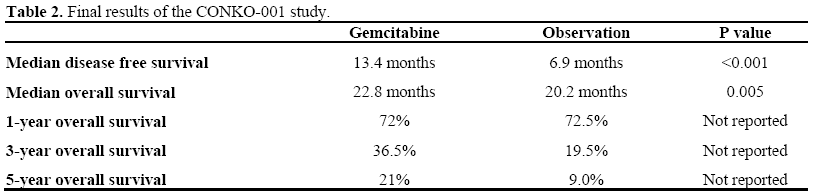
In summary, adjuvant treatment with gemcitabine for 6 months significantly increases disease free survival and overall survival compared with observation alone.
Locally Advanced Pancreatic Cancer
Surgery is often contraindicated by vascular invasion, making the pancreatic cancer unresectable. Neoadjuvant chemo-radiation has theoretical advantages; however, true pathological down-staging is rare with current treatment (1-5%) [8]. Unfortunately, most succumb with distant metastases. Chemoradiation therapy has shown to be associated with improved overall survival as well as better pain control. A recent French study (FFCD-SFRO: Federation Francophone de Cancerologie Digestive and Societe Francaise de Radiotherapie Oncologique) showed improved overall survival with gemcitabine vs. chemo-radiation using 5-FU and cisplatin [9]. The first study that compared gemcitabine in combination with radiation therapy versus gemcitabine alone in patients with locally advanced pancreatic cancer was presented at the meeting (E4201 study) [4].
E4201. A Randomized Phase III Study of Gemcitabine in Combination with Radiation Therapy versus Gemcitabine Alone in Patients with Localized, Unresectable Pancreatic Cancer
Study Design. Patients with histologically proven, locally advanced pancreatic cancer, Eastern Cooperative Oncology Group (ECOG) performance status less than 2, without prior chemotherapy or radiation therapy were enrolled onto this study as outlined in Figure 2. Objectives. With a planned sample size of 316 eligible patients, the trial was designed to have an 88% power to detect a 50% improvement in median overall survival from 8 to 12 months (onesided log-rank test; significance level P=0.025). Results. From April 2003 to December 2005, 71 patients were enrolled but 69 only were evaluable. The study was closed early because of slow accrual. The summary of the results are described in Table 4. Toxicity. Although tolerable, gemcitabine in combination with radiation therapy for locally advanced pancreatic cancer was more myelosuppressive, and also associated with considerable gastrointestinal toxicity and fatigue.
Figure 2. Study design of E4201: gemcitabine in
combination with radiation therapy in locally advanced
pancreatic cancer.
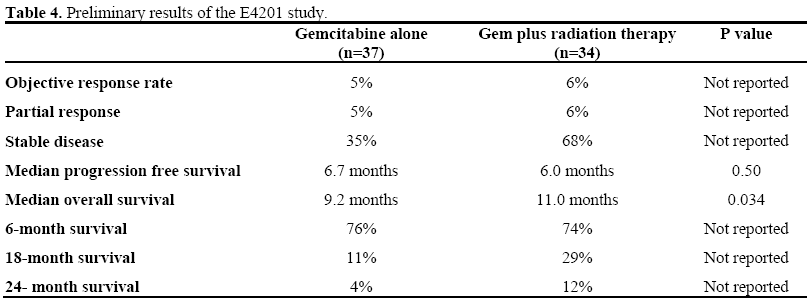
In summary, addition of radiation therapy to gemcitabine significantly improves overall survival (P=0.034) and triples the survival rate at 24 months for patients with locally advanced pancreatic cancer.
First-Line Treatment of Advanced Pancreatic Cancer
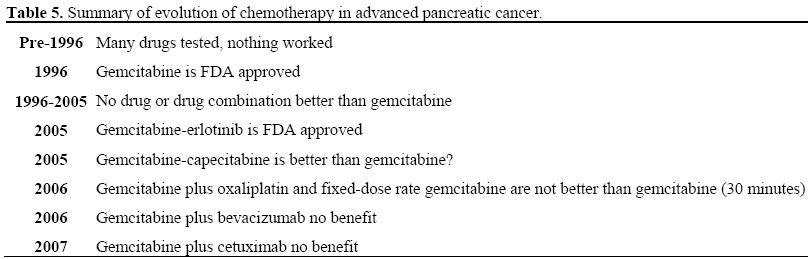
Little progress has been made on the treatment of advanced pancreatic cancer. Gemcitabine has been an acceptable standard for more than a decade. The benefit of singleagent gemcitabine in advanced and metastatic pancreatic cancer is small [10]. Adding other chemotherapy agents to gemcitabine did not result in meaningful improvement in survival. The randomized trials studying the addition of molecular targeting agents (cetuximab, bevacizumab, farnesyl transferase inhibitors and metalloproteinase inhibitors) to gemcitabine compared with gemcitabine alone have been disappointing [2]. A small gain in median survival by adding erlotinib to gemcitabine has recently been reported [11] (Table 5).
In the phase III, overall survival trial of erlotinib plus gemcitabine vs. gemcitabine the hazard ratio was 0.82 (95% CI: 0.69-0.99; P=0.0328) [11]. The phase II bevacizumab with gemcitabine trial showed a 21% response rate with a median overall survival of 8.8 months [12]. Therefore, a phase III randomized, double-blind, placebo controlled, multicenter study was conducted to evaluate the efficacy and safety of adding bevacizumab to erlotinib and gemcitabine in patients with metastatic pancreatic cancer (AViTA study) [5].
AViTA. A Randomized, Double-Blind, Placebo Controlled, Multicenter Phase III Trial to Evaluate the Efficacy and Safety of Adding Bevacizumab to Erlotinib and Gemcitabine in Patients with Metastatic Pancreatic Cancer.
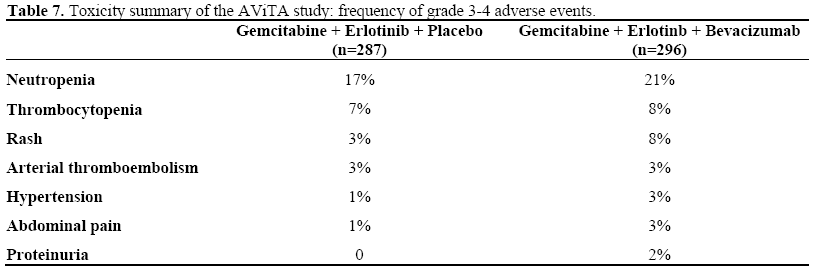
Study Design. The study design is shown in Figure 3. Objectives. The primary endpoint was overall survival, and the secondary endpoints included response, progression free survival, safety, and tolerability. Results. As of March 2007, 454 patients (233/221) had died. Efficacy results are summarized in Table 6. Toxicity. No clinically relevant difference observed in grade 3-4 adverse events between the two arms (Table 7).
Figure 3. Study design of AViTA: addition of
bevacizumab to erlotinib and gemcitabine in advanced
pancreatic cancer.
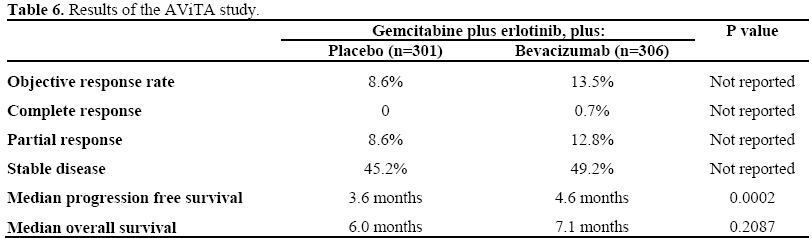
In summary, the study showed that the triple combination with two biologics combined with gemcitabine significantly improved progression free survival (P=0.0002), but not overall survival (P=0.2087), compared to gemcitabine plus erlotinib.
Second-Line Treatment of Advanced Pancreatic Cancer
Current data set on treatment options in second-line setting after gemcitabine failure is scattered and scant. A recently published editorial [13] highlighted that there is no consensus about second-line therapy after disease progression while receiving gemcitabine, but 5-FU-based regimens are considered. Randomized second line studies in advanced pancreatic cancer are very rare. At this meeting, the results of the CONKO- 003 study were presented [6].
CONKO-003. A Randomized Trial in Patients with Gemcitabine Refractory Pancreatic Cancer
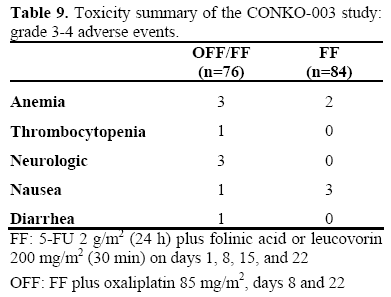
Study Design. This study randomized 165 patients to FF (5-FU 2 g/m2 (24 h) plus folinic acid or leucovorin (FA) 200 mg/m2 (30 min) on days 1, 8, 15, and 22) or OFF (FF plus oxaliplatin 85 mg/m2, days 8 and 22) (Figure 4). Objectives. The primary endpoint was overall survival and secondary endpoints were disease free survival and toxicity. Results. The results presented at the meeting are summarized in Tables 8 and 9. The study indicated that alternating OFF/FF and continuous FF are feasible and tolerable regimens as second-line treatment of advanced pancreatic cancer after gemcitabine failure. OFF/FF results in significantly longer progression free survival (P=0.012) and overall survival (P=0.014) vs. FF. OFF/FF also results in substantially greater clinical benefit in patients with poor prognostic features (Table 10).
Figure 4. Study design of CONKO-003: patients with
gemcitabine refractory pancreatic cancer.
FF: 5-FU 2 g/m2 (24 h) plus FA 200 mg/m2 (30 min)
on days 1, 8, 15, and 22
OFF: FF plus oxaliplatin 85 mg/m2, days 8 and 22
FA: folinic acid or leucovorin

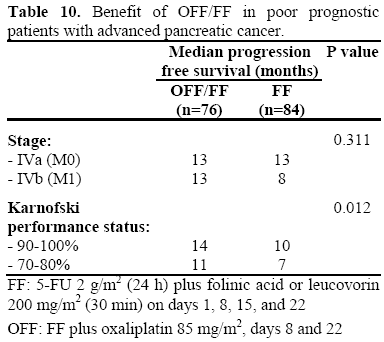
The authors suggested that OFF/FF should be considered standard second-line treatment in patients who progress on gemcitabine.
Conflict of interest
The author has no potential conflicts of interest
References
- Saif MW. Is there a standard of care for the management of advanced pancreatic cancer?. Highlights from the Gastrointestinal Cancers Symposium. Orlando, FL, USA. January 25-27, 2008. JOP. J Pancreas (Online) 2008; 9:91-8. [PMID 18326919]
- Strimpakos A, Saif MW, Syrigos KN. Pancreatic cancer: from molecular pathogenesis to targeted therapy. Cancer Metastasis Rev 2008 Apr 22. [PMID 18427734]
- Neuhaus P, Riess H, Post S, Gellert K, Ridwelski K, Schramm H, et al. CONKO-001: Final results of the randomized, prospective, multicenter phase III trial of adjuvant chemotherapy with gemcitabine versus observation in patients with resected pancreatic cancer (PC). J ClinOncol 26: 2008 (May 20 suppl; abstr LBA4504).
- Loehrer PJ, Powell ME, Cardenes HR, Wagner L, Brell JM, Ramanathan R K, et al. A randomized phase III study of gemcitabine in combination with radiation therapy versus gemcitabine alone in patients with localized, unresectable pancreatic cancer: E4201. J ClinOncol 26: 2008 (May 20 suppl; abstr 4506).
- Vervenne W, Bennouna J, Humblet Y, Gill S, Moore MJ, Van Laethem J, et al. A randomized, double-blind, placebo (P) controlled, multicenter phase III trial to evaluate the efficacy and safety of adding bevacizumab (B) to erlotinib (E) and gemcitabine (G) in patients (pts) with metastatic pancreatic cancer. J ClinOncol 26: 2008 (May 20 suppl; abstr 4507).
- Pelzer U, Kubica K, Stieler J, Schwaner I, Heil G, Görner M, et al. A randomized trial in patients with gemcitabine refractory pancreatic cancer. Final results of the CONKO 003 study. J ClinOncol 26: 2008 (May 20 suppl; abstr 4508).
- Saif MW. Controversies in the adjuvant treatment of pancreatic adenocarcinoma. JOP. J Pancreas (Online) 2007; 8:545-52. [PMID 17873458]
- Kim R, Saif MW. Is there an optimal neoadjuvant therapy for locally advanced pancreatic cancer? JOP. J Pancreas (Online) 2007; 8:279-88. [PMID 17495356]
- Chauffert B, Mornex F, Bonnetain F, Triboulet JP, Bouche O, Rougier P, et al. Phase III trial comparing initial chemoradiotherapy (intermittent cisplatin and infusional 5-FU) followed by gemcitabine vs. gemcitabine alone in patients with locally advanced non metastatic pancreatic cancer: A FFCD-SFRO study. J ClinOncol 2006; 24(18S, Part I):4008. ASCO Annual Meeting.
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as firstline therapy for patients with advanced pancreas cancer: a randomized trial. J ClinOncol 1997; 15:2403-13. [PMID 9196156]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J ClinOncol 2007; 25:1960-6. [PMID 17452677]
- Kindler HL, Friberg G, Singh DA, Locker G, Nattam S, Kozloff M, et al. Phase II trial of bevacizumab plus gemcitabine in patients with advanced pancreatic cancer. J ClinOncol 2005; 23:8033-40. [PMID 16258101]
- Kang SP, Saif MW. Optimal second line treatment options for gemcitabine refractory advanced pancreatic cancer patients. Can we establish standard of care with available data? JOP. J Pancreas (Online) 2008; 9:83- 90. [PMID 18326918]





