Keywords
Diabetes Mellitus, Type 2; Pancreas
Abbreviation
BP blood pressure; NAFLD non-alcoholic fatty liver
disease; NAFPD non-alcoholic fatty pancreas disease; T2DM type 2
diabetes mellitus; WC waist circumference
Introduction
Nonalcoholic fatty pancreas disease (NAFPD) is an
excessive lipid accumulation in the pancreas in the absence
of significant alcohol intake [1]. It is usually an incidental
finding during transabdominal ultrasound examination and its clinical significance is still poorly understood.
Prevalence of NAFPD has been reported in Asia as well as
in Western countries. In Taiwan, Wang et al. reported that
16% of Chinese population had fatty pancreas [2]. In USA,
Sepe et al. reported as high as 27.8% of the patients who
underwent EUS evaluation had NAFPD [3]. In Indonesia,
which represents the biggest Southeast Asian country, the
prevalence of NAFPD in the medical check-up population
was 35% [4].
Previous studies had shown that NAFPD is associated
with T2DM [5, 6, 7, 8, 9, 10, 11]. As a consequence of insulin
resistance, pancreatic beta cells will produce more insulin.
Beta cells apoptosis will occur as it were exhausted. Then,
this empty area will be replaced by adipose tissue [9].
Moreover, hyperglycemia via malonyl-CoA inhibits beta
oxidation of fatty acids in the cell mitochondria. These unoxidized fatty acids will accumulate as intracellular
triglycerides and develop into NAFPD [12]. It will further
decrease beta cell function in T2DM patients [13, 14].
Pancreatic cancer is still the most lethal cancer in the
world. The known risk factors for pancreatic cancer include
tobacco exposure, longstanding diabetes mellitus, obesity,
advanced age, exposure to benzenes, family history, and
chronic pancreatitis [15, 16]. NAFPD may allegedly develop
into chronic pancreatitis and further leads to pancreatic
cancer [17, 18, 19, 20], and facilitates its dissemination
[21]. Patients with type 2 DM have a 2-fold increase in the
risk of pancreatic cancer [22, 23, 24]. Therefore, T2DM
patients with NAFPD should be considered for pancreatic
cancer screening and surveillance.
Factors which are known to be associated with
NAFPD in general population include male, age over 60
years, hypertension, fasting blood glucose, triglycerides,
body mass index, central obesity and nonalcoholic
fatty liver disease (NAFLD) [2, 3, 6, 8, 9, 10, 25, 26].
However, previous studies provided inconsistent results
regarding the association of NAFPD with age [3], sex [2, 25], hypertension [2, 25], hypertriglyceridemia [25], and
NAFLD [9, 10]. These inconsistent results may be due to
difference in diagnostic methods, small sample size in
some studies and its retrospective design. The aim of
our study was to prospectively determine the prevalence
of NAFPD in T2DM population at Cipto Mangunkusumo
Hospital (RSCM) Jakarta and to determine the associations
of NAFPD with age, sex, duration of diabetes, presence of
NAFLD, hypertension, hypertriglyceridemia, and HbA1C
level.
Methods
Study Design and Subject
This was a cross-sectional study in adult T2DM patients
(age of 18 or older) who visited diabetes outpatient clinic at
Cipto Mangunkusumo National Referral Hospital between
January and February 2017. Subjects were recruited
consecutively. Subjects with alcohol consumption ≥20
gram per day in the past year; chronic pancreatitis; or nonvisualized
pancreas on ultrasound were excluded.
Sample Size
By using the formula to count a single proportion
in a population, the minimum sample size to detect
the proportion of NAFPD in T2DM population was 80.
While by using the formula to detect difference in two
unpaired proportions, the minimum sample size to define
the association of various factors with NAFPD in T2DM
patients was 160.
Data Collection
Data collection includes age, sex, and duration of DM,
comorbid, alcohol consumption, and medication used. Each
subject’s waist circumference (WC) and blood pressure
(BP) were measured. The WC (to the nearest 0.1 cm) was
performed at the end of normal expiration on bare skin midway between the lower rib margin and the iliac crest.
Central obesity was defined as WC ≥90 cm in male and ≥80
cm in female. Two blood pressure readings separated by
intervals of at least 5 minutes were performed after the
subject took a minimum of 5 minutes rest and were taken
in a sitting position with an appropriate-sized cuff wrapped
around the right upper arm using calibrated digital
tensimeter (Omron HEM 7221, Japan). Hypertension was
defined as on blood pressure lowering drug(s), or systolic
blood pressure ≥140 mmHg or diastolic blood pressure
≥90 mm Hg according to the Seventh Report of the Joint
National Committee on Prevention, Detection, Evaluation,
and Treatment of High Blood Pressure.
After an overnight 12-hour fast, all subjects underwent
blood test for serum triglyceride and HbA1C levels. HbA1C
was measured by immunoturbidimetry method and
serum triglyceride was measured by glycerol-3-phosphate
oxidase phenol aminophenazone method, both of them
using automatic clinical chemistry analyzer (Roche, Cobas
501, Germany).
Diagnosis of Fatty Pancreas
All subjects underwent transabdominal
ultrasonography in the hepatobilliary division by a junior
consultant and re-evaluated by a senior consultant who
was blind to the subjects’ information. The ultrasound
was done with high-resolution ultrasonography (GE Logic
P6, US) using a convex 3.5-MHz transducer, followed the
ultrasonography protocol that had been made before. The
protocol stated that problems with bowel gas overlying
the pancreas can be overcome by some ways, include deep
inspiration or expiration; distend the abdomen against
the probe (ask the patient to push their stomach out as
if they are pregnant); give the patient an oral waterload
(2-3 glasses of water is used as a window to look through
when it is in the stomach and duodenum); and scan with
the patient erect if needed.
Diagnostic criteria for fatty pancreas is an increase
echogenicity of the pancreatic body parenchymal over
that of the kidney [2, 6, 27]. Since pancreas could not be
visualized in the same window with kidney, the examiner
compared the echogenicity between liver and right kidney
first, then compared the differences between liver and
pancreatic echogenicity to obtain an pancreatorenal
echo contrast. Increased deposition of fat that infiltrated
along the pancreatic septa, has been shown to be a major
determining factor of pancreatic echogenicity in one study
evaluating pancreatic echogenicity and its correlation
with the morphologic appearance of the pancreas in
computed tomography [28]. Therefore, it is reasonable
to conclude that the “fatty pancreas” found on ultrasound
examination is associated with increased fat accumulation
pathologically.
Ethics
The research protocol was approved by the Institutional
Review Board of Cipto Mangunkusumo Hospital and this
study was carried out without any linkage of personal information for all participants. We obtained written
informed consent the patients for publication of this report.
Statistical Analysis
All subjects were classified into either the NAFPD or
the non–NAFPD group as dependent variable and were
divided by age (<60 or ≥60 years-old), sex (male or
female), duration of diabetes (<5 or ≥5 years), absence or
presence of NAFLD and hypertension, HbA1C levels (<7.0
or ≥7.0) and serum triglycerides (<150 m/dL or ≥150 mg/
dL) as independent variables. Chi Square test was used for
bivariate analysis and binary logistic regression was used
for multivariate analysis. A p value <0.05 was considered
statistically significant. All statistical analyses were
performed with SPSS 21.0.
Results
From 191 participants enrolled in the study, 171
subjects were suitable for the data analysis (Figure 1). The
characteristics of all study subjects is shown in Table 1.
Figure 1. Recruitment of subjects.
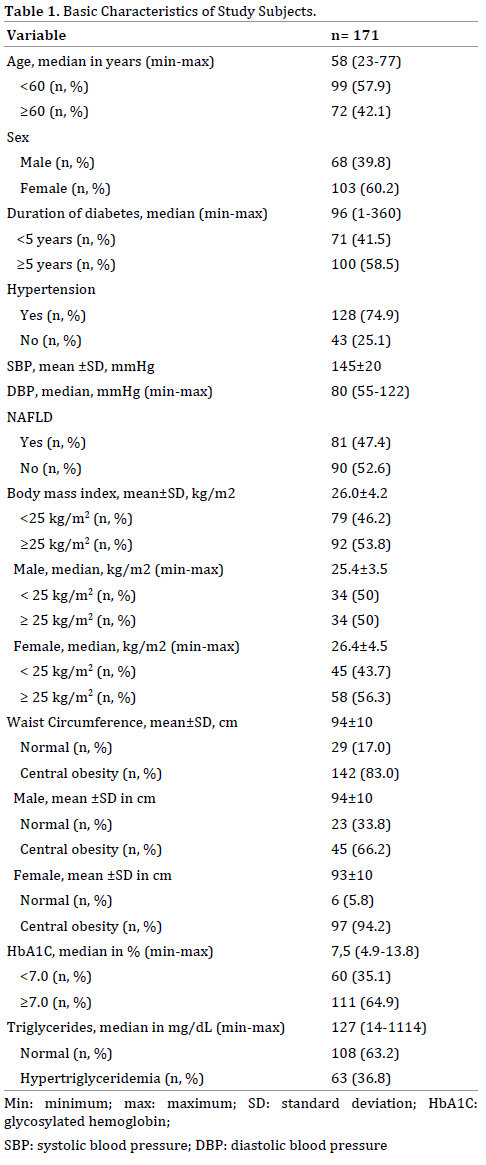
NAFPD was found in 83 (48.5%; 95%CI=41.2-55.9%)
subjects, consist of 34 (41%) male and 49 (59%) female.
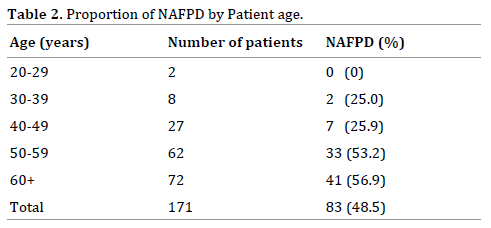
The prevalence of NAFPD is more frequent with increasing
age (Table 2). Concurrence of NAFPD and NAFLD on
abdominal ultrasound was found in 53 patients (31%).
Factors associated with NAFPD on bivariate analysis
were NAFLD (PR=1.96; 95%CI=1.41-2.74; p<0.001)
and hypertriglyceridemia (PR=1.38; 95%CI=1.02-1.86;
p=0.042) (Table 3).
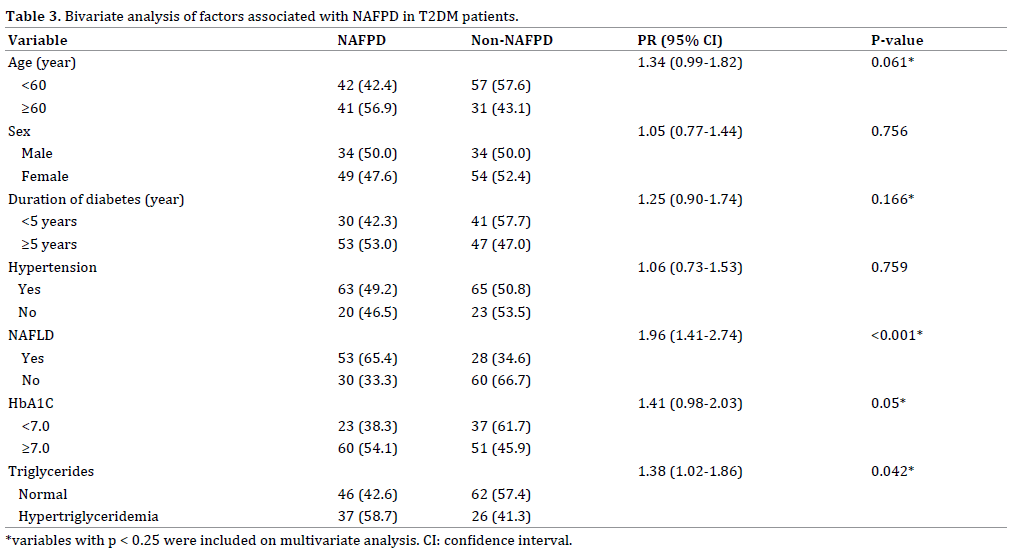
Variables with a p value of less than 0.25 (*) ie age,
duration of diabetes, NAFLD, HbA1C and triglycerides
were included in multivariate analysis. On stepwise binary
logistic regression analysis, factors associated with NAFPD
in T2DM patients were NAFLD (OR=3.65; 95%CI=1.90-
6.99), age ≥60 years (OR=2.15; 95%CI=1.10-4.23) and
hypertriglyceridemia (OR=2.03; 95%CI=1.02-4.05).
Discussion
To our knowledge, this is the first prospective study
aimed to find the proportion of NAFPD in T2DM population
and its associated factors. Our study demonstrated
the big proportion of NAFPD in T2DM patients. Recent
meta-analysis also showed that there was a significant
relationship between NAFPD and T2DM (RR 2.08;
95%CI=1.44-3; p <0.001) [29].
Fatty replacement on pancreas was an inevitable aging
process [20, 27, 30]. This was confirmed by our finding
that NAFPD was more frequent with increasing age. Other
studies using cut off of 60 year-old age [26] and 35 yearold
age [4] also showed an association of NAFPD with age.
(OR=2.87; 95%CI=1.54-5.37 and OR=4.01; 95%CI=2.82-
5.70). Therefore, older age is considered as an important
risk factor of NAFPD.
On the contrary to the previous studies [4, 26], our
study showed no association of male gender and NAFPD.
It was hypothesized that men are at higher risk to develop NAFPD because they had more visceral (abdominal) fat
deposition while women had more subcutaneous (glutealfemoral)
lipid deposition [26, 31]. However, in our study
there were more centrally obese women (94.4%) than men
(66.2%). Majority of female subjects in this study were at
monopausal age (above 50 years-old). It had been known
that in menopausal woman, fat distribution changed from a
gluteo-femoral pattern into a centrally dominant (viseral)
pattern due to hormonal changes [31]. Distribution of
T2DM patients by age in other countries might be different
from ours, so it’s not generalizable to all T2DM patients.
In this study, we found no significant association of
NAFPD with duration of diabetes and HbA1C. It may be
due to the 2-way relationship between NAFPD and T2DM.
NAFPD may occur long time before the onset of type 2
diabetes. This was supported by a study which revealed
that pancreatic fat deposition had already been found in
the prediabetic phase before the onset of T2DM [32]. Our
findings also suggested that insulin resistance play a more
important role in the development of NAFPD compared to
hyperglycemia.
Hypertension which was known to be a risk factor
of NAFPD in previous studies [2, 4, 26] was also not
associated with NAFPD in our study subject. This can be
explained by the fact that insulin resistance had occurred
in T2DM patients long time before they was diagnosed
[33, 34, 35], then metabolic syndrome parameters such as
hypertension might be found in T2DM patients either with
or without NAFPD. Therefore, hypertension which in the
general population was a risk factor of NAFPD could not be
used as a predictor of NAFPD in T2DM patients.
Consistent with the findings from earlier studies
[2, 3, 4], hypertriglyceridemia and NAFLD were also
associated with NAFPD in our study. In the state of insulin
resistance, excessive free fatty acids [36] were brought and accumulated into various visceral organs including
the liver (NAFLD) and pancreas (NAFPD) [37]. Our finding
indicated that NAFPD and NAFLD may had the same risk
factors leading to fat accumulation in both organs. Thus,
the presence of NAFLD may be a predictor of NAFPD in
T2DM patients.
This study has several limitations. Owing to its
cross-sectional design, we could not determine causal
relationship between NAFPD and the variables studied.
But this study has given a new insight of metabolic factors
associated with NAFPD, which should be considered as
a new risk factor for pancreatic cancer development.
Furthermore, the pathophysiology of NAFPD is still not fully
understood so that other factors that may play a role could
be not included in this study. Diagnosis of fatty pancreas
in this work was made with transabdominal ultrasound
examinations without any histologic confirmation.
However, doing pancreatic biopsy in a healthy subject is
unethical. The major drawbacks of ultrasound include
operator dependency and insensitivity with regard to
small amounts of fat. However, it has been proven as
a reliable, reproducible and non-invasive screening
tool for NAFPD in previous studies [2, 4, 6, 8, 38, 39, 40]. Zhou et al. (n=1190) randomly selected 50 people
diagnosed with NAFPD by an abdominal ultrasound to
undergo MRI examination and found consistent results
[39]. Therefore we still use abdominal ultrasound in this
study. Finally, we did not use grading system to assess
pancreatico-renal echo contrast. Sepe et al. [3] define
the degree of fatty pancreas by using 3 criteria include
pancreatic echogenicity, clarity of the parenchyma and
pancreatic duct margins. But, to our knowledge, this
only can be done by using endoscopic ultrasound not by
trans-abdominal ultrasound.
Basic characteristics of our study population resembles
that of T2DM patients in 18 secondary and tertiary health
care centers in Indonesia [41], and also in community [42],
so it is generalizable to all patients with type 2 diabetes in
Indonesia.
Conclusion
The proportion of NAFPD in T2DM patients in Cipto
Mangunkusumo National Referral Hospital was 48.5%.
Presence of NAFLD, hypertriglyceridemia and older age
were factors associated with NAFPD in T2DM patients.
Screening of NAFPD should be considered to be performed
on T2DM patients with those conditions. A prospective
longitudinal study is needed to reveal the natural course
of NAFPD in T2DM population and its unknown risk
factors. We also suggested that greater number of patients
included in further study by using abdominal tomography
to better evaluate the fat infiltrative pancreatic disease.
Acknowledgments
We thank Hepatobilliary Division Junior Consultants
for their sincerely help and Mrs. Utami S. for helpful advice.
Conflict of Interest
We declare that we have no conflict of interests.
References
- Alempijevic T, Dragasevic S, Zec S, Popovic D, Milosavljevic T. Nonalcoholic
fatty pancreas disease. Postgrad Med J 2017; 93:226-230.
[PMID: 28069746]
- Wang CY, Ou HY, Chen MF, Chang TC, Chang CJ. Enigmatic ectopic
fat: prevalence of nonalcoholic fatty pancreas disease and its associated
factors in a Chinese population. J Am Heart Assoc 2014; 3:297–304.
[PMID: 24572250]
- Sepe PS, Ohri A, Sanaka S, Berzin TM, Sekhon S, Bennett G, et al. A
prospective evaluation of fatty pancreas by using EUS. Gastrointest
Endosc 2011; 73:987–93. [PMID: 21521567]
- Lesmana CR, Pakasi LS, Inggriani S, Aidawati ML, Lesmana LA.
Prevalence of non-alcoholic fatty pancreas disease (NAFPD) and its risk
factors among adult medical check-up patients in a private hospital: a
large cross sectional study. BMC Gastroenterol 2015; 15:1–5. [PMID:
26652175]
- Wong VW, Wong GL, Yeung DK, Abrigo JM, Kong AP, Chan RS, et al.
Fatty pancreas, insulin resistance, and β-cell function: a population study
using fat-water magnetic resonance imaging. Am J Gastroenterol 2014;
109:589–97. [PMID: 24492753]
- Lee JS, Kim SH, Jun DW, Han JH, Jang EC, Park JY, et al. Clinical implications
of fatty pancreas: Correlations between fatty pancreas and metabolic
syndrome. World J Gastroenterol 2009; 15:1869–75. [PMID: 19370785]
- Milburn JL, Hirose H, Lee YH, Nagasawa Y, Ogawa A, Ohneda M, et
al. Pancreatic cells in obesity: evidence for induction of functional,
morphologic, and metabolic abnormalities by increased long chain fatty
acids. J Biol Chem 1995; 270:1295–9. [PMID: 7836394]
- Wu WC, Wang CY. Association between non-alcoholic fatty pancreatic
disease (NAFPD) and the metabolic syndrome: case–control retrospective
study. Cardiovasc Diabetol 2013; 12:77. [PMID: 23688357]
- Tushuizen ME, Bunck MC, Pouwels PJ, Bontemps S, van Waesberghe
JHT, Schindhelm RK, et al. Pancreatic fat content and beta-cell function in
men with and without type 2 diabetes. Diabetes Care 2007; 30:2916–21.
[PMID: 17666465]
- Heni M, Machann J, Staiger H, Schwenzer NF, Peter A, Schick F,
et al. Pancreatic fat is negatively associated with insulin secretion in
individuals with impaired fasting glucose and/or impaired glucose
tolerance: a nuclear magnetic resonance study. Diabetes Metab Res Rev
2010; 26:200–5. [PMID: 20225188]
- Newcastle Unversity. Type 2 diabetes reversed by losing fat from
pancreas. ScienceDaily [Internet]. 2015 [cited 2017 Mar 14]; Available from:
https://www.sciencedaily.com/releases/2015/12/151201141231.htm
- Rasmussen BB, Holmbäck UC, Volpi E, Morio-Liondore B, Paddon-
Jones D, Wolfe RR. Malonyl coenzyme A and the regulation of functional
carnitine palmitoyltransferase-1 activity and fat oxidation in human
skeletal muscle. J Clin Invest 2002; 110:1687–93. [PMID: 12464674]
- Robertson RP, Harmon J, Tran POT, Poitout V. Beta-cell glucose
toxicity, lipotoxicity, and chronic oxidative stress in type 2 diabetes.
Diabetes 2004; 53 Suppl 1:119–24. [PMID: 14749276]
- Shimabukuro M, Zhou YT, Levi M, Unger RH. Fatty acid-induced beta
cell apoptosis: a link between obesity and diabetes. Proc Natl Acad Sci U S
A 1998; 95:2498–502. [PMID: 9482914]
- Becker AE, Hernandez YG, Frucht H, Lucas AL. Pancreatic ductal
adenocarcinoma: Risk factors, screening, and early detection. World J
Gastroenterol 2014; 20:11182–98. [PMID: 25170203]
- Andersen DK, Andren-Sandberg A, Duell EJ, Goggins M, Korc M,
Petersen GM, et al. Pancreatitis, diabetes, pancreatic cancer: summary of
an NIDDK-NCI workshop. Pancreas 2013; 42. [PMID: 24152948]
- Hori M, Takahashi M, Hiraoka N, Yamaji T, Mutoh M, Ishigamori
R, et al. Association of Pancreatic Fatty Infiltration With Pancreatic
Ductal Adenocarcinoma. Clin Transl Gastroenterol 2014; 5:1–5. [PMID:
24622469]
- Tomita Y, Azuma K, Nonaka Y, Kamada Y, Tomoeda M, Kishida M, et
al. Pancreatic fatty degeneration and fibrosis as predisposing factors for
the development of pancreatic ductal adenocarcinoma. Pancreas 2014;
43:1032–41. [PMID: 24991971]
- Rebours V, Gaujoux S, d’ Assignies G, Sauvanet A, Ruszniewski P,
Levy P, et al. Obesity and Fatty Pancreatic Infiltration Are Risk Factors
for Pancreatic Precancerous Lesions (PanIN). Clin Cancer Res 2015;
21:3522–8. [PMID: 25700304]
- Mathur A, Marine M, Lu D, Swartz-Basile DA, Saxena R, Zyromski NJ,
et al. Nonalcoholic fatty pancreas disease. HPB 2007; 9:312–8. [PMID:
18345311]
- Mathur A, Zyromski NJ, Pitt HA, Al-Azzawi H, Walker JJ, Saxena R, et al.
Pancreatic steatosis promotes dissemination and lethality of pancreatic
cancer. J Am Coll Surg 2009; 208:989–96. [PMID: 19476877]
- Huxley R, Ansary-Moghaddam A, Berrington de González A, Barzi F,
Woodward M. Type-II diabetes and pancreatic cancer: a meta-analysis of
36 studies. Br J Cancer 2005; 92:2076–83. [PMID: 15886696]
- Chari ST, Leibson CL, Rabe KG, Ransom J, de Andrade M, Petersen GM.
Probability of pancreatic cancer following diabetes: a population-based
study. Gastroenterology 2005; 129:504–11. [PMID: 18061176]
- Jee SH, Ohrr H, Sull JW, Yun JE, Ji M, Samet JM. Fasting Serum Glucose
Level and Cancer Risk in Korean Men and Women. JAMA 2005; 293:194–
202. [PMID: 15644546]
- Al-Haddad M, Khashab M, Zyromski N, Pungpapong S, Wallace MB,
Scolapio J, et al. Risk factors for hyperechogenic pancreas on endoscopic
ultrasound: a case-control study. Pancreas 2009; 38:672–5. [PMID:
19506531]
- Choi CW, Kim GH, Kang DH, Kim HW, Kim DU, Heo J, et al. Associated
factors for a hyperechogenic pancreas on endoscopic ultrasound. World J
Gastroenterol 2010; 16:4329–34. [PMID: 20818817]
- Tariq H, Nayudu S, Akella S, Glandt M, Chilimuri S. Non-Alcoholic
Fatty Pancreatic Disease: A Review of Literature. Gastroenterol Res 2016;
9:87–91. [PMID: 28058076]
- Ogilvie RF. The islands of langerhans in 19 cases of obesity. J Pathol
Bacteriol 1933; 37:473–81.
- Singh RG, Yoon HD, Wu LM, Lu J, Plank LD, Petrov MS. Ectopic fat
accumulation in the pancreas and its clinical relevance: A systematic
review, meta-analysis, and meta-regression. Metab Clin Exp 2017; 69:1–
13. [PMID: 28285638]
- Chantarojanasiri T, Hirooka Y, Ratanachu-ek T, Kawashima H, Ohno
E, Goto H. Evolution of pancreas in aging: degenerative variation or early
changes of disease? J Med Ultrason 2015; 42:177–83. [PMID: 26576570]
- Blaak E. Gender differences in fat metabolism. Curr Opin Clin Nutr
Metab Care 2001; 4:499–502. [PMID: 11706283]
- Lingvay I, Esser V, Legendre JL, Price AL, Wertz KM, Adams-Huet
B, et al. Noninvasive quantification of pancreatic fat in humans. J Clin
Endocrinol Metab 2009; 94:4070–6. [PMID: 19773401]
- McGarry JD. Banting lecture 2001: dysregulation of fatty acid
metabolism in the etiology of type 2 diabetes. Diabetes 2002; 51:7–18.
[PMID: 11756317]
- Kahn SE, Hull RL, Utzschneider KM. Mechanisms linking obesity to
insulin resistance and type 2 diabetes. Nature 2006; 444:840–6. [PMID:
17167471]
- DeFronzo RA, Ferrannini E. Insulin Resistance: A Multifaceted
Syndrome Responsible for NIDDM, Obesity, Hypertension, Dyslipidemia,
and Atherosclerotic Cardiovascular Disease. Diabetes Care 1991; 14:173–
94. [PMID: 2044434]
- Mooradian AD. Dyslipidemia in type 2 diabetes mellitus. Nat Clin
Pract Endocrinol Metab 2009; 5:150–9. [PMID: 19229235]
- Bradbury MW. Lipid metabolism and liver inflammation. I. Hepatic
fatty acid uptake: possible role in steatosis. Am J Physiol Gastrointest
Liver Physiol 2006; 290:G194–8. [PMID: 16407588]
- Uygun A, Kadayifci A, Demirci H, Saglam M, Sakin YS, Ozturk K, et al.
The effect of fatty pancreas on serum glucose parameters in patients with
nonalcoholic steatohepatitis. Eur J Intern Med 2015; 26:37-41. [PMID:
25491010]
- Zhou J, Li ML, Zhang DD, Lin HY, Dai XH, Sun XL, et al. The correlation
between pancreatic steatosis and metabolic syndrome in a Chinese
population. Pancreatology 2016; 16:578–83. [PMID: 27050733]
- Ou HY, Wang CY, Yang YC, Chen MF, Chang CJ. The Association
between Nonalcoholic Fatty Pancreas Disease and Diabetes. PLoS ONE
2013; 8:1–9. [PMID: 23671610]
- Soewondo P, Soegondo S, Suastika K, Pranoto A, Soeatmadji DW,
Tjokroprawiro A. The DiabCare Asia 2008 study – Outcomes on control
and complications of type 2 diabetic patients in Indonesia. Med J Indones
2010; 19:235–44. [PMCID: PMC3901560]
- Badan Penelitian dan Pengembangan Kesehatan Kementerian
Kesehatan Republik Indonesia. Riset Kesehatan Dasar. Kementerian
Kesehatan RI; 2013 [cited 2016 Jul 19]. 16 p. Available


