Keywords
Carcinoma, Pancreatic Ductal; gemcitabine; Immune System; Molecular Targeted Therapy
Abbreviations
MEK 1/2: mitogen-activated protein kinase (MAPK), extracellular signal-regulated protein kinase (ERK)
What Did We Know Before the 2012 American Society of Clinical Oncology (ASCO) Annual Meeting?
The current approved cytotoxic treatments for advanced pancreatic cancer include the antimetabolite gemcitabine combined often with a fluoropyrimidine or a platinum agent and 5-fluorouracil, leucovorin, irinotecan, oxaliplatin (FOLFIRINOX) [1, 2, 3]. As far as the biological agents are concerned, only erlotinib demonstrated a small, but significant, added benefit to chemotherapy [4]. Despite Kirsten rat sarcoma (KRAS) mutations are so frequently observed in pancreatic cancer, we have not managed to tackle its aberrant pathway in a clinical meaningful way. Regarding the role of immunotherapy we hope that, similarly to the recent advances in the management of metastatic melanoma, new prospects will open in pancreatic cancer too. The studies that are presented below add new information on how we approach this disease.
What Have We Learnt from the 2012 American Society of Clinical Oncology (ASCO) Annual Meeting?
Interesting pharmacokinetic and pharmacodynamic data on novel biological treatments (Figure 1) and chemotherapy-based combinations are presented here, which we hope that will become a platform for use in clinical efficacy studies in near future.
Figure 1. Mode of action of some of the novel agents (stars)
(adapted and modified with permission from Rustgi AK, Genes Dev
2006; 20:3049-53. [9]).
Studies on Treatments Stimulating the Immune System
Two of the phase I studies on pancreatic cancer presented at the 2012 ASCO Annual Meeting were based on principles of immunotherapy (Table 1).
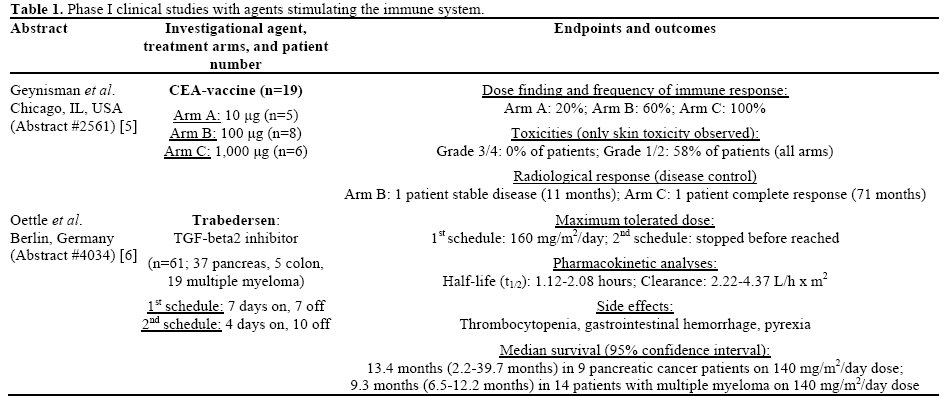
The first one explored the appropriate dose of a CEAbased vaccine which was made by a modified carcinoembryonic antigen peptide (CAP1-6D) in conjunction with the adjuvant cytokine granocyte macrophage-colony stimulating factor (GM-CSF) and the oil adjuvant montanide (Abstract #2561) [5]. This cytokine-enriched vaccine was designed to overcome the natural immune tolerance to CEA molecule, which is found to be overexpressed in the vast majority of pancreatic cancers. Patients included in this study needed to be pretreated, with very good performance status, to expressed CEA and also to express the human leukocyte antigen A2 (HLA-A2) on their tissue specimen. From the 66 screened patients, 19 were expressing the HLA-A2 serotype and were randomized in three arms (A, B, C) receiving different CEAvaccine doses (10 μg, 100 μg and 1,000 μg, respectively), every two weeks until disease progression or a maximum of 24 doses. The design, end-points and the results of this study are highlighted in Table 1. In conclusion, this phase I study showed that the CEA-based vaccine at the higher tested dose was tolerated and able to produce a satisfactory immune response as well as evidence of clinical activity that warrants further evaluation.
The second study related to immune system, tested the safety, pharmacokinetic and pharmacodynamic properties of trabedersen on patients diagnosed with pancreatic cancer, colorectal cancer and malignant melanoma (Abstract #4034) [6]. Trabedersen is an inhibitor of the tissue growth factor-beta 2 (TGFbeta2). This growth factor is overexpressed in many malignancies and attenuates the immune reaction and response of the host to cancer cells. The study was designed with a phase I and phase II part. Patients with disease progression after two to four previous lines of treatment were treated with two dose escalation schemes of intravenous trabedersen. The treatment details and study results are demonstrated in Table 1. The experimental treatment showed a very safe profile and was tolerated by the majority of patients. Furthermore, some early efficacy results suggest probable activity in patients with pancreatic cancer and melanoma.
Studies on Agents Improving the Role of Cytotoxic Treatment
In two phase I studies reported in this year’s ASCO Annual Meeting, agents improving the role or the method of administration of gemcitabine were investigated (Table 2).
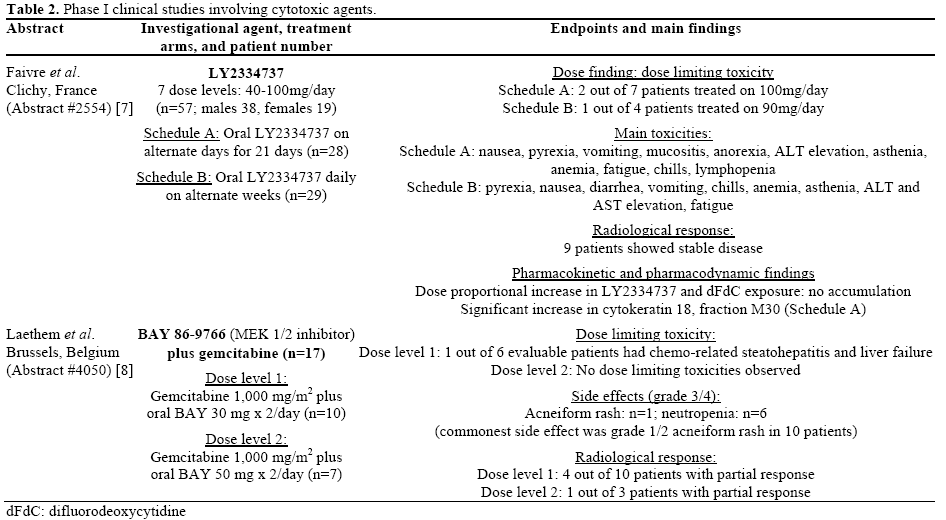
First, the optimal dose and schedule of administration of LY2334737, an oral pro-drug of gemcitabine, was explored in Abstract #2554 [7]. Secondary endpoints of the study included the pharmacokinetic and pharmacodynamic properties of this agent. Patients with good performance status and satisfactory organ function received LY2334737 (7 dose levels, from 40 mg to 100 mg) on two different schedules (A: on alternate days for 21days; B: daily on alternate weeks). The patients’ characteristics, treatment details and finding of the study are presented in Table 2. The authors of this early phase I study suggested that 90 mg of LY2334737, given every other day, should be the recommended dose for subsequent phase II trials.
The second phase I study involving a cytotoxic treatment, investigated the pharmacokinetic properties and the maximum tolerated dose of the combination of gemcitabine with the oral mitogen-activated protein kinase (MAPK), extracellular signal-regulated protein kinase (ERK) (MEK 1/2) inhibitor named BAY 86- 9766 (Abstract #4050) [8]. Seventeen patients with advanced pancreatic cancer were enrolled in the phase I part of this phase I/II study with a 3+3 design. The patients received gemcitabine in its usual fashion (7 weeks on, 1 week off on cycle 1 and then 3 weeks on, 1 off) along with oral BAY 86-9766 30 mg or 50 mg twice a day. The treatment was well tolerated with only one serious dose limiting toxicity on a patient who developed chemotherapy associated steatohepatitis, liver failure and succumbed. The commonest side effects were neutropenia and acneiform rash, which were also manageable.
Discussion
Little progress has been made in the treatment of pancreatic cancer as compared to other solid tumors. The biological pathways seem to be very complex and the various novel agents against the identified molecular targets have not proven very helpful. Therefore, early diagnosis and optimal resection of the tumor remains the most optimistic scenario, but this applies only for the minority of pancreatic cancer patients. For the vast majority though, soon after the diagnosis and their initial treatment the only realistic but also promising pathway one can follow is the participation in clinical trials testing new agents, which in addition probably to one of the standard drugs might improve their chances for a longer survival. The role of immunotherapy has been broadly explored in the management of neoplastic disorders. So far, we have been facing more disappointments than achievements in the immunotherapy field, but recent advances in the management of metastatic melanoma, with the clinical important role of ipilimumab, our interest on vaccines purposed to stimulate the immune-mediated control of cancer has been re-instated. One hurdle to the success of immunotherapy is the lack of precise biomarkers to select the patients’ populations who might benefit the most from this concept. The search for biomarkers could be a collateral task in these early phase clinical studies, in order to prevent from performing likely unsuccessful trials and wasting of resources. The invention of biomarkers on immune therapies could both facilitate and accelerate the development of “personalized” studies and a true individualized management. The potential of the antisense agent trabedersen in pancreatic carcinoma, by blocking the production of a protein (e.g., TGF-beta2) involved in the progression and metastasis of this aggressive malignancy, is really intriguing and the clinical results very much anticipated.
Of great importance is also the development of an oral pro-drug of gemcitabine, which has been for many years the core cytotoxic in the management of pancreatic cancer. A well tolerated and usually convenient oral cytotoxic, providing it proves its efficacy, might improve the quality of life of these very affected by the disease patients.
Finally, the combination of a standard cytotoxic with a biological agent of the EGFR downstream pathway is usually feasible without much unpredictable toxicity. Although, most of the late phase clinical studies with a biological turned out to be ineffective, the combination of gemcitabine with the MEK 1/2 inhibitor showed promising results which deserve further exploration.
It will be of great interest to see results of phase II and III clinical trials on these agents and particularly the subgroup of pancreatic cancer patients who derive the greatest benefit.
Conflict of interest
The authors have no potential conflicts of interest
References
- Sultana A, Smith CT, Cunningham D, Starling N, Neoptolemos JP, Ghaneh P. Meta-Analyses of Chemotherapy for Locally Advanced and Metastatic Pancreatic Cancer. Journal of Clinical Oncology 2007 Jun 20;25(18):2607-15.
- Strimpakos A, Saif MW, Syrigos KN. Pancreatic cancer: from molecular pathogenesis to targeted therapy. Cancer Metastasis Rev 2008 Sep;27(3):495-522.
- Conroy T, Desseigne F, Ychou M, Bouche O, GuimbaudR,Becouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de la FC, Bennouna J, Bachet JB, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011 May 12;364(19):1817-25.
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, Au HJ, Murawa P, Walde D, Wolff RA, Campos D, Lim R, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007 May 20;25(15):1960-6.
- Geynisman DM, Zha Y, Kunnavakkam R, Aklilu M, Catenacci DVT, Polite BN, Rosenbaum CA, Namakydoust A, Karrison T, Gajewski T, Kindler HL. A randomized pilot phase I study of modified carcinoembryonic antigen (CEA) peptide (CAP1- 6D)/montanide/GM-CSF-vaccine (CEA-vac) in patients (pts) with pancreatic adenocarcinoma (PC). J Clin Oncol 2012; 30(Suppl):Abstract 2561.
- Oettle H, Seufferlein T, Luger T, Schmid RM, von Wichert G, Endlicher E, Garbe C, Kaehler KK, Enk A, Schneider A, Rothhammer-Hampl T, Grosser S, et al. Final results of a phase I/II study in patients with pancreatic cancer, malignant melanoma, and colorectal carcinoma with trabedersen. J Clin Oncol 2012; 30(Suppl):Abstract 4034.
- Faivre SJ, Olszanski AJ, Weigang-Koehler K, Riess H, Peng G, Callies S, Benhadji KA, Raymond E. Phase I and pharmacokinetic (PK)/pharmacodynamic (PD) study of LY2334737, an oral gemcitabine prodrug, in patients (pts) with advanced solid tumors. J Clin Oncol 2012; 30(Suppl):Abstract 2554.
- Van Laethem JL, Heinemann V, Martens UM, Jassem J, Michl P, Peeters M, Weekes CD, Marechal R, Stieler J, Giurescu M, Rajagopalan P, Garosi VL, et al. A phase I/II study of the MEK inhibitor BAY 86-9766 (BAY) in combination with gemcitabine (GEM) in patients with nonresectable, locally advanced or metastatic pancreatic cancer (PC): Phase I dose-escalation results. J Clin Oncol 2012; 30(Suppl):Abstract 4050.
- Rustgi AK. The molecular pathogenesis of pancreatic cancer: clarifying a complex circuitry. Genes & Dev 2006; 20:3049-53.


