Pancreatic neuroendocrine tumors represent a small percentage of all pancreatic tumors (1.3%) but their incidence is rising. Prior to 2011, the only approved agent for unresectable disease was streptozicin (often used in combination with doxorubicin) but the efficacy of this drug is in question and there had not been any new drugs approved for this disease in more than 20 years. Recently there has been new excitement for the treatment of advanced neuroendocrine tumors including those of the pancreas (pNET) with FDA approval of 2 new agents in 2011. One of these agents was everolimus, an mTOR inhibitor, which was approved on the basis of a landmark phase III study (RADIANT-3). At the 2011 American Society of Clinical Oncology (ASCO) Annual Meeting, several abstracts were presented reviewing novel agents in the treatment of advanced NET. Three abstracts looked at characteristics of patients treated on the RADIANT-3 study and looked at the role of prior chemotherapy use (Abstract #4103), somatostatin analog use (Abstract #4010), and updated safety data (Abstract #4009) from this trial. Additionally, an abstract was presented (Abstract 4008) looking at updated data from the other targeted agent approved for advanced pNET, sunitinib, a multi-tyrosine kinase inhibitor, which demonstrated improvement in progression-free survival compared to placebo. Novel agents were also presented, including a phase II trial looking at the combination of sorafenib and bevacizumab (Abstract #4113), and a phase I trial looking at a novel somatostatin analog, pasireotide, in combination with everolimus (Abstract #4120) The authors review and summarize these abstracts in this article.
Keywords
Drug Therapy; everolimus; Neuroendocrine Tumors; Pancreatic Neoplasms
Abbreviations
LAR: long-acting release; RADIANT: RAD001 in Advanced Neuroendocrine Tumors; SSA: somatostatin analog
What Did We Know Before the 2011 American Society of Clinical Oncology (ASCO) Annual Meeting?
Pancreatic neuroendocrine tumors (pNET) represent a small percentage of all pancreatic tumors: 1.3% (with a 9.9% prevalence) [1]; but their incidence is rising [2]: between 1977-1981 to 2002-2005, the incidence rate of endocrine cancer rose more than 100% (P value less than 0.05). This increase was also seen in advanced stage disease (137% increase). The majority of patients are unresectable as pNETs are frequently diagnosed at an advanced stage, with approximately 65% of patients presenting with unresectable or metastatic disease [3]. Prior to 2011, the only approved agent for unresectable disease was streptozocin which was approved prior to 1984 after demonstrating some efficacy in studies in the 1980’s (either alone [4] or in combination with doxorubicin [5]). Further studies have questioned the efficacy of streptozocin [6] and there have not been any new drugs approved in the last 20 years. As a result patients with unresectable pNETs have a poor prognosis. The median survival time for patients with distant metastatic disease is 24 months [3]; the 5-year survival rate of patients with metastatic disease is 30% to 40% [7] and has not changed for 20 years [8].
In April 2011 the FDA approved a new drug for this disease, everolimus, a mammalian target of rapamycin (mTOR) inhibitor. This approval was based on a landmark phase III trial, the “RAD001 in Advanced Neuroendocrine Tumors” study, RADIANT-3, which was first reported at the ASCO GI Symposium in January 2011 [9]. In RADIANT-3 [10], researchers showed that everolimus was superior to placebo in prolonging progression free survival in patients with unresectable, advanced pNET from 4.6 to 11.0 months. Another phase III trial looked at sunitinib in unresectable pNET and found an improvement in progression free survival from 5.5 to 11.4 months when compared to placebo [11]. Both drugs were approved by the FDA in recent months. At the 2011 ASCO Annual Meeting, several abstracts were presented providing follow up data on these trials and on other novel agents in the treatment of advanced NET.
What We Learned at ASCO 2011 Annual Meeting
Updates from RADIANT-3
In two abstracts exploratory analysis of the RADIANT- 3 trial was performed. Shah et al. (Abstracts #4010) [12] looked at whether the use of long acting somatostatin analog (SSA) therapy impacted the improvement of progression free survival that was seen with everolimus compared to placebo. They found that the treatment arms in RADIANT-3 were well balanced between those who received SSAs prior to enrollment (50% in each arm), and during the trial (39% in the everolimus group vs. 40% in the placebo group.) A statistically significant improvement in progression free survival was seen in the everolimus group regardless of pattern of SSA use, including those who never had SSA therapy and those who had SSA therapy while on study. Pommier et al. (Abstracts #4103) [13] looked at whether patients who received chemotherapy had different outcomes compared to those who did not prior to enrolling in RADIANT-3. They found that prior chemotherapy was used in 50% of the patients and that this was equally divided between those who received everolimus (50%) and those who received placebo (49%) (Table 1). The benefit in progression free survival seen with everolimus versus placebo was found in those with and without prior chemotherapy use and this did not impact the beneficial effect of everolimus.
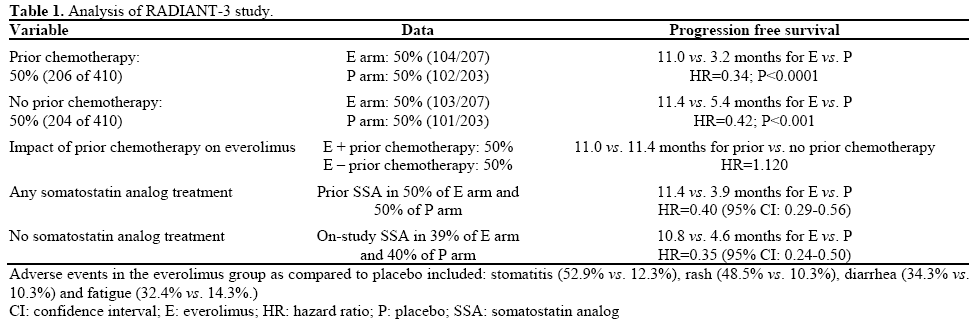
Safety data of the RADIANT-3 trial was reported by Strosberg et al. (Abstract #4009) [14]. At a median follow up of 20.1 months, the updated safety found that grade 3 or 4 adverse events were rare but more frequent in the everolimus group with anemia (5.9%), hyperglycemia (5.9%), and stomatitis (4.9%) being the most common severe adverse events. The most common adverse events overall were stomatitis (52.9% vs. 12.3%), rash (48.5% vs. 10.3%), diarrhea (34.3% vs. 10.3%) and fatigue (32.4% vs. 14.3%) (everolimus vs. placebo, respectively).
Other Agents in Advanced NET
Updated data was also presented regarding the role of sunitinib in prolonging progression free survival in unresectable pancreatic NETs (Table 2). Raymond et al. (Abstract #4008) [15] reported updated results from their trial looking at sunitinib vs. placebo in patients with unresectable NET that had progressed in less than 12 months [11]. In their original report, an improvement in progression-free survival with sunitinib vs. placebo was observed (11.4 vs. 5.5 months; HR: 0.42; P<0.001) but the median over survival was not reached. This updated report included events through June 2010 and found that the median overall survival in the sunitinib arm was 30.5 months compared to 24.4 months in the placebo arm with hazard ratio of 0.737 which was not statistically significant (95% CI: 0.465-1.168; P=0.19). They continued to observe a benefit in median progression free survival of 12.6 vs. 5.8 months for sunitinib vs. placebo, HR: 0.315, P<0.0001 and noted that progression free survival was confirmed by blinded independent central review.
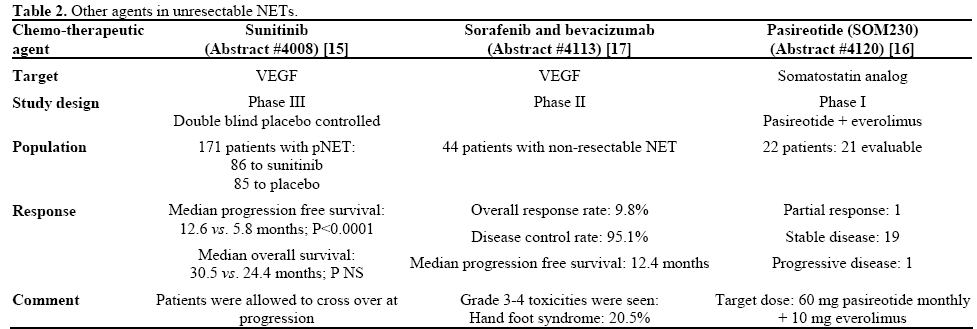
Data regarding novel agents for the treatment of pancreatic NET were also presented. Chan et al. (Abstract #4120) [16] looked at the feasibility of combining a novel somatostatin analog to everolimus for the treatment of advanced NET in a phase I study. They found that pasireotide was tolerated when added to everolimus with dose limiting toxicity of rash and diarrhea (each grade 3) and determined that the dose for further studies is pasireotide 60 mg i.m. monthly with daily everolimus (10 mg). A phase II trial looking at treatment of advanced NET with sorafenib, an oral multi kinase inhibitor which blocks vascular endothelial growth factor (VEGF) and platelet-derived growth factor receptors (PDGFR), and bevacizumab, a monoclonal antibody to VEGF. Castellano et al. (Abstract #4113) [17] reported the results of this phase II trial. Forty-four patients were included; they all had non-resectable NET and had received prior chemotherapy. Response by the Response Evaluation Criteria In Solid Tumors (RECIST) criteria was seen in 9.8% of patients, with disease control rate of 95.1%. Median progression free survival was 12.4 months (95% CI: 9.4-16.2); 8 patients prematurely ended the study (6 due to adverse events). The most common grade 3-4 toxicities were hand-foot syndrome and asthenia which occurred in 20.5% and 15.9% of patients.
Discussion
Pancreatic neuroendocrine tumors are rising in incidence and represent a growing proportion of pancreatic tumors. Most NETs are unresectable at diagnosis or progress after local treatment and in this setting there have been relatively few treatment options. Recently, two new targeted agents have been approved for this setting. Everolimus is an mTOR inhibitor which inhibits cell growth, proliferation, and angiogenesis, and has been shown to prolong progression free survival compared to placebo. Sunitinib is a multi-kinase inhibitor that is thought to have an effect in NET through inhibition of VEGF which plays a role in angiogenesis in NET [18]. Much needs to be discovered about the appropriate role of these new agents including identifying appropriate candidates for therapy and safety profiles of these medications in this new indication; and there were several important abstracts addressing these questions at the ASCO Annual Meeting in 2011. In Abstract #4010 [12], Shah et al. demonstrated that everolimus is beneficial despite the prior or concurrent use of long acting somatostatin analogs. Octreotide (in long acting depot administration) has been shown to prolong time to progression in a subset of NETs [19] and this data suggests that the benefit of everolimus is independent of octreotide use. In Abstract #4103 [13], Pommier et al. reported that there was benefit to everolimus compared to placebo in patients regardless of whether they had prior chemotherapy. Updated safety data of everolimus in RADIANT-3 was reported in Abstract #4009 [14]; Strosberg et al. found that everolimus was associated with frequent adverse events but few grade 3 or 4 toxicities (5-6%). In Abstract #4008 [15], Raymond et al. reported updated survival data for sunitinib. They found that with additional follow up median overall survival was not prolonged by a statistically significant margin, the progression free survival benefit was preserved. Patients on this trial were allowed to switch therapy at progression and this may explain to lack of survival benefit seen to date. Two novel agents were also reported, in phase I data (Abstract #4120) [16], a novel somatostatin analog, pasireotide, was found to be safe when administered with everolimus. In phase II data (Abstract #4113) [17], the combination of sorafenib and bevacizumab for dual anti-angiogenesis blockade was associated with clinical benefit with increased toxicity.
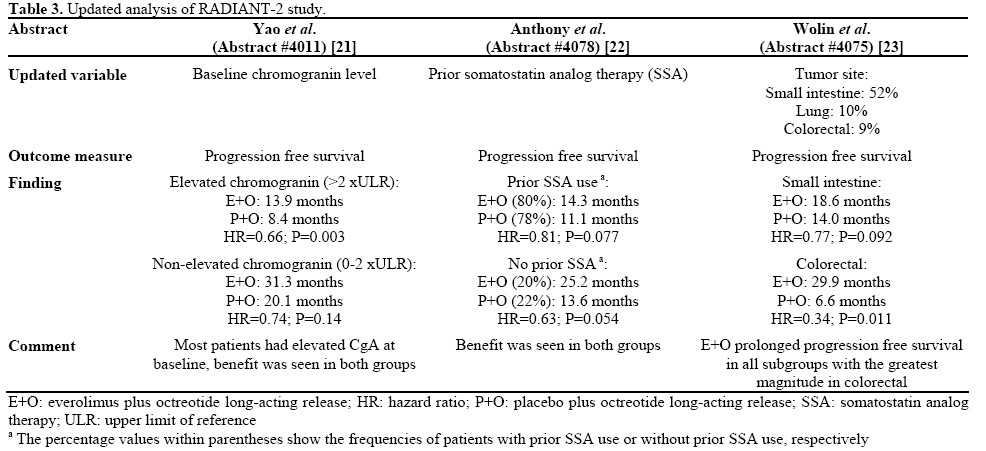
Finally, updated data was also presented from the RADIANT-2 clinical trial which looked at the role of adding everolimus or placebo to treatment with longacting release (LAR) octreotide in patients with advanced NETs with carcinoid syndromes (Table 3). This study included 429 patients, a small number had primary pancreatic site, and it demonstrated improvement in median progression free survival from 11.3 to 16.4 months with the addition of everolimus. Though the trial demonstrated that everolimus is associated with a reduced risk of progression of 23%, the hazard ratio (HR: 0.77; P=0.026) fell just short of the prespecified boundary of statistical significance [20]. Exploratory data from the RADIANT-2 trial are summarized in Table 3.
Conclusions
In summary, everolimus demonstrates improvement in progression free survival in advanced pNET independent of prior chemotherapy or somatostatin analog use and is generally well tolerated. Sunitinib demonstrated benefit in progression free survival compared to placebo in pNET and a phase II trial of combination anti-angiogenic therapy showed some efficacy with increased toxicity. Together these reports suggest that patients with pNET will continue to benefit from novel therapy.
Conflict of interest
The authors have no potential conflicts of interest
References
- Yao JC, Eisner MP, Leary C, et al. Population-based study ofislet cell carcinoma. Ann Surg Oncol 2007;14:3492-3500.
- Zhou J, Enewold L, Stojadinovic A, et al. Incidence rates ofexocrine and endocrine pancreatic cancers in the United States. Cancer Causes Control 2010;21:853-861.
- Yao JC, Hassan M, Phan A, et al. One hundred years after"carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008; 26:3063-72.
- Moertel CG, Hanley JA, Johnson LA. Streptozocin alone compared with streptozocin plus fluorouracil in the treatment of advanced islet-cell carcinoma. N Engl J Med 1980;303:1189-1194.
- Moertel CG, Lefkopoulo M, Lipsitz S, Hahn RG, Klaassen D. Streptozocin-doxorubicin, streptozocin-fluorouracil, or chlorozotocinin the treatment of advanced islet-cell carcinoma. N Engl J Med1992; 326:519-523.
- McCollum AD, Kulke MH, Ryan DP, et al. Lack of efficacy of streptozocin and doxorubicin in patients with advanced pancreatic endocrine tumors. Am J Clin Oncol 2004;27:485-488
- Metz DC, Jensen RT. Gastrointestinal neuroendocrine tumors: pancreatic endocrine tumors. Gastroenterology 2008;135:1469-1492
- Hauso O, Gustafsson BI, Kidd M, et al. Neuroendocrine tumor epidemiology: contrasting Norway and North America. Cancer 2008;113:2655-2664
- Shah MH, Ito T, Lombard-Bohas C, Wolin EM, Van Cutsem E,Sachs C, et al. Everolimus in patients with advanced pancreatic neuroendocrine tumors: Updated results of a randomized, doubleblind, placebo-controlled multicenter phase III trial (RADIANT-3). J Clin Oncol 2011, 29(Suppl. 4):158.
- Yao JC, Shah MH, Ito T, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med 2011; 364:514-23.
- Raymond E, Dahan L, Raoul J-L, et al. Sunitinib malate for thetreatment of pancreatic neuroendocrine tumors. N Engl J Med 2011;364:501-13.
- Shah MH, Lombard-Bohas C, Ito T, et al. Everolimus in patients with advanced pancreatic neuroendocrine tumors (pNET): Impact of somatostatin analog use on progression-free survival in the RADIANT-3 trial. J Clin Oncol 2011; 29(Suppl.):4010.
- Pommier RF, Wolin EM, Panneer selvam A, et al. Impact ofprior chemotherapy on progression-free survival in patients (pts) with advanced pancreatic neuroendocrine tumors (pNET): Results from the RADIANT-3 trial. J Clin Oncol 2011; 29(Suppl.):4103.
- Strosberg JR, Lincy J, Winkler RE, et al. Everolimus in patients with advanced pancreatic neuroendocrine tumors (pNET): Updated results of a randomized, double-blind, placebo-controlled, multicenter, phase III trial (RADIANT-3). J Clin Oncol 2011;29(Suppl.):4009.
- Raymond E, Niccoli P, Raoul J, et al. Updated overall survival (OS) and progression-free survival (PFS) by blinded independent central review (BICR) of sunitinib (SU) versus placebo (PBO) for patients (Pts) with advanced unresectable pancreatic neuroendocrinetumors (NET). J Clin Oncol 2011; 29(Suppl.):4008.
- Chan JA, Ryan DP, Fuchs CS, et al. Updated results of a phase Istudy of pasireotide (SOM230) in combination with everolimus (RAD001) in patients (pts) with advanced neuroendocrine tumors (NET). J Clin Oncol 2011; 29(Suppl.):4120.
- Castellano DE, Capdevila J, Salazar R, et al. Sorafenib and bevacizumab combination targeted therapy in advanced neuroendocrine tumor: A phase II study of the Spanish Neuroendocrine Tumor Group (GETNE0801). J Clin Oncol 2011;29(Suppl.):4113.
- Casanovas O, Hicklin DJ, Bergers G, Hanahan D. Drug resistance by evasion of antiangiogenic targeting of VEGF signalingin late-stage pancreatic islet tumors. Cancer Cell 2005;8:299-309
- Rinke A, Muller HH, Schade-Brittinger C, et al. Placebo controlled, double-blind, prospective, randomized study on the effectof octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol 2009; 27:4656-63.
- Pavel M, Hainsworth JD, Baudin E, et al. A Randomized, Double-blind, placebo-controlled, multicenter Phase III trial of everolimus + octreotide LAR vs placebo + octreotide LAR inpatients with advanced neuroendocrine tumors (NET) (RADIANT-2). Ann Oncol 2010; 21(Supplement 8): viii1-12.
- Yao JC, Ricci S, Winkler RE et al. Everolimus plus octreotide LAR versus placebo plus octreotide LAR in patients with advanced neuroendocrine tumors (NET): Updated safety and efficacy results from RADIANT-2. J Clin Oncol 2011; 29(Suppl.):4011.
- Anthony LB, Peeters M, Hainsworth JD et al. Everolimus plusoctreotide LAR versus placebo plus octreotide LAR in patients with advanced neuroendocrine tumors (NET): Effect of prior somatostatin analog therapy on progression-free survival in the RADIANT-2 trial.J Clin Oncol 2011; 29(Suppl.):4078.
- Wolin EM, Fazio N, Saletan S et al. Everolimus plus octreotide LAR versus placebo plus octreotide LAR in patients with advanced neuroendocrine tumors: Analysis by primary tumor site from RADIANT-2. J Clin Oncol 2011; 29(Suppl.):4075.

