Keywords
Mortality; Obesity; Pancreatitis
INTRODUCTION
Early diagnosis and accurate prediction of acute
pancreatitis (AP) severity is basic. Although most patients
with AP run a benign course, up to 20% develop severe
complications resulting in high mortality, ranging from
14 to 25% [1]. The severity of AP is a continuum from
a mild, self-limiting pancreatic inflammation to severe
disease with local and systemic complications. Identifying
patients who are likely to present a complicated course
helps the physician selecting those patients who will
benefit from close monitoring and surveillance. To date,
several objective and inexpensive multiple-choice score
systems (APCAHE II, Ranson, Glasgow…) have been
studied, neither one completely satisfactory. Obesity
has been used as a covariate within a multiple clinical score [2] and has been linked to respiratory failure,
local and systemic complications and death in patients
with AP [3, 4, 5].
The prevalence of obesity has grown over the past
two decades in most occidental countries and it is a
well-recognized risk factor for cardiovascular diseases
and mortality in general population [6, 7, 8]. However,
during the past decade, there is emerging evidence that
some obese patients with chronic diseases and acute
decompensations, such as congestive heart failure in
subjects with chronic heart failure [9, 10] or exacerbation
of chronic obstructive pulmonary disease [11] may
present lower mortality or readmissions compared
with normal-weight patients. In addition, it has been
reported that obese subjects might fare better after some
surgical procedures, namely non-bariatric surgery [12],
coronary artery bypass surgery [13] and decompressive
laparotomy in patients with AP requiring Intensive Care
Unit admission [14]. Such obese relationship has been
termed as a phenomenon of obesity paradox and has
never been stated among patients with AP. To address
this question in patients with AP, we conducted a study
to assess the relationship between overweight and
obesity and in-hospital mortality.
The aim of this study was to examine the association
between obese individuals and all-cause in-hospital
mortality among patients with AP.
PATIENTS AND METHODS
A retrospective chart review of consecutive patients
with AP as the primary reason for discharge was performed.
We identified every patient discharged from an Internal
Medicine Department from hospitals in the Spanish Public
Health Service (SPHS) between January 1st, 2005 and
December 31st, 2013. Patients with AP and a diagnosis of
obesity in the hospital discharge medical report were then
identified. The in-hospital mortality in obese patients with
AP was compared with their normal-weight counterparts
to assess the effect of obesity on the final outcome.
Hospital discharge data were obtained from the Basic
Minimum Data Set (BMDS) which is a compulsory registry
for each patient admitted to a hospital in the SPHS, a system
that cares for more than 90% of the country’s population.
All centers are requested to submit this information to the
Spanish Health Ministry. BMDS contains sociodemographic
and clinical data for every hospital discharge, including:
gender and age, primary and secondary diagnoses
according to the International Classification of Diseases,
Ninth Revision, Clinical Modification (ICD-9-CM) code,
primary and secondary procedures, admission and discharge
status, inpatient stay from the time of admission to discharge
and hospital characteristics (less than 200 beds; 200 to 500
beds; 500 to 1,000 beds; more than 1,000 beds).
Patients were selected if they were discharged with the
diagnosis of pancreatitis (ICD-9-CM: 577.0). The patients
above selected who also had a secondary diagnosis of
obesity (ICD-9-CM: DRG 278.00. 278.01) were analyzed.
Definitions
Complications: The grading of the severity in AP has
undergone significant recent changes [15, 16]. In the
present study, disease severity was stratified as described
in the Atlanta classification [17] because it reflects the
criteria used in the medical reports and discharge files
during the period of the study. Severe AP was defined by
the presence of local complications (fluid collections or
pancreatic necrosis) and/or organ failure, including shock,
renal o respiratory failure or digestive hemorrhage. In our
study, other conditions linked to a poor outcome were also
considered as complications during admission.
In order to describe the complications above mentioned,
we identified the following ICD-9-MC codes present in any
secondary diagnosis field in the discharge medical reports:
acute respiratory failure (ICD-9-CM: 518.82-518.84), acute
renal failure (ICD-9-CM: 403.11, 403.91,404.12, 585-586),
pneumonia (ICD-9-CM:480-486; 003.22, 507.0,510.0,
510.9, 513.0), bronchoaspiration (ICD-9-CM: 507.0),
hypoglycemia (ICD-9-CM: 251.0-2, 250.30-1, 250.80-1,
249.80-1), decubitus ulcer (ICD-9-CM: 707.xx), urinary
tract infection (ICD-9-CM: 599.00, 590.xx, 646.60-49, 601),
deep venous thrombosis (ICD-9-CM: 415.1, 415.11, 415.19, 451.2, 451.81, 451.9, 453.40, 453.41, 453.42, 453.8, 453.9),
sepsis (ICD-9-CM: 531-536, 537.83, 530.2, 530.82) 038.
xx, 995.91, 995.92), gastrointestinal bleeding (ICD-9-MC:
530.21, 530.82, 531-535.00, 531-535.01, 531-535.20, 531-
535.21, 531-535.40, 531-535.41, 531-535.60, 531-535.61),
shock (ICD-9-CM: 785.50-59) and malnutrition (ICD-9-CM:
260-263.9). The presence or absence of complications has
been shown in three different ways. Firstly, an item named
“Any complication” which describes the presence of any of
the complications mentioned above. Secondly, a composite
variable named “Atlanta”, which includes any complication
linked to severe AP according to 1992 Atlanta consensus,
and finally, each one of the different complications in a
separate display.
Comorbidity: The Charlson Co-morbidity Index (CCI)
[18] was computed for each patient. This index illustrates
the number and relevance of co-morbid diseases according
to ICD categories. It has been used in the present study to
adequately depict the presence of additional co-occurring
disorders, and thus appropriately adjust the results for
the presence of diseases coexisting with AP and obesity
that may affect mortality. The Charlson comorbidity index
predicts the ten-year mortality for a patient who may
have a range of comorbid conditions. Each condition is
assigned a score of 1, 2, 3, or 6, depending on the risk of
dying associated with each one. Results provide a total
score ranging between 0-37 to predict mortality. A grade
higher than 2 is related to a mortality rate greater than
50% per year. Clinical conditions and associated scores
are as follows:
1 each: Myocardial infarction, congestive heart failure,
peripheral vascular disease, dementia, cerebrovascular
disease, chronic lung disease, connective tissue disease,
ulcer, chronic liver disease, diabetes.
2 each: Hemiplegia, moderate or severe kidney disease,
diabetes with end organ damage, tumor, leukemia,
lymphoma.
3 each: Moderate or severe liver disease.
6 each: Malignant tumor, metastasis, AIDS.
In addition, the following risk factors were identified
using ICD-9-MC codes in any primary or secondary
diagnosis field: diabetes (ICD-9-CM: 250.00-250.99),
alcohol abuse (ICD-9-MC 305.00-305.03) and gallstones
(ICD-9-CM: 575.xx).
Hospital Stay: Mean hospital stay was defined as the
number of days that each patient spent at the medical
center.
In-Hospital Mortality: Patients who died during
admission were recorded. Deaths that might have occurred
after patient´s discharge were not measured as these data
were not available for the investigators.
Statistical Methods
A descriptive analysis was carried out in patients with
AP. The demographic variables among patients with or without obesity were compared. We used the chi-square
test for categorical variables with the Yates correction, the
Fisher`s exact test for dichotomous variables when the
expected value of a cell was less than 5, and Student´s t-test
or ANOVA for quantitative variables. All the univariate
analyses were accomplished after having adjusted for age
and gender. The Odds-Ratios (OR) and 95% Confidence
Intervals (CI) were estimated from the regression
coefficients.
A multivariate logistic regression analysis was
performed in order to determine the excess of mortality
owing to obesity, after the correction of possible
confounding variables such as the age of the patient (in
years, as a continuous variable), Charlson index (in points,
as a continuous variable), sex and all variables that had
demonstrated a statistically significant relationship in the
univariate analysis with mortality (alcohol, gallstones,
diabetes, acute respiratory failure, and acute renal failure).
A logistic regression analysis with backward stepwise
procedure and p>0.10 as the criterion for exclusion was
used to find the best predictive model. Stratified analyses
were performed to examine confounders and interactions.
All statistical analyses were carried out with the Statistical
Package for the Social Sciences (SPSS, version 16, Chicago,
Illinois, SPSS Inc).
RESULTS
Within the study period, 55285 episodes of AP were
included in the analysis. The average age was 64.1 years
(SD 18.87 18-108); 56.3% of the patients were men. The
median hospital stay was 10.9 days (SD, 12.72; range
0-849). A CCI ≥ 2 was present in 18.0% of the cases.
Overall, a total of 4594 (8.3%) subjects were obese. During
admission 2844 (5.1%) patients died, 4478 (8.1%) were
readmitted at least once within 30 days of the index date
of admission with the same Major Diagnostic Category
as the main diagnosis, and a high proportion of patients
developed complications 10339 (18,7%). Overall, 27% of
patients were admitted in small size centers (<200 beds),
40% in medium size (200-500), 18.5% in big size (500-
1000) and 14.5% in hospitals with more than 1000 beds.
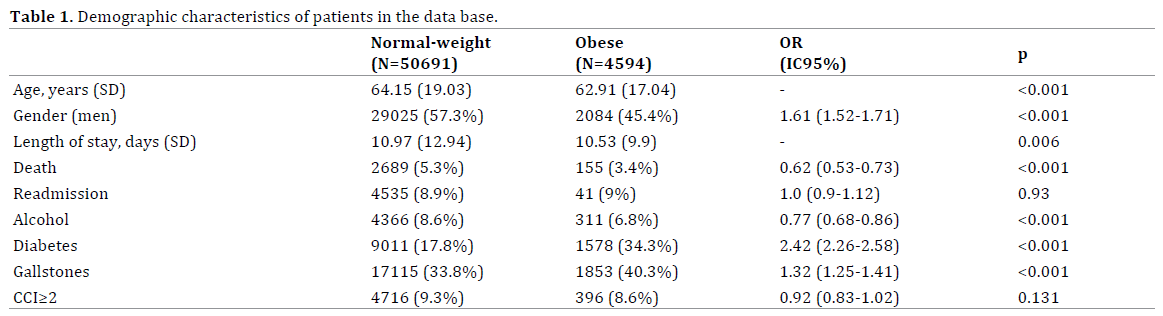
Obese patients were more frequently women (54.6%
vs. 42.7%; P <0.001), younger (62.9 vs. 64.1 years; p<0.001)
and there was a less proportion of alcoholic intake (6.8%
vs. 8.6%; P <0.001) than in non-obese patients. Diabetes and gallstones were more frequently found in obese
patients than in non-obese (34.3% vs. 17.8% and 40.3% vs.
33.8% respectively, P<0.001). CCI was higher in non-obese
patients (2.4 vs. 1.7; P <0.001). The mortality among obese
patients was 3.4% versus 5.3% in non-obese patients, the
unadjusted mortality rate was 0.62 IC 95% 0.53-0.573
(Table 1).
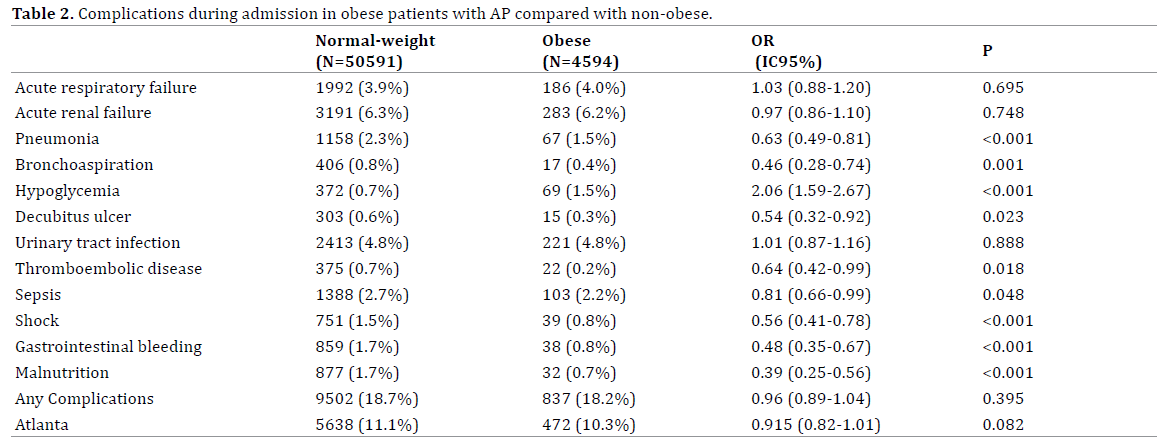
Obese patients presented more hypoglycemia (1.5%
vs. 0.7% p<0.001) than non-obese during admission.
Bronchoaspiration (0.8% vs. 0.4%; P <0.001), pneumonia
(2.3% vs. 1.5%; P <0.001), decubitus ulcer (0.6% vs. 0.3%; P =0.02), sepsis (2.7% vs. 2.2%; P=0.04), shock (1.5% vs.
0.8%; P <0.001), malnutrition (1.7% vs. 0.7%; P <0.007) or
thrombosis (0.7% vs. 0.2%; P=0.04) were less frequent in
obese patients than in non-obese subjects (Table 2). The
total rate of complications was slightly superior in nonobese
patients than in obese patients (18.7% vs. 18.2%;
OR 1.03 IC95% 0.96-1.10; P =0.395), but there were no
statistical differences. Similarly, the presence of severe
AP was slightly superior in non-obese patients than in
obese (11.17% vs. 10.3%; OR 0.915 IC 95% 0.829-1.010,
p= 0.082), but there were no statistical differences.
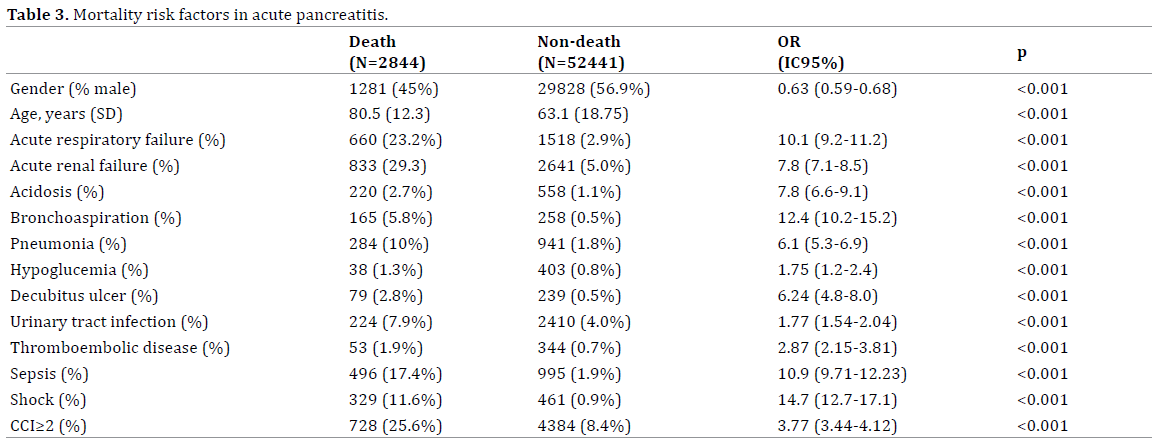
The following complications were significantly
associated with higher risk of mortality in the univariate
analysis in all patients with AP: acute renal failure, acute
respiratory failure, acidosis, bronchoaspiration, pneumonia,
hypoglycemia, decubitus ulcer, urinary tract infection, deep
venous thrombosis, sepsis or shock (Table 3).
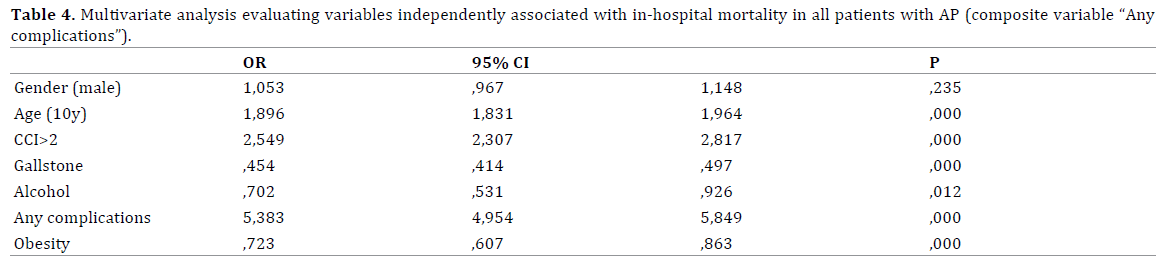
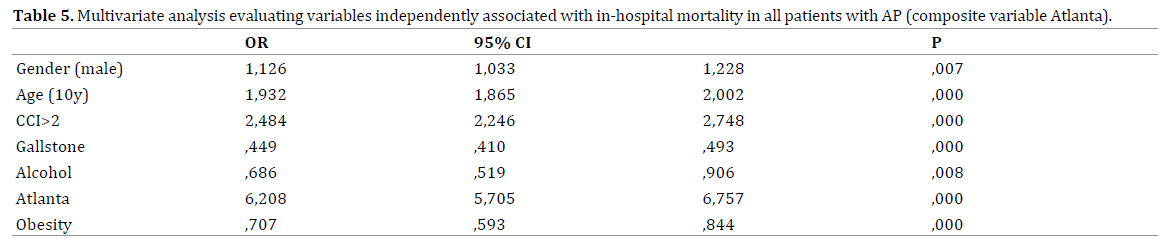
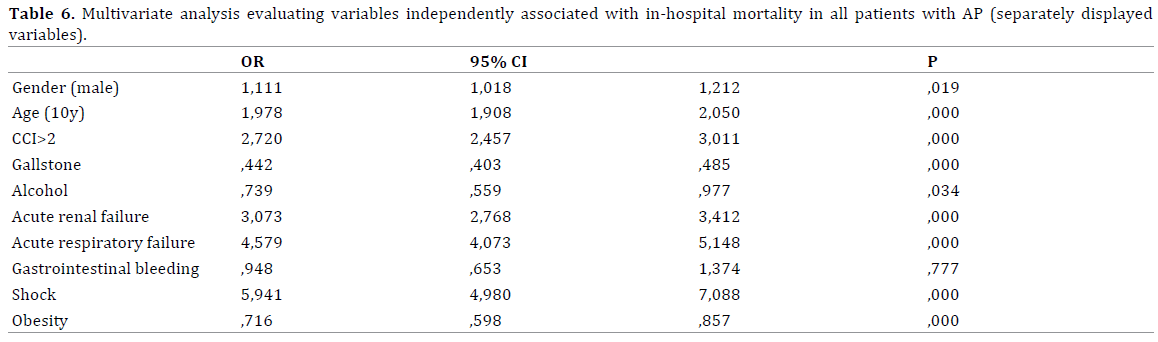
Multivariate logistic regression analysis was performed
to further assess which variables were independently
associated with a higher mortality risk during hospital
stay in all patients with AP). Age, gender (male), CCI≥ 2 and
the presence of “All complications” and Atlanta composite
variable were independent predictive factors of mortality
in patients with AP (Table 4 and 5). Obesity was found to
have a lower mortality risk (OR 0.72 IC 95% 0.61-0.86).
Acute renal and respiratory failure as well as the presence
of shock correlate with in-hospital mortality (Table 6).
DISCUSSION
Our data from a large series of medical records of
patients admitted with AP reveal that there is an inverse
relationship between obesity and mortality. The results
from the analysis of 55285 charts show that obesity is
an independent prognostic factor for lower in-hospital mortality in subjects with AP and that this association
remains significant when controlled for confounding
factors. The mechanisms that might account for lower risk
of death in obese patients affected by AP remain unknown.
The fact that patients may be beneficially affected by obesity is known as “obesity paradox” or “reverse epidemiology”.
Some authors claim that obese patients may have a more
aggressive medical treatment and a closer surveillance
than normal-weight groups. Also, it has been suggested
that some obese patients may be on more cardioprotective medical therapy than other groups. These factors may lead
to the false impression that obesity has a protective effect
in some clinical conditions.
As for the physiologic mechanisms that may account for
the obesity paradox, most of them are merely conjectures.
Biochemical changes in obese patients may partly
explain this benefit. A greater mobilization of endothelial
progenitor cells has been found in obese patients with less
coronary atherosclerosis [19]. Cardiovascular protection
of obese patients may also be mediated by a decreased
production of thromboxane [20]. Also, among subjects with
heart failure, obese patients exhibit lower concentration of
tumor necrosis factor receptor and this may cause a better
outcome [21].
Controversies remain as to whether the obesity
paradox is related to age. Most of the studies that confirm
the obesity paradox have recruited cohorts of elderly
subjects. It has been demonstrated that accumulation of
intra-abdominal fat is significantly greater at younger ages
compared with older ages, regardless of sex and race [22].
Thus, if visceral adiposity decreases with age, then higher
BMI due to peripheral fat stores may be responsible for the
observed protective effect of obesity in elderly patients. In
the present analysis, no waist circumference measures
have been registered and therefore no information can
be obtained regarding fat distribution. However, obese
subjects were significantly younger than those non-obese,
62.9 vs. 64.1 years respectively. Thus, the obesity paradox
in our cohort does not seem to be related to changes
in adiposity distribution linked to aged individuals.
Furthermore, the reduction of mortality in obese patients
with AP persisted after multivariate adjustment, including
age.
Literature review shows that there are no studies to
directly examine the paradoxal obesity in patients with AP.
The results of this analysis apparently contradict current
wisdom on obesity as a risk factor for severity in AP. Earlier
work suggests obesity as a risk factor for severe AP [2, 3, 4, 5]. Two meta-analysis have examined the association
between BMI and AP prognosis [23, 24]: compared with
normal weight individuals, obese patients (BMI > 30 kg/
m2) developed significantly more severe AP and had a
significantly increased risk of death. However, the rates
of obesity in the studies were significantly heterogeneous, varying from 8% to 57%, and, as is usually the case in any
meta-analysis, there were wide methodological variations.
In addition, the possibility of publication bias is of concern.
Conversely, in another systematic review, obesity was not
found to be an independent prognostic factor for mortality
and organ failure in patients with AP [25].
In two prospective reports, several parameters were
investigated in patients suffering from AP to assess its
prognostic role. Thandassery et al. [26] found that dynamic
multiple organ failure over the first week (measured
by multiple organ failure scoring system MOFS), higher
APACHE II score and infected necrosis were independent
predictors of mortality. Similarly, Gloor et al. [27] reported
that the only parameter that proved to be an independent
risk factor for death among patients with AP was infection
of pancreatic necrosis. In both studies, univariate analysis
revealed that BMI was a negative risk factor. However, after
multivariate analyses with a stepwise forward regression,
obesity did not prove to be an independent risk factor for
death.
In our analysis, advanced age has shown to be a risk
factor for higher mortality. In many but not all reports
[28], older age has correlated with a more severe prognosis
[29]. Some authors state that older individuals have a poor
outcome because of comorbid disease rather than old age
itself [30]. We have separately analyzed the influence of
age and comorbidity in the evolution of AP and logistic
regression failed to show significant association. Thus,
in agreement with previous literature [31], we conclude
that, in this cohort, advanced age worsens prognosis
irrespective the comorbid diseases. Unfavorable outcome
in older individuals could be put down to the diminished
physiological response typical of elderly patients.
As for the outcome of AP according to the main causes,
to date, the influence of etiology on the severity of AP has
not been clearly stablished and the results differ depending
on the various studies reviewed. Some authors emphasize
that etiology is not linked to poor outcome in AP [31, 32].
On the contrary, previous studies confirm a more severe
presentation in alcoholic AP [33], while others claim that
biliary AP correlates with worse prognosis [34]. In our
study, both etiologies were significantly associated to
lower in-hospital mortality. This finding could probably
be linked to current improvements in antibiotic therapy, endoscopic retrograde biliary drainage followed by
endoscopic sphincterotomy and specific care in critical
units. It seems to be accepted that once the pathogenic
mechanism has initiated the disease, the course of AP is no
longer linked the initial cause.
As previously accepted [1], the rate of in-hospital
mortality in our analysis was higher in patients with
Atlanta complications. When examined separately, acute
renal and respiratory failure as well as the presence of
shock, correlates with in-hospital mortality. However,
digestive hemorrhage was not an independent prognostic
factor of mortality probably due to the reduced number of
patients presenting this complication.
The strengths of our study include the large nationwide
population (more than 55000 patients) allowing
statistically precise estimates of the relationship between
obesity and mortality in patients with AP. Compared with
previous studies this is a large population-based analysis
with much greater numbers of patients and thus adequately
powered to detect differences between both groups.
There are however certain caveats that may affect the
results of this report. Firstly, the main limitation of our
analyses is that it is a retrospective study of the Basic
Minimum Data Set (BMDS) administrative database and
therefore subject to information bias. This database is
applied nationwide and allows clustering of patients in
medical codes that describe procedures and assistance
in hospital inpatients. Medical indexing International
Classification of Diseases, Ninth Revision, Clinical
Modification (CIE-9-CM) and Diagnosis Related Group
(GRD) obtained from BMDS were initially intended to
define different categories that were clinically similar
and expected to use the same level of hospital resources,
therefore medical codes can sometimes be inaccurate
concerning severity in some clinical conditions. However,
this classification system has long been accepted and used
throughout many different countries in our environment.
We fully agree on the accuracy of these data and we
retrospectively focused on the information displayed in
the database.
We have not adjusted for edematous or necrotizing
pancreatitis, thus, weather there are many more obese
patients with edematous pancreatitis cannot be rule out.
The ICD-9-CM code describes three different groups of
patients with pancreatitis, namely, acute (577.0), chronic
(577.1) and mumps pancreatitis (072.3). ICD-9-CM code
577.0 applies to abscess of pancreas, necrosis (sterile
or infected) of pancreas, edematous, hemorrhagic and
suppurate pancreatitis. Based on ICD-9-CM 577.0, a
"grouper" program assigns a DRG 204 to all patients with
acute pancreatitis, irrespective of the presence of necrosis.
Both 577.0 medical code and DRG 204 can thus indicate
a wide range of severity within patients admitted with
acute pancreatitis. Being aware of the possible limitations
of the DRG classification system to account adequately
for severity of acute pancreatitis, we included ICD-9-CM
medical codes describing complications related to acute pancreatitis according to Atlanta classification system as
well as other medical complications not included in Atlanta
criteria. We believe that such conditions can provide a more
accurate spectrum of severity and sometimes indirectly
reflect a possible underlying pancreatic necrosis, left
underdiagnosed otherwise by means of ICD-9-CM codes.
There has only been limited evaluation on how
frequently obesity is captured in administrative databases
or how accurately is captured. A recent study by Martin et
al. to assess the validity of obesity coding in administrative
database [35], confirmed that obesity was poorly coded,
however, when coded it was coded accurately.
Previous studies show that the relationship between
mortality and obesity in patients with AP is not linear.
Patients who are overweight and moderately obese have
lower mortality risk than those with either normal or
low BMI and those who are morbidly obese [36]. This is
consistent with the “U” shaped curve concept that may
explain the obesity paradox. No categories of BMI have
been registered in our study, thus no conclusions can be
dropped as whether different BMI ranges are protective
from mortality in AP while others might be associated with
worse outcome.
Finally, it should be emphasized the fact that BMI
does not discriminate centrally distributed adiposity in
upper body from lower-body obesity, the former being
associated with poor outcome. A recent cohort study
using dual-energy x-ray absorptiometry (DEXA) scans to
estimate percent body fat reveals that higher BMI is not
associated with high body-fat percentage, which might
help explain the obesity paradox observed in some studies
[37]. Neither waist circumferences measures nor percent
body fat have been recorded in the present study.
It is well known that obesity is related to an overall
decrease in lifetime survival and it is an increasingly major
hazard in many developing countries. The discussion of
the existence of the obesity paradox cannot lead to the
underestimation for obesity as a crucial risk factor for
the development of some cardiovascular and metabolic
diseases, which requires appropriate prevention and
specific management strategies. The results of the present
study cannot be extrapolated to the general population.
However, in certain clinical settings, obesity could confer
survival advantage over non-obese individuals after all
confounding factors are assessed.
CONCLUSION
This study highlights the need for further prospective
studies to be undertaken to determine the potential
contribution of obesity as a protective factor in patients
with AP.
Contribution Statement
RB designs the study and made statistical analysis; AG
wrote the article; JM and SP were the reviewers; AZ and
JC made the data interpretation and de final revision; MY
made the statistical analysis with RB
Acknowledgments
The authors thank the Spanish Minister or Hearth for
the permission to use of the data.
Conflict of Interest
There is no potential source of financial or relationship
conflict of interest.
References
- Banks PA, Freeman ML, Practice Parameters Committee of the
American College of Gastroenterology. Practice guidelines in acute
pancreatitis. Am J Gastroenterol 2006; 101:2379-400. [PMID: 17032204]
- Johnson CD, Toh SK, Campbell MJ. Combination of APACHE-II score
and an obesity score (APACHE-O) for the prediction of severe acute
pancreatitis. Pancreatology 2004; 4:1-6. [PMID: 14988652]
- Suazo-Baráhona J, Carmona-Sánchez R, Robles-Díaz G, Milke-García
P, Vargas-Vorácková F, Uscanga-Domínguez L, et al. Obesity: a risk factor
for severe acute biliary and alcoholic pancreatitis. Am J Gastroenterol
1998; 93:1324-8. [PMID: 9707059]
- Mentula P, Kylänpää ML, Kemppainen E, Puolakkainen P. Obesity
correlates with early hyperglycemia in patients with acute pancreatitis
who developed organ failure. Pancreas 2008; 36:e21-5. [PMID: 18192869]
- Sempere L, Martinez J, de Madaria E, Lozano B, Sanchez-Paya J,
Jover R, et al. Obesity and fat distribution imply a greater systemic
inflammatory response and a worse prognosis in acute pancreatitis.
Pancreatology 2008; 8:257-64. [PMID: 18497538]
- Hall JE. The kidney, hypertension, and obesity. Hypertension 2003;
41:625-33. [PMID: 12623970]
- Roberts DL, Dive C, Renehan AG. Biological mechanisms linking
obesity and cancer risk: new perspectives. Annu Rev Med 2010; 61:301-
16. [PMID: 19824817]
- Adams KF, Schatzkin A, Harris TB, Kipnis V, Mouw T, Ballard-Barbash
R, et al. Overweight, obesity, and mortality in a large prospective cohort
of persons 50 to 71 years old. N Engl J Med 2006; 355:763-78. [PMID:
16926275]
- Curtis JP, Selter JG, Wang Y, Rathore SS, Jovin IS, Jadbabaie F, et al. The
obesity paradox: body mass index and outcomes in patients with heart
failure. Arch Intern Med 2005; 165:55-61. [PMID: 15642875]
- Zapatero A, Barba R, Gonzalez N, et al. Influence of obesity and
malnutrition on acute heart failure. Rev Esp Cardiol (Engl Ed) 2012;
65:421-6. [PMID: 22133785]
- Zapatero A, Barba R, Ruiz J, et al. Malnutrition and obesity: influence
in mortality and readmissions in chronic obstructive pulmonary disease
patients. J Hum Nutr Diet 2013; 26 Suppl 1:16-22. [PMID: 23656492]
- Mullen JT, Moorman DW, Davenport DL. The obesity paradox: body
mass index and outcomes in patients undergoing nonbariatric general
surgery. Ann Surg 2009; 250:166-72. [PMID: 19561456]
- Hastie CE, Padmanabhan S, Slack R, Pell AC, Oldroyd KG, Flapan AD, et
al. Obesity paradox in a cohort of 4880 consecutive patients undergoing
percutaneous coronary intervention. Eur Heart J 2010; 31:222-6.
[PMID: 19687163]
- Davis PJ, Eltawil KM, Abu-Wasel B, Walsh MJ, Topp T, Molinari M, et
al. Effect of obesity and decompressive laparotomy on mortality in acute
pancreatitis requiring intensive care unit admission. World J Surg 2013;
37:318-32. [PMID: 23052814]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG,
et al. Classification of acute pancreatitis--2012: revision of the Atlanta
classification and definitions by international consensus. Gut 2013;
62:102-11. [PMID: 23100216]
- Dellinger EP, Forsmark CE, Layer P, Lévy P, Maraví-Poma E, Petrov
MS, et al. Determinant-based classification of acute pancreatitis severity:
an international multidisciplinary consultation. Ann Surg 2012; 256:875-
80. [PMID: 22735715]
- Bradley EL. A clinically based classification system for acute
pancreatitis. Summary of the International Symposium on Acute
Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg
1993; 128:586-90. [PMID: 8489394]
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of
classifying prognostic comorbidity in longitudinal studies: development
and validation. J Chronic Dis 1987; 40:373-83. [PMID: 3558716]
- Fadini GP, Boscaro E, de Kreutzenberg S, Agostini C, Seeger F,
Dimmeler S, et al. Time course and mechanisms of circulating progenitor
cell reduction in the natural history of type 2 diabetes. Diabetes Care
2010; 33:1097-102. [PMID: 20150295]
- Graziani F, Biasucci LM, Cialdella P, Liuzzo G, Giubilato S, Della Bona
R, et al. Thromboxane production in morbidly obese subjects. Am J
Cardiol 2011; 107:1656-61. [PMID: 21439532]
- Feldman AM, Combes A, Wagner D, Kadakomi T, Kubota T, Li YY, et al.
The role of tumor necrosis factor in the pathophysiology of heart failure.
J Am Coll Cardiol 2000; 35:537-44. [PMID: 10716453]
- Lee CG, Fujimoto WY, Brunzell JD, Kahn SE, McNeely MJ, Leonetti
DL, et al. Intra-abdominal fat accumulation is greatest at younger ages
in Japanese-American adults. Diabetes Res Clin Pract 2010; 89:58-64.
[PMID: 20392506]
- Hong S, Qiwen B, Ying J, Wei A, Chaoyang T. Body mass index and
the risk and prognosis of acute pancreatitis: a meta-analysis. Eur J
Gastroenterol Hepatol 2011; 23:1136-43. [PMID: 21904207]
- Martinez J, Jonhson CD, Sanchez-Paya J, de Madaria E, Robles-Díaz G,
Pérez-Mateo M. Obestiy is a definitive risk factor of severity and mortality
in acute pancreatitis: an updated Meta-analysis. Pancreatology 2006; 6:
206-9. [PMID: 16549939]
- Premkumar R, Phillips AR, Petrov MS, Windsor JA. The clinical
relevance of obesity in acute pancreatitis: targeted systematic reviews
Pancreatology 2015; 15:25-33. [PMID: 25464938]
- Thandassery RB, Yadav TD, Dutta U, Appasani S, Singh K, Kochhar R.
Dynamic nature of organ failure in severe acute pancreatitis: the impact
of persistent and deteriorating organ failure. HPB (Oxford) 2013; 15:523-
8. [PMID: 23750495]
- Gloor B, Müller CA, Worni M, Martignoni ME, Uhl W, Büchler MW.
Late mortality in patients with severe acute pancreatitis. Br J Surg 2001;
88:975-9. [PMID: 11442530]
- Kaya E, Dervisoglu A, Polat C. Evaluation of diagnostic findings and
scoring systems in outcome prediction in acute pancreatitis. World J
Gastroenterol 2007; 13:3090–4. [PMID: 17589925]
- Company L, Saez J, Martinez J, Aparicio JR, Laveda R, Griñó P, et al.
Factors predicting mortality in severe acute pancreatitis. Pancreatology
2003; 3:144–8. [PMID: 12748423]
- Blum T, Maisonneuve P, Lowenfels AB, Lankisch PG. Fatal outcome
in acute pancreatitis: its occurrence and early prediction. Pancreatology
2001; 1:237–41. [PMID: 12120201]
- Gonzálvez-Gasch A, García de Casasola G, Barba Martín R, et al. A
simple prognostic score for risk assessment in patients with acute
pancreatitis. Eur J Intern Med 2009; 20:43–8. [PMID: 19393477]
- Uhl W, Isenmann R, Curti G. Influence of etiology on the course and
outcome of acute pancreatitis. Pancreas 1996; 13:335–343. [PMID: 8899793]
- Cho J, Kim T, Kim S. Comparison of clinical course and outcome of
acute pancreatitis according to the two main etiologies: alcohol and
gallstone. BMC Gastroenterol 2015; 15:1-7. [PMID: 26209440]
- Zheng Y, Zhou Z, Li H, Li J, Li A, Ma B, et al. A multicenter study on
etiology of acute pancreatitis in Beijing during 5 years. Pancreas 2015;
44:409-14. [PMID: 25438072]
- Martin BJ, Chen G, Graham M, Quan H. Coding of obesity in
administrative hospital discharge abstract data: accuracy and impact
for future research studies. BMC Health Serv Res 2014; 14:70.
[PMID: 24524687]
- Gupta R, Villa M, Agaba E, Ritter G, Sison C, Marini CP, et al. The effect
of body mass index on the outcome of critically ill surgical patients. JPEN J
Parenter Enteral Nutr 2013; 37:368-74. [PMID: 23019130]
- Padwal R, Leslie WD, Lix LM, Majumdar SR. Relationship Among Body
Fat Percentage, Body Index, and All-Cause Mortality: A Cohort Study. Ann
Intern Med 2016; 164:532-41. [PMID: 26954388]

