Bahareh Nazemisalman1, Surena Vahabi2*, Shayan Darvish3
1Pedodontics Department, Dental school, Zanjan University of Medical Sciences, Zanjan, Iran
2Periodontics Department, School of Dentistry, University of Medical Sciences, Tehran, Iran
3Pardis Health Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
*Corresponding Author:
Surena Vahabi
Dental Research Center, Research Institute
of Dental Sciences, Shahid Beheshti
University of Medical Sciences, Tehran, Iran
E-mail: ivsure1@gmail.com
Received Date: February 20, 2018 Accepted Date: March 05, 2018 Published Date: March 12, 2018
Citation: Nazemisalman B, Darvish S, Vahabi S. Oligodontia Management in Patients with Ectodermal Dysplasia Syndrome. Periodon Prosthodon. 2018, Vol.4 No.1:04. doi: 10.21767/2471-3082.100040
Copyright: © 2018 Nazemisalman B. This is an open-access article distributed under the terms of the creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Background and aim: A relatively common sex- linked dermatitis characterized by a congenital dysplasia of one or more ectodermal structures is Ectodermal dysplasia (ED). Common signs include fragile skin and nails, defective teeth and salivary glands, frontal bossing with prominent supra orbital ridges, nasal bridge depression and protuberant lips. There are often a few conical teeth existing (hypodontia or Oligodontia) that results in generalized spacing. Deciduous and/or the permanent dentition may fail to form (anodontia), and, consequently, hypoplasia of jaws may happen in both cases. This article reports a case of ED and shows how to handle it.
Case report: A 5 years old girl with HED visited SBMU, school of dentistry. Clinical examination showed hypotrichosis following the missing of eyelashes and eyebrows, dry skin, saddle nose and pigmentation on the legs which are characteristics of ED. Partial denture for lower jaw and composite restoration for upper jaw was used as the treatment plan.
Conclusion: Preventive treatments are very crucial to save present teeth in ED patients. One treatment option is to use removable dentures as a cost-benefit and desired intermediate treatment to restore both function and esthetics and improve patient’s psychological status in Oligodontia cases.
Keywords
Oligodontia; Ectodermal dysplasia syndrome; Lymphocyte; Mandibular
Introduction
Ectodermal dysplasia (ED) is commonly known as a rare inherited disorder characterized by defective development of ectodermal origin tissues with occasional dysplasia of mesodermal tissues [1]. Sparse hair (Hypotrichosis), abnormal or missing teeth (Hypodontia or Oligodontia) and sweating disability (Anhydrosis or Hyphlydrosis) are the major signs of ED and minimum two of these features are necessary to confirm its diagnose [2]. ED incidence is reported to be approximately 1 in 100.000 live births [3] and its mortality rate has been reported as high as 30% in infancy and early childhood due to intermittent hyperpyrexia [4]. There are two different forms of the disease: the 1st one, Clouston syndrome, has autosomal inheritance. The second one, Christ- Siemens Syndrome (Hypohidrotic form), usually an X-linked recessive which is only expressed in males [5]. Spontaneous gene mutation can also result in this condition [6]. ED got several clinical manifestations and facial abnormalities such as prominent forehead, saddle nose and thick lip, linear wise and hyper pigmentation around the eyes, hypoxemia or anodontia. Reduced alveolar bone growth can be happen as a result of teeth absence which often has a narrow and concave lingual clinical appearance [7,8]. Decreased function of lymphocyte and cellular immune hypo function is one of the symptoms in ED patients which may lead to infection. One of the most important challenges in treating such patients is to achieve an improved appearance. Since the presence of teeth has a great influence on patient’s self-steam, such treatment is critically necessary to be well defined. In this matter, prosthetic replacement for the teeth is crucial for such individuals including partial and complete dentures as it will improve their social engagements especially in school age [9-11]. This article deals with the importance of prosthetic management of a young kid and its effect on her social life.
Case Report
A 5-year-old girl visited the school of Dentistry, Shahid Beheshti University of medical Sciences with chief complaint of missing teeth. While mastication was also a problem, but the main complaint of the patient was about esthetic problems since it is a more important factor for girls than boys. Comparing to the other case this case was more complaining about esthetics and less about mastication due to the fact that she had more teeth as visible in the panoramic cliché (Figure 1). Clinical examination showed hypotrichosis which also includes the eyelashes and eye brows. From the sagittal view, the saddle nose and prominent forehead were visible (Figures 2A and 2B). Dry skin and nails with malformation of fingers and pigmentation in legs were other clinical manifestations, this becomes more to attention in girls than boys because esthetic is more valuable in girls (Figure 2C). The patient also had sweating problems which is one of the major problems in ED that can cause the body temperature to rise very easily, this is important especially in kids when affected by infection since their body is weak and immediate action should be taken, thus it is also important to identify these kids early and dentists can play an important role in this matter by a simple clinical and dental examination. Dental examination showed Oligodontia with only A, C and E tooth present in the upper jaw along with C and E in the lower jaw. Both maxillary and mandibular primary canines were conical (Figure 3A). It seemed she probably had a familial heredity of Oligodontia because her mother's maxilla, in anterior part, was similar to her daughter but she does not permit us for more assessment. After prosthetic consultation, the treatment plan was set as to do an overdenture for mandibular and composite reshaping for maxillary teeth. The maxillary present teeth were initially reshaped using composite resin restoration materials (Filtek z250, 3M ESPE, USA). This was considered as a desired intermediate treatment until her prosthetic could be performed in a later stage. 2 primary canines were used for abutments of the overdenture (Figures 3B-3D). Any other permanent treatment shall be postponed until complete growth of the jaws. It is important to maintain and keep the tooth since they are necessary for jaws growth. This case was treated in the dental unit chair in dental school unlike the previous one as she was cooperating. Follow ups were determined for every 6 months after the treatment. As the permanent maxillary central incisors started to grow, gradually, the composite restorations were trimmed and modified to create space for them. The results of follow ups were again as the previous case, first the acceptance was good since esthetic and function of the kid’s teeth were improved but followed by a limited use of the denture due to unsatisfactory motivation and control of parents.
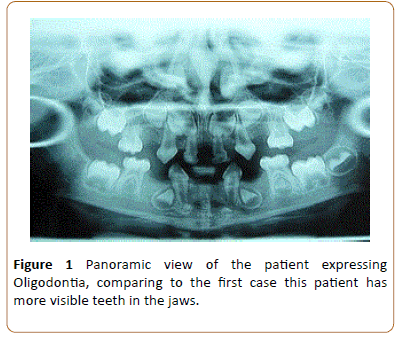
Figure 1: Panoramic view of the patient expressing Oligodontia, comparing to the first case this patient has more visible teeth in the jaws.

Figure 2: A, B: Lack of Eye lashes and eye brows, flattened nose bridge and hypotrichosis. C: Malformed fingers and hyper pigmentation in legs along with dry skin and nails.
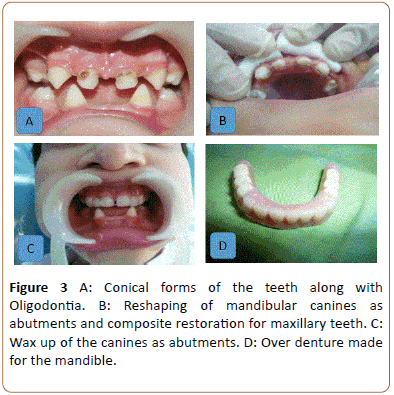
Figure 3: A: Conical forms of the teeth along with Oligodontia. B: Reshaping of mandibular canines as abutments and composite restoration for maxillary teeth. C: Wax up of the canines as abutments. D: Over denture made for the mandible.
Discussion
Appearance of the children is depending highly on a natural smile and any defect interfering with smile could directly influence several aspects of their life. Initial management of such conditions is required in order to impress the self-steam of such patients while facilitating the correct mastication and pronunciation [7]. Characteristically thin and underdeveloped residual ridge is presented in these groups which are covered by a thin layer of mucosa topped by a cord of movable connective tissue [5]. Most common dental treatment for ED is use of a removable denture [10]. It is recommended, therefore, to initiate the treatment by a removable that is found to be more tolerable for children when at a school age [11]. By the time of school age, children are considered old enough to recognize their esthetic issues and usually show willingness to improve it. Alternative treatment modalities which are suggested including dental implant and implant borne total denture in immature and no cooperative patients [12]. It is usually recommended to postpone the use of Osseointegrated implants for children until complete growth. It is necessary for a periodic follow up as growth changes occur and it is critical to adapt the prosthesis to improve both esthetics and function. Usually, it is recommended to postpone the use of osseointegrated implants for children until complete growth. Removable partial dentures are often indicated for children and adults with ED [13,14]. The main factors to make a decision between removable partial denture and an overdenture are presence of natural posterior teeth, facial esthetics, lip support, number and size of existing natural teeth, and the vertical dimension of occlusion [15]. All changes in the dental arches, including alveolar bone growth in response to tooth eruption, should be considered to ensure appropriate adjustments are constantly implied. Long-term treatment is an active process that must be constantly adjusted according to the child’s development and growth [16]. In a study by Pinto et al., following prosthetic rehabilitation, the child experienced a wider variety of foods and thus improved his/her nutrition [17]. Children should always perform standard oral hygiene and take care of the devices personally. In their study, dental implants were not recommended since cone beam computed tomography revealed that both maxillary and mandibular micrognathism had occurred as the result of missing teeth. Cephalometric analysis indicated that patient must be followed up to assess bone growth after placement of prosthesis [17]. The authors recommended early prosthetic treatment in patients with this syndrome, especially at a school-age.
In our case, initial acceptance, eating and esthetic appearance were very good following the delivery of removable partial denture as it really needs good cooperation of the child. If the child fails to use it full time, obviously some objectives of treatment will not be achieved, and this point is very important when considering such treatment plans for ED patients.
Conclusion
The patient showed a desire and achieved the goal by replacing her teeth for a more social engagement while improving bite and speech though, followed by a reduction in use in follow up sessions. Thus, based on the information and experience gained in treating this case, it appears that communication between professionals and parents play a key role to gain a successful result in treating ED patients.
References
- Dhanrajani PJ, Jiffy AO (1998) Management of Ectodermal Dysplasia. A Literature Review. Dent Update 25: 73-75.
- Rouse C, Siegfried E, Breer W, Nahass G (2004) Hair and sweat glands in families with hypohidrotic ectodermal dysplasia: further characterization. Arch Dermatol 140: 850-855.
- Kupietzky K, Milton H (1995) Hypohidrotic ectodermal dysplasia: Prosthetic management of hypohidrotic ectodermal dysplasia. Quintessence Int 26: 285-291.
- Clauss F, Maniere MC, Obry F, Waltmann E, Hadj-Rabia S (2008) Dento-craniofacial phenotypes and underlying molecular mechanisms in hypohidrotic ectodermal dysplasia (HED): A Review. J Dent Res 87: 1089-1099.
- Motil KJ, Fete TJ, Fraley JK, Rebecca J Schultz, Thomas M Foy (2005) Growth characteristics of children with ectodermal dysplasia syndromes. Pediatrics 116: 229-234.
- Clarke A (1987) Hypohidrotic ectodermal dysplasia. J Med Genet 24: 659-663.
- Kupletzky A, Houpt M (1995) Hypohydrotic ectodermal dysplasia: characteristics and treatment. Quintessence Int 26: 285-291.
- Tanner BA (1988) Psychological aspects of hypohidrotic ectodermal dysplasia. Birth Defects Orig Artic Ser 24: 263-275.
- Kaercher T (2004) Ocular symptoms and signs in patients with ectodermal dysplasia syndromes. Graefes Arch Clin Exp Ophthalmol 242: 495-500.
- Nowak AJ (1988) Dental treatment for patients with ectodermal dysplasia. Birth Defects Orig Artic Ser 24: 243-252.
- Lowry RB, Robinson GC, Miller JR (1966) Hereditary ectodermal dysplasia. Symptoms, inheritance patterns, differential diagnosis, management. Clin Pediatr (Phila) 5: 395-402.
- Lypka M, Yarmand D, Burstein J, Tso V, Yamashita DD (2008) Dental implant reconstruction in a patient with ectodermal dysplasia using multiple bone grafting techniques. J Oral MaxilloFac Surg 66: 1241-1244.
- Vasconcelos Carvalho M, Romero Souto de Sousa J, Paiva Correa de Melo F, Fonseca Faro T, Nunes Santos AC et al. (2013) Hypohidrotic and hidrotic ectodermal dysplasia: a report of two cases. Dermtol Online J 19: 11.
- Derbanne MA, Sitbon MC, Landru MM, Naveau A (2010) Early prosthetic treatment in children with ectodermal dysplasia. Eur Arch Paediatr Dent 11: 301-305.
- Maroulakos G, Artopoulou II, Angelopoulou MV, Emmanouil D (2016) Removable partial dentures vs overdentures in children with ectodermal dysplasia: two case reports. Eur Arch Paediatr Dent 17: 205-210.
- Dellavia C, Catti F, Sforza C, Tommasi DG, Ferrario VF (2010) Craniofacial growth in ectodermal dysplasia: an 8-year longitudinal evaluation of Italian subjects. Angle Orthod 80: 733-739.
- Pinto AS, Melo Val Alencar C, Costa Oliveira L, Costa de Aquino C, Vasconcelos DF (2016) Prosthetic management of a child with hypohidrotic ectodermal dysplasia: 6-year follow-up. Case Rep Dent.

