Keywords
Cervical cancer; Screening program; SWOT analysis; Opportunities; Challenges; China
Introduction
Because of its large population, China carries a heavy burden of cervical cancer, especially in rural areas. In China, although there was a steady incidence trend of 7.4/100,000 in rural areas from 2007 to 2009, the national incidence has increased by 200.0% from 2003 (3.8/100,000) to 2012 (11.4/100,000). The national mortality rate for cervical cancer has also increased incrementally, with an overall increase in that period of 116.7% [1-3]. In order to reduce the high cervical cancer burden in rural areas, the Chinese government implemented several important measures, including the implementation of the National Cervical Cancer Screening Program in Rural Areas (NCCSPRA) since 2009. It was the first time that the Chinese government had proposed to gradually widen access in rural areas to cervical cancer screening services and it represented a step towards nationwide provision of cervical cancer screening.
However, since its launch, there has been no systematic national level research about the implementation of the program. Evaluating the performance of this program is necessary to guide policymakers in making future decisions. This research will fill the gap by assessing the performance of the current program, identifying the strengths, weaknesses and challenges of this program and suggesting strategies for policymakers to improve the program and make decisions about how to improve it before extending it nationwide.
Methodology
A mixed qualitative and quantitative method was conducted between September 2015 and April 2016 in China.
Data sources
There were three types of sources of data in this research. They were from secondary data, online survey and field investigation. Both quantitative methods (e.g. questionnaire survey) and qualitative methods (e.g. literature review, in depth review and expert review) were used.
Secondary data
In this research, the information about the number of women who received the screening service, screening coverage and the number of the national project counties from 2009 to 2015 was collected from the National Cervical Cancer Screening Information Reporting System (NCCSIRS).
Online survey
Written questionnaires were used for collecting information about funding, equipment, training, staff, availability of services, supervision and quality control. There were three types of written questionnaires in this research. They were a management questionnaire, hospitals’ questionnaire and a health care providers’ questionnaire. A total of six project counties in each province (total 31 provinces) were asked to answer the management questionnaire, of these, 183 project counties responded to it.
Field investigation
Considering geographic distribution and economic development, Liaoning, Hubei and Shaanxi provinces (representing the three geographical regions of China: Eastern, Central and Western China) were selected as survey implementation areas. Within each province, two counties from the NCCSPRA were selected randomly as the field survey areas. Two towns that carry out the program were randomly sampled from the counties surveyed.
The hospitals questionnaire was designed for all of the hospitals that provided cervical cancer screening services in the field survey areas. The key contents of this questionnaire consisted of availability of services, staff, training and expenditure. A total of 58 hospitals were recruited in this survey. The health care providers’ questionnaire was designed for the health care providers who provided cervical cancer screening services in the hospitals in the field survey areas. A total of 135 health care providers were recruited and completed this questionnaire in this research. Face-to-face interview questionnaires were utilized to collect information from the target women, about knowledge of cervical cancer prevention. A total of 308 women who received cervical cancer screening services as part of the NCCPSA were recruited in the investigation. An expert review was used to assess the quality of Pap smear tests by reviewing sets of slides previously interpreted by cytopathologists in the project counties visited. A total of 170 positive smear slides and 110 negative smear slides from the project counties visited were collected for this research. In-depth interviews were used to explore the participants’ experience, and the needs, barriers, problems and their suggestions about the NCCSPRA. A total of 18 persons across field visits project counties were interviewed for this research. This study was approved by the Ethics Committee of Griffith University, Queensland, Australia (GU Ref No: ENV/33/13/HREC).
Statistics analysis
In this research, the questionnaire data were entered into EpiData 3.2 with dual entry verification, consistency, and logic error checking. Statistical analyses were performed by SPSS 22.0, with p-value<0.05 determined as the threshold of statistical significance. The qualitative analysis included the following steps: firstly, the codable units from in-depth interviews and focus groups were classed under the following words: policy, funding, health education, training, supervision and quality control, knowledge, challenges, barriers, experience. The next step was to understand the meaning of what was said. Based on the meanings, groups of data with similar meanings were gathered in larger categories. Final step was to connect the different categories to analyse the opportunities, barriers and challenges to the implementation of this program.
Results
Coverage rates of target population and national project counties
The findings from secondary data showed that during the 2009 to 2011 period, although 11.69 million rural women aged between 35 and 59 years received free cervical cancer screening, this represented only 8.40% (11.69/139.22 million) of all rural women aged 35-59 years. In 2012-2014, 31.20 million rural women aged 35-64 years received free cervical cancer screening in the national project counties, representing 19.99% (31.2/156.06 million) of all rural women aged 35-64 years. During the 2009 to 2015 period, the number of national project counties expanded, from 245 in 2009 to 1299 in 2015, representing 8.6% (245/2858) of all counties nationwide in 2009 and 45.5% (1299/2853) in 2015 (Figure 1). Moreover, 13 provinces, representing 41.9% of all provinces have already carried out cervical cancer screening funded by different level of governments in the whole province and covering all of the 35-64 years old women whether in urban or in rural areas.
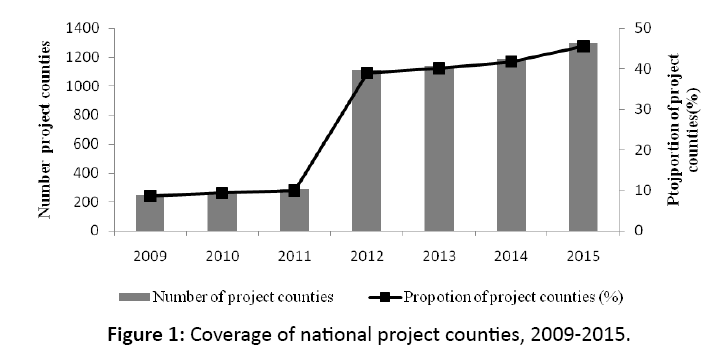
Figure 1: Coverage of national project counties, 2009-2015.
Service capacities
The results from online survey showed that from 2012 to 2014, the proportions of project counties which had cytopathologists, pathologists and colposcopists increased as the years progressed and statistically significant differences in the proportions were seen across different years (p<0.001) (Table 1).
| Project counties |
N |
2012 |
2013 |
2014 |
χ2 |
p |
| n |
% |
n |
% |
n |
% |
| Having cytopathologists |
183 |
112 |
61.2 |
162 |
88.5 |
164 |
89.6 |
39.842 |
0.000 |
| Having pathologists |
183 |
109 |
59.6 |
153 |
83.6 |
160 |
87.4 |
46.978 |
0.000 |
| Having coploscopists |
183 |
121 |
66.1 |
172 |
94.0 |
176 |
96.2 |
82.555 |
0.000 |
Table 1: Differences in proportion of project counties with cervical cancer screening service providers in different years (From Chi-square test).
Although the numbers of the service providers in project counties increased with years. The results from field survey showed that among cytologists and histologists, none had a university or higher degree. About 40-50% of gynaecologists, colposcopists and cytolopathologist had a primary qualification. Half of cytologists had less than 5 years’ service (Table 2).
| Characteristics |
Gynaecologist |
Colposcopists |
Cytolopathologist |
Pathologist |
| Education level |
|
|
|
|
| University or higher |
29 (33.7) |
7 (21.9) |
0 (0.0) |
0 (0.0) |
| Junior college |
38 (44.2) |
21 (65.6) |
6 (75.0) |
6 (75.0) |
| Senior/technical school |
19 (22.1) |
4 (12.5) |
2 (25.0) |
2 (25.0) |
| Technical qualification* |
|
|
|
|
| No qualification |
0 (0.0) |
0 (0.0) |
2 (25.0) |
0 (0.0) |
| Primary |
41 (47.1) |
13 (40.6) |
4 (50.0) |
2 (25.0) |
| Middle |
33 (37.9) |
10 (31.3) |
2 (25.0) |
4 (50.0) |
| Senior |
13 (14.9) |
9 (28.1) |
0 (0.0) |
2 (25.0) |
| Years of service (years) |
|
|
|
|
| 1-5 |
17 (19.8) |
7 (21.9) |
4 (50.0) |
0 (0.0) |
| 6-10 |
11 (12.8) |
3 (9.4) |
2 (25.0) |
2 (25.0) |
| 11-20 |
40 (46.5) |
17 (53.1) |
0 (0.0) |
2 (25.0) |
| >20 |
18 (20.9) |
5 (15.6) |
2 (25.0) |
4 (50.0) |
* In China technical skill is recognized through “Technical Qualifications” at three levels”
Table 2: Education status and technical qualification among health care providers who provided different services within the NCCSPRA.
“Primary technical qualification” means a basic level of skill. “Middle technical qualification” is given to workers who have improved their skills through experience. “Senior technical qualification” is used for workers with advanced skill – highly experienced workers. In some hospitals, workers need to pass an examination or an expert review or even (for senior level) publish research papers to advance to a higher qualification.
The results also revealed that the educational level, technical qualification and service years of health care providers in more developed and developed regions were statistically significantly higher and longer (p<0.05) than in less developed regions. The technical qualification of health care providers in more developed regions was statistically significantly higher (p<0.05) than in developed regions (Table 3).
Characteristics |
More developed regions |
Developed regions |
Less developed regions |
χ2 |
p |
| Education level bc |
|
|
|
|
|
| University or higher |
7 (53.8) |
20 (27.4) |
13 (27.1) |
96.439* |
0.000 |
| Junior college |
6 (46.2) |
51 (69.9) |
1 (2.1) |
| Senior/technical school |
0 (0.0) |
2 (2.7) |
34 (70.8) |
| Technical qualification a b c |
|
|
|
|
|
| No qualification |
1 (11.1) |
7 (8.8) |
8 (17.4) |
23.181* |
0.000 |
| Primary |
1 (11.1) |
35 (47.4) |
28 (56.9) |
| Middle |
8 (61.1) |
31 (42.1) |
9 (19.3) |
| Senior |
3 (19.4) |
1 (1.8) |
3 (6.4) |
| Years of service bc |
|
|
|
|
|
| 1-5 |
1 (7.7) |
14 (18.9) |
21 (46.7) |
|
|
| 6-10 |
1 (7.7) |
14 (18.9) |
7 (15.6) |
20.337* |
0.001 |
| 11-20 |
10 (76.9) |
30 (40.5) |
8 (17.8) |
|
|
| >20 |
1 (7.7) |
16 (21.6) |
9 (20.0) |
|
|
* Fisher’s Exact Test
aIndicates a statistically significance significant difference between more developed and developed regions
bIndicates a statistically significance significant difference between more developed and less developed regions
cIndicates a statistically significance significant difference between developed and less developed regions
Table 3: Differences in education status and technical qualification among health care providers in different regions (From Chi-square test).
From 2012 to 2014, the proportion of project counties which had colposcopes increased with years, from 65.6% in 2012, 92.9% in 2013 to 95.1% in 2014. Statistically significant differences in the proportions were seen in different years (p<0.001). The numbers of colposcopes in project counties increased with years. The mean number of colposcopes increased from 3.02 in 2012 to 4.92 in 2014. A significant difference was found in the numbers of colposcopes in different years (p<0.001).
The analysis results derived from expert review showed that there was a statistically significant difference of the adequate cytology rates and interpretation agreement rates between before and after program complementation (p<0.05). The adequate cytology rates and interpretation agreement rates increased from 92.9% and 57.4% to 99.5% and 69.1%, respectively.
Funds investment
The results from online survey showed that most of the funds came from different levels of government. Funds from the central government accounted for the largest proportion (almost 50%), followed by provincial, municipal and county matching funds (Figure 2).
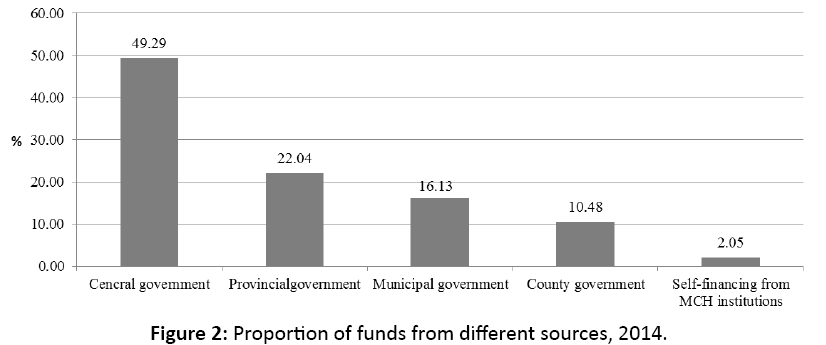
Figure 2: Proportion of funds from different sources, 2014.
In 2014, in 11.5% (21/182) of the surveyed project counties, central government funding was the sole source of project funding. The largest number of project counties which only received funding from central government (42.9%) was in less developed regions, 38.1% in developed regions and 19.0% in more developed regions.
Health awareness and knowledge of cervical cancer prevention among target women
The results derived from the field survey showed that, the overall knowledge about cervical cancer prevention among target women was low. About 30-40% of the respondents were unaware of risk factors and prevention measures of cervical cancer. Only 33.1% of participants believed that cervical cancer screening could enable “early diagnosis of cervical precancerous lesions or cancer”. About 60-70% of participants believed that positive screening result means suffering from cervical cancer or precancerous lesions. As the results derived from the in-depth review showed that, because many target women lack awareness to participate in screening independently, most of the screening hospitals took many measures to encourage them to attend screening, including ferrying women to screening locations for free, giving gifts, providing free ultrasound examination or free medicines for women who were diagnosed with STIs by screening.
SWOT Analysis
Strengths
Coverage rates of target population and national project counties have increased over time: As showed in above results, more and more rural area women received free cervical cancer screening services and more and more counties received funding from central and local governments to provide free services and improve their capacities.
More appropriate screening tests are being used in NCCSPRA: The Pap smear (cytology) is the screening test that has been used for population-based screening in high-income countries and it has been shown to reduce cervical cancer incidence and mortality [4]. It is the main screening test used in NCCSPRA [5]. However, taking into account the shortage of laboratories and sufficiently skilled technicians, in 2014, the HPV DNA test was introduced into pilot areas of NCCSPRA [6]. Compared with Pap smear and VIA/VILI, the HPV test has the following advantages over the Pap smear test: simple process for collection of specimens, allowing the possibility of self-collected specimens; automated processing; high sensitivity and long screening interval (5 years) [4]. Therefore, using the HPV test in the program is a good step forwards improving the ineffectiveness of the program.
Service capacities have gradually improved: As showed in above results, the numbers of service providers and the amount of equipment in project counties increased a lot during the program implementation. Moreover, the quality of services of cytology in project counties also improved with years.
Weaknesses
Low screening coverage rate: WHO recommends that high coverage, around 80% of the population at risk of cervical cancer, is an important factor for a successful screening program [7]. However, although the target population is these aged 35-64 years in rural areas, the free cervical cancer screening services is not available to all of the 35-64 years old rural women in the NCCSPRA. The number of target women who can receive the free service is decided by the quota from the central government [5,6,8]. The quota of women eligible to access the free service was 10 million per year. This figure represents a screening coverage of only 20% of eligible rural women. For this reason, increasing the screening coverage of rural women in China must be a priority.
Insufficient compensation from the government to screening hospitals: Although the target women receive a free screening service, the funds from the program do not cover the full cost of the program because of the large target population. They only provide the costs for screening tests and diagnosis [5,6,9,10]. The central government requires local governments to contribute part of the cost, depending on the prosperity of the region. The central government contributes 80% in less developed regions, 60% in developed regions, and 10% in more developed regions. The rest of the funds come from the local government [5]. However, as showed in above results, most of project counties which only receive funding from central government.
Opportunities
Government recognises the importance of women’s health: Especially, in recent years, the Chinese government has paid more attention to cervical cancer control. The National Program on the Development of Chinese Women (2011-2020) (NPDCW) [11] identified “women and health” as the first consideration out of the seven fields of health, education, economy, political participation, social security, environment and law. Within the main objectives of the NPDCW, “improving the rates of early diagnosis and treatment of cervical cancer, reducing mortality of cervical cancer” was explicitly prioritized. Moreover, the strategies and measures of NPDCW emphasized “increasing investment in special funds for cervical cancer prevention and control, expanding the coverage rate of cervical cancer screening, strengthening training of professional knowledge and skills for grass-roots women health care providers, improving the capacities of diagnosis and treatment of cervical cancer of healthcare facilities, providing subsidy of treatment for the poor and critical patients”. In 2015, NHFPC combined with the National Development and Reform Commission and the other 14 ministries and commissions released the Chinese Three-year Action Plan on Cancer Prevention (2015-2017). The action plan also prioritized expanding the coverage of cervical cancer screening, early diagnosis and treatment.
Medical security system and relevant policies have constantly improved: The coverage of basic medical insurance – Urban Employee Basic Medical Insurance (UEBMI), Urban Resident Basic Medical Insurance (URBMI) and New Rural Cooperative Medical System (NRCMS) has expanded. In 2014, the total number of insured people was over 1.3 billion. All of the insurance rates are more than 95.0%. Among the insured people, a total of 270 million women accessed UEBMI and URBMI. This increased by about 8.0 million than 2011. At the same time, a total of 740 million people accessed NRCMS. The insurance rate reached 99.0%. It increased by 3.0% than 2011 [12]. In 2015, within the scope stipulated by policy, the maximum compensation rate reached 50% and 75% of outpatient and inpatient expenditure, respectively [13]. By the end of 2014, the pilot program of serious illness insurance for urban and rural residents covered 700 million of residents across all provinces of China. The actual reimbursement rate of patients with serious illness increased by 10-15% based on the basic medical insurance reimbursement [14]. In order to ensure that all of the women who were diagnosed with pre-cancer lesions or cervical cancer could receive treatment, they also established Special Rescue Funds for poor cervical cancer patients [9]. Although the subsidy from this fund is not enough to pay all of the treatment costs, it at least partly reduces individual’s worries about not having enough money for treatment.
A screening network has been established: The Maternal and Child Health (MCH) institutions at all levels are responsible for implementation of the program [15]. In 2015, there were a total of 3062 MCH institutions. Of these, 30 were at provincial level, 330 at city level and 2709 at county level. They covered 96.8% (30/31), 99.1% (330/333) and 95.0% (2709/2853) of provinces, cities and counties, respectively [16]. During the implementation of NCCSPRA, the township level hospitals also take all important responsibilities for collection and fixation of the smear, collection of HPV DNA specimen or providing VIA/ VILI tests. In 2012, there were 37,097 township level hospitals. They covered 100% of townships [17]. In 2015, the General Office of the State Council of China issued the Planning Outline of National Health Care System (2015-2020) [18]. It set specific indicators of numbers of staff and standardized construction of township hospitals. It also emphasized that the key responsibility of grassroots hospitals is to provide basic health care services, including prevention, health care, health education and family planning. All of these provided the basis for the expansion of the coverage of cervical cancer screening. It means that a very extensive screening network has been established.
Threats
A shortage of competent health care personnel: Although the numbers of the service providers in project counties increased with years. The results from field survey showed that the educational level, technical qualification and service years of service providers in project counties were not optimistic, especially in less developed regions. This shortage of qualified service providers poses a significant barrier to the delivery of quality cervical cancer screening services across rural areas of China [7,19].
Low health awareness and knowledge of cervical cancer among target women: As the above results indicated that women’s knowledge about cervical cancer in project counties was inadequate. The Guideline for Comprehensive Cervical Cancer Prevention and Control of WHO mentions that one of the barriers to control of cervical cancer is lack of knowledge cervical cancer and its prevention [7]. The reason of this is that lack of knowledge was a significant barrier to attending screening program [20,21] and the effectiveness of participation could reduce mortality and incidence [19,22]. Moreover, the above results also showed that in order to improve the participation rate, many various measures were taken to encourage the women to participate in the screening. This resulted in the cost of organizing women to participate in the screening accounting for the largest part of the cost of the program. Such funds could be diverted to many other deficit areas of the program if women were more aware of risk factors, benefits of follow up and were more motivated to participate follow up.
Rapid increase in migration from rural to urban areas: With rapid urbanization and economic growth, more and more rural labour has entered the cities seeking employment opportunities. Based on the national census data, the estimated number of rural migrant workers was 20 million in 1990, 45 million in 1995, and 79 million in 2000 [23]. By 2015 this number had grown to 277 million [24]. Millions of rural people in the central and western regions have flooded into eastern industrial centres to work and this pattern of internal movement accounts for 72.4% of all migrant workers [25]. As the results derived from in-depth review showed that, about 30-40% of the target women in project counties in less developed regions have moved to cities seeking jobs. However, according to the plan of NCCSPRA, the target women only receive the free cervical cancer screening service in their original (rural) registration location. Thus the free cervical cancer screening services for about 30-40% of the target women in project counties in less developed regions is not available. In addition, with the increase of migration from rural to urban areas, it was difficult to follow up the women with abnormal results. Furthermore, according to the National Plan on New Urbanization (2014-2020), with the urbanization process accelerated, approximately 100 million rural migrant workers will be resettled in cities and towns and will have urban hukou (household registration) by 2020 [26]. This phenomenon will create greater challenges in implementation of the NCCSPRA.
Discussion and Recommendation
The analysis provided here clearly shows that the effectiveness of an organized cervical cancer screening program is not only influenced by internal factors (strengths and weaknesses) related to the program itself but also by external factors (opportunities and threats). Therefore, in order to improve the implementation of the organized cervical cancer screening program in China, multi-strategy actions need to be considered to strengthen the advantages, seize the opportunities, overcome the weaknesses and confront the threats.
First, it is necessary to gradually adjust the cervical cancer screening policy and extend screening coverage. In order to develop an achievable and more effective strategy for increasing the screening coverage rate, it is necessary to consider both short-term and long-term strategy actions. For short-term action, there is need to extend the quota of target women in NCCSPRA. For long-term action, it is necessary to extend the program to all 35-64 years old women.
Second, there is a need to consider covering the cost of screening service by medical insurance. As showed above, one of the weaknesses is insufficient compensation of the government to screening hospitals. If China government further extend the quota of target women or extend the program to all 35-64 years old women, the lack of screening funding could be more serious. Therefore, it is necessary to seize the opportunities – medical security system has constantly improved – to incorporate the cost of screening service into the medical insurance.
Third, it is necessary to establish systematic capacity building and training programs. As showed above, lack of qualified service providers was one of threats to the implementation of the program. Therefore, systematic capacity building and training should be given high priority for future development of cervical cancer prevention and control.
Final, it is necessary to develop and implement a national health education program. Numerous studies have shown that many barriers to cancer screening programs, such as lack of awareness of the risk of cervical cancer, can be addressed through education of the community. Health education can ensure optimal program coverage and motivate individuals to follow up treatment, which in turn, will lead to enhanced program impact. As showed above, the overall knowledge about cervical cancer prevention among target women was low. Therefore, strengthening health education is a critical activity. The following measures need to be considered. They include: to standardize information of health education and improve the knowledge skills of health educators, use new media to extend health education coverage and to strengthen health education at the national level.
Acknowledgement
This study was partially supported by grants from MCH hospitals in Xunyang and Hanbin in Shaanxi province, Xiangzhou and Zaoyang in Hubei province, and Zhuanghe and Wafang Dian in Liaoning province. We are grateful to all the health careworkers who participated in the study.
References
- NCC, DPCB, NHFPC. Chinese cancer registry annual report 2013. Military Medical Science Press, Beijing 2013.
- Wanqing C. Report of cancer incidence and mortality in China, 2012. China Cancer 2016; 25: 1-11.
- NOCPC, NCCR, DPCB. Chinese cancer registry annual report 2004. Beijing Union Medical University Press, Beijing 2008.
- WHO. Comprehensive cervical cancer control: A guide to essential practice Second edition. WHO Press, Geneva 2014.
- https://www.moh.gov.cn/fys/s7900/200906/cd3c33a7ad624a50b8100b262041dabe.shtml
- NHFPC. Notification about carry out major women and children's public health program in 2014. Women and Chirden's Health Services, Editor 2014.
- WHO. Comprehensive cervical cancer control A guide to essential practice. WHO press, Geneva 2006.
- MOH. Notification about carry out major women and children's public health program in 2012, Women's health and community health, Editor. Ministry of Health of the People's Republic of China, Beijing 2012.
- MOH. Record of process of major women and children's public health program in press conference. MOH 2012.
- NHFPC. Notification about carry out major women and children's public health program in 2013. Maternal and Children's Health Services, Editor 2013.
- The State Council of China. Outline for the Development of Chinese Women (2011-2020). t.S.C.o.P.R.o. China, Editor 2011.
- https://www.stats.gov.cn/tjsj/zxfb/201511/t20151127_1282257.html
- GOSCPRC. Notice of the 2014 wrap-up report and 2015 major task list on deepening the medical and health care system reform. State Council of the People's Republic of China, Editor 2015.
- https://paper.people.com.cn/rmrb/html/2015-05/10/nw.D110000renmrb_20150510_5-03.htm
- Jiangli D, Shannon R, Cordia C. Review of the cervical cancer burden and population-based cervical cancer screening in China. Asian Pacific Journal of Cancer Prevention 2015; 16: 7401-7407.
- NCWCH, CC.The report of resources and operation situations of MCH institutions in 2014. National Center for Women and Children's Health, China 2015.
- MOH. China's health statistics yearbook 2013. Peking Union Medical College Press, Beijing 2013.
- GOSCPRC. Planning outline of National Health Care System (2015-2020), G.O.o.t.S.C.o.t.P.s.R.o. China, Editor. The State Council of the People's Republic of China, Beijing 2015.
- IARC, IARC. Handbooks of cancer prevention. IARC Press, Geneva 2005.
- Shea J, Klainin-Yobas P, Mackey S. Young Singaporean women's knowledge of cervical cancer and pap smear screening: A descriptive study. J Clin Nurs 2013; 22: 3310-3319.
- Yanikkerem E. Knowledge about cervical cancer, pap test and barriers towards cervical screening of women in Turkey. J Cancer Educ 2013; 28: 375-383.
- Anttila A. Cervical cancer screening policies and coverage in Europe. Eur J Cancer 2009; 45: 2649-2658.
- Qin XZ, Pan J, Liu GG. Does participating in health insurance benefit the migrant workers in China? An empirical investigation. China Economic Review 2014; 30: 263-278.
- NBS. National economic and social development statistics bulletin. National Bureau of Statistics, Beijing 2013.
- Yao HQ, Ren ZZ. Report on economic development in western regions of China. Social Sciences Academic Press, Beijing 2007.
- Central committee of the communist party of china and state council of China. Central Committee of the Communist Party of China, State Council of China, Beijing 2014.

