Keywords
Absorptiometry, Photon; Osteoporosis; Pancreatitis;
Prevalence; Risk Factors
Abbreviations
BMD bone mineral density; BMI body mass index;
CP chronic pancreatitis; EPI exocrine pancreatic insufficiency
INTRODUCTION
Chronic pancreatitis (CP) is a progressive, inflammatory
disease leading to fibrosis and functional impairment of
the pancreatic gland a [1], which ultimately affects the
exocrine and endocrine function. Exocrine pancreatic
insufficiency (EPI) often leads to maldigestion with ensuing
malabsorption of micronutrients such as fat-soluble
vitamins including vitamin-D [2]. Osteoporosis is typically caused by an increased stochastic bone remodelling to
meet the needs of plasma calcium homeostasis. This
will affect the bone strength through loss of bone mass
because of trabecular penetration. The bone is thereby
left weakened and at increased fracture risk. The calcium
homeostasis is influenced by several factors, and some
of these, including vitamin-D deficiency, may negatively
influence bone metabolism and thereby increase the risk
for developing osteoporosis. Another predisposing factor
for osteoporosis is inactivity. The body is programmed to
remodel bone to strengthen the weight bearing bones and
shed “unused” bone. If the bone is overused, microdamage
will occur due to remodelling. Likewise, microdamage will
also occur when bone is shed due to inactivity. Activity is
therefore essential in osteoporosis prophylaxis [3].
In keeping with this, CP patients have several potential
risk factors for osteoporosis and population based studies
have shown that there is an increased incidence of low
energy fractures in CP patients compared to matched
control groups [3, 4].
Albeit the increased risk of low energy fractures is
well established at the population level, the contributing
risk factors and their interaction are still incompletely
understood at the individual patient level. Hence, most
previous studies have mainly focused on EPI as a risk
factor for osteoporosis in the context of CP and there has
been a relative disregard of other potential risk factors
such as excessive alcohol consumption, low body weight,
steroid use, endocrine insufficiency, and muscle strength
and function [5, 6, 7, 8, 9, 10, 11].
Based on this lack of information we investigated the
association between osteoporosis and several potential
risk factors in a population of well-characterized Danish
CP outpatients. We hypothesized that a low bone mass
density (BMD) would be associated with a number of
predefined risk factors including EPI and D-vitamin
deficiency. The aim of the study was to identify risk factors
associated with decreased BMD.
METHODS
Study Design, Patients, and Normative Data
This was a cross-sectional study conducted at Centre
for Pancreatic Diseases, Department of Gastroenterology
and Hepatology, Aalborg University Hospital, Denmark
from December 2011 through August 2015. All patients
with CP referred to our specialised tertiary centre who
had a recent Dual-energy X-ray Absorptiometry (DXA)
scan (≤12 months) were included. The diagnosis of CP was
based on the Lüneburg criteria and CP was defined as a
score ≥4 points [12].
The prevalence of osteoporosis in patients with CP was
compared to age and gender-matched population derived
normative data from Danish citizens as described earlier
by Vestergaard et al. [13].
Study Outcomes
The primary outcome was to identify risk factors
associated with a low BMD in chronic pancreatitis.
Data Collection and Risk Factors for low BMD
Predefined risk factors for low BMD (see below),
demographics, clinical characteristics, and medication
were collected at the patients’ first visit in our outpatient
clinic. The M-ANNHEIM classification system was used to
categorise the aetiology of CP [14].
A number of risk factors that have previously been
associated with a low BMD were collected. These were;
gender, age, alcohol consumption [15], smoking [16, 17],
vitamin-D levels, and EPI [5, 6, 7, 9, 18, 19], opioid treatment
[20], diabetes [21, 22], malnutrition (BMI<18.5 kg/m2) [23, 24], and muscle strength and function assessed by handgrip
strength (HGS) and Timed Up and Go Test (TUG) [25].
Alcohol consumption was defined as excessive if it
exceeded the Danish Health Authorities’ recommendations
of a maximum 7 units of alcohol per week for women and
14 units of alcohol per week for men. Tobacco use was
specified as number of cigarette packs per day. Opioid use was arbitrary stratified into three groups; no opioids, opioids
use <50 morphine milligram equivalents per day, and opioid
use ≥50 morphine milligram equivalents per day.
Anthropometric Assessment
Body weight was measured to nearest 0.1 kg using
a digital electronic weight (Seca 701, CE0108, Seca,
Birmingham, United Kingdom). Height was measured to
nearest 0.1 cm using a wall-mounted stadiometer (Seca
222, CE0123, Seca, Birmingham, United Kingdom). Body
mass index (BMI) was calculated as measured body weight
in kilograms divided by height in meters squared (kg/m2).
Muscle Strength and Function
The HGS was used to estimate the muscle strength. It
was measured to the nearest kg using a hydraulic hand
dynamometer (NC70142, North Coast Medical, Arcata, CA,
USA). The patient was sitting on a chair with the shoulder
neutrally rotated, the elbow bend 90º, the wrist in neutral
position, and the dynamometer in second handle position.
HGS was measured 3 times with intervals of 10-15 seconds.
For statistical analysis, the average HGS of the two hands’
highest recordings was used [25].
The TUG was used to assess the patient’s muscle
function and mobility. It measures the time that a person
takes to rise from a chair, walk three meters, turn around,
walk back to the chair, and sit down. The TUG test provides
a composite measure of muscle function, requires both
static and dynamic balance, and has been validated in
various patient groups [26].
Dual-energy X-ray Absorptiometry
BMD (g/cm2) for the lumbar spine (L1-L4) and right
femoral neck were assessed using dual-energy X-ray
absorptiometry (Hologic Discovery DXA-scanner, Hologic
Inc., Marlborough, MA, USA). BMD was expressed as
T-scores, as well as age- and sex-adjusted Z-scores based
on the manufacturers reference material. Osteoporosis was
defined according to the World Health Organization as a
T-score ≤2.5 SD below the young adult mean and osteopenia
was defined as a T-score between -1.0 SD and -2.5 SD below
the young adult mean [27]. A daily quality control program
was employed to ensure scanner reliability and coefficient of
variations between days were <1%.
Statistical Analysis
Results are presented as means ±SD unless otherwise
stated. Normality was checked through inspection of QQplots.
The prevalence of osteoporosis was compared to
age and gender matched normative data from a population
of Danish citizens [13] and prevalence estimates were
reported as population proportions with odds ratios (OR)
and 95% confidence intervals (CI). Associations between
BMD and risk factors were analysed using univariate and
multivariate regression analysis with backward stepwise
elimination. Bootstrapping based on 5000 samples was
used for internal validation of the multivariate estimates.
To aid in interpretation of the retrieved findings, ordinal
logistic regression was used to generate probability plots illustrating the probability of having osteoporosis or
osteopenia as a function of BMI and TUG. A p-value <0.05
was considered significant. The software package STATA
version 14.2 (StataCorp LP, College Station, TX) was used
for the statistical analysis.
RESULTS
Patient Characteristics
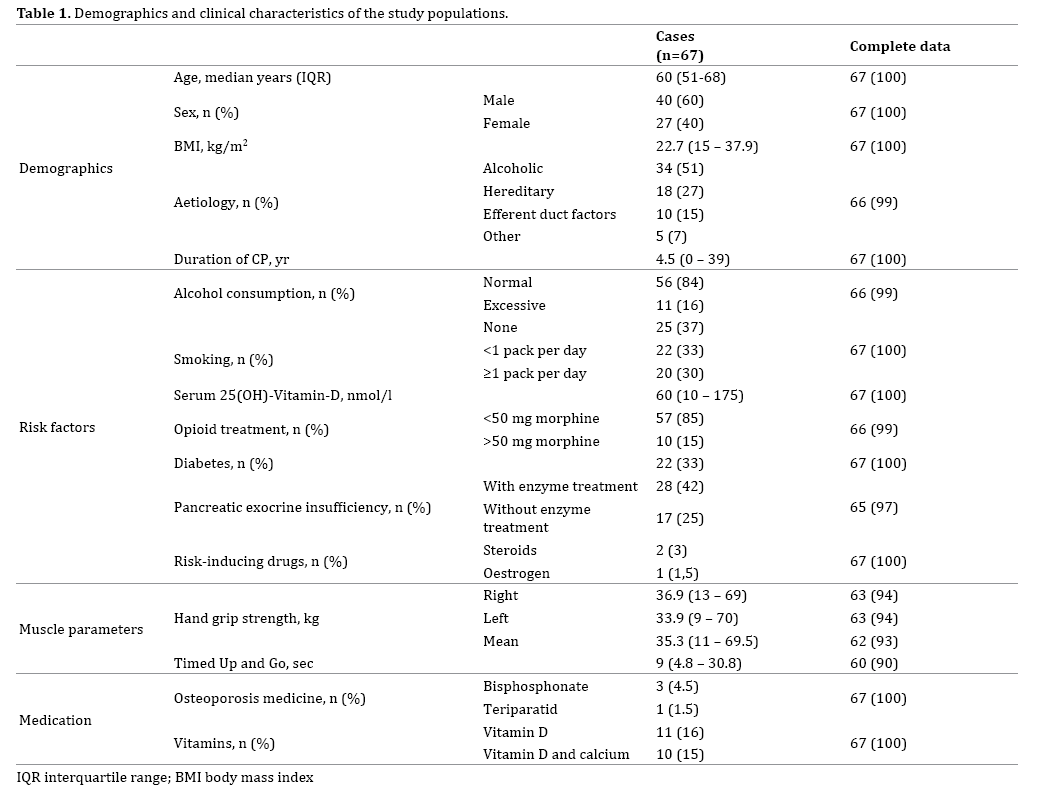
A total of 67 patients were included. The median age was
60 years (IQR 51-68) and 40 % were women. Table 1 reports
demographics and clinical characteristics for all patients.
Prevalence of Osteoporosis and Osteopenia
The prevalence of osteoporosis (combined estimate for
femoral neck and lumbar spine) in this patient group was 26.9
% in patients with CP compared to 9.1% in the population
of Danish citizens (OR 2.4 [95% CI; 1.0-5.7]; P=0.042). The
prevalence of osteoporosis for the femoral neck was 18.5 %
in CP compared to 7.3% in the Danish normative population
(OR 2.7 [95% CI; 0.9-8.2]; P=0.058); for the columnar spine,
the estimates were 16.9% and 4.7 % respectively (OR 4.2
[95% CI; 1.1-15.9]; P=0.022) (Figure 1). The prevalence of
osteoporosis for the femoral neck (18.5%) was comparable
to that observed for the columnar spine (16.9%) (P=0.82).
Figure 1: Prevalence of osteoporosis.
The prevalence of osteopenia (combined estimate for
femoral neck and lumbar spine) was 50.2 % in patients
with CP; no estimates were available for osteopenia from
the normative database.
Risk Factors Associated with Bone Mineral Density
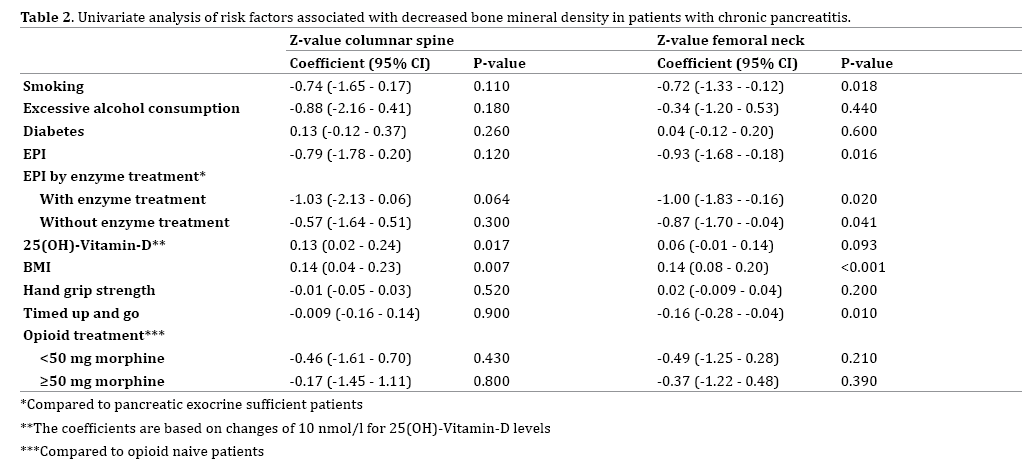
On univariate analysis two risk factors were associated
with BMD in the columnar spine; vitamin-D level
(coefficient 0.13 g/cm2; P=0.017) and BMI (coefficient 0.14
g/cm2; P=0.007). For the femoral neck four risk factors
were associated with BMD on univariate analysis; smoking
(coefficient -0.72 g/cm2; P=0.018), EPI (coefficient -0.93 g/
cm2; P=0.016), BMI (coefficient 0.14 g/cm2; P<0.001), and
TUG (coefficient (-0.16 g/cm2; P=0.01) (Table 2).
On multivariate analysis, diabetes (coefficient 0.96;
P=0.03) and EPI (coefficient -1.07; P=0.006) were
independently associated with BMD in the columnar spine,
while TUG (coefficient -.17; P<0.001), 25(OH)-Vitamin-D
level (0.13; P<0.001), and BMI (coefficient 0.14; P<0.001)
were independently associated with BMD at the femoral
neck (Table 3).
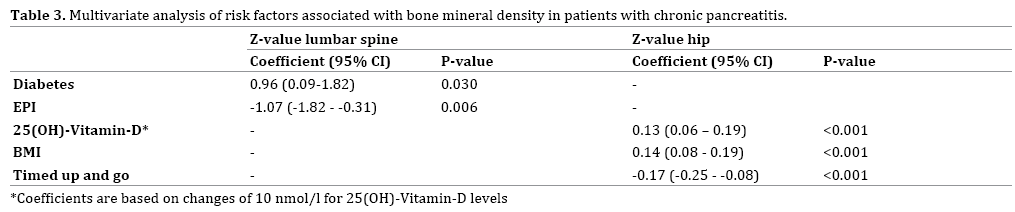
Figure 2a illustrates the risk of osteopenia and
osteoporosis as a function of BMI and TUG. A low BMI and
a prolonged time to complete the TUG were associated
with an increased risk of osteoporosis (Figure 2b).
Figure 2: (a). The risk of osteopenia and osteoporosis as a function of BMI and TUG, (b). The TUG was associated with an increased risk of osteoporosis.
DISCUSSION
We investigated the prevalence of osteoporosis and
associated risk factors in patients with CP at a tertiary
referral centre in Denmark. The patients had an increased
risk of osteoporosis compared to an age- and gender
matched normative population. Diabetes, EPI, low vitamin-D,
low BMI, and impaired muscle function (prolonged Timed Up
and Go test) were independently associated with decreased
bone mineral density. Our findings underline the importance
of systematic evaluation of bone-health in patients with CP
even in the absence of EPI.
Prevalence of Osteoporosis
We found a more than twofold increased prevalence
of osteoporosis in patients compared to the reference
population. Previous studies have reported highly varying
prevalence of osteoporosis in CP ranging from 6.7% to 34%
[5, 6, 7, 8, 11]. These variations likely reflect differences
in study populations including different age and gender
distributions, as well as differences in aetiology, severity,
duration of CP, and differences in sun exposure. The
relatively high prevalence observed in our study may be
explained by referral bias as patients were not consecutive and that they were seen at a tertiary centre and thus it is
likely that they comprised a cohort of CP patients with
more advanced disease stages than observed in primary
care or less specialised hospital facilities.
Risk factors for Osteoporosis
Our findings show that different risk factors besides
EPI are associated with low BDM. As in several other
studies, we found that EPI and low vitamin-D status were
associated with a decreased BMD. EPI is present in many
patients with CP and in the absence of appropriate enzyme
replacement therapy; it may lead to malabsorption of
fat and fat-soluble vitamins, including vitamin-D. The
latter is an essential hormone for the control of intestinal
absorption of calcium and bone mineralization and, as
such, vitamin-D deficiency is a well-known risk factor for
osteoporosis [28].
Low BMI was independently associated with a
decreased BMD in the femoral neck, but not in the
lumbar spine. Similar observations have consistently
been reported from observational studies and metaanalyses
[22, 23, 28, 29, 30, 31]. The pathophysiological
mechanisms underlying these observations have not been
fully elucidated, but two mechanisms have been proposed:
First, individuals with a high BMI conceivable have more
adipose tissue than lean individuals and in adipose tissue
aromatization of androgens to oestrogens may contribute
to maintaining bone health by maintaining a higher level of
oestrogens [23]. Second, physical activity and mechanical
loading is essential for maintaining a normal bone health
and strength [24]. Many studies have investigated the
relationship between muscle function, muscle strength,
and BMD [32, 33]. Overall, strength training does not
affect BMD [32], whereas walking exercises significantly
increases BMD in the femoral neck, but not in the lumbar
spine [33]. Our findings are in line with these observations;
hence, muscle strength was not associated with BMD,
whereas muscle function was significantly associated with
BMD in the femoral neck, but not the lumbar spine.
Our study showed a positive association between
diabetes and BMD in the columnar spine. Previous studies
have shown similar results in both type 1 and type 2
diabetes although the fracture risk was found to be higher
in these patients than in healthy control subjects [34],
indicating that BMD might not be sufficient to evaluate
bone quality in these patients.
On univariate analysis, smoking was significantly
associated with a low BMD in the femoral neck, but the
significance was lost in multivariate modelling. There
have been several studies and meta-analysis investigating
the relationship between smoking and BMD [16, 17, 34].
Overall studies conclude that smoking is associated with a
decrease in BMD of the spine and femoral neck as well as an
increased fracture risk. Many studies explain the increased
risk of low BMD in smokers with a dose-dependent
osteoblast inhibition and/or osteoclast activation from
smoking leading to decreased osteogenesis and increased
bone resorption [16]. One study hypothesized that the
relationship between smoking and decreased BMD was
secondary to confounding risk factors, e.g. low BMI which
is frequently seen in heavy smokers [17]. This could
explain why the association between smoking and BMD
in our study was lost in the multivariate model, while BMI
remained a significant and independent risk factor for low
BMD.
Strengths and Limitations
Strength in the study is that a detailed stratification and
analysis of putative risk factors was performed and when
using the Z-score for risk factor analysis, we eliminated
the confounding effects of age and gender that may have
biased previous studies.
Some limitations to this study need to be underscored:
First, the patients were not included consecutively, and
it is therefore likely that the prevalence will differ from
that in the general CP patients. Second, the cross-sectional
nature precludes definitive causal inferences about the
relationship between osteoporosis and the reported risk factors. However, plausible biological mechanisms
exist for all the identified risk factors and these are
further substantiated by previous research concerning
osteoporosis in other patient groups. Third, the relatively
small sample size may introduce a risk of type II errors,
which are particularly pertinent for the multivariate
analysis and may explain why some risk factors did not
reach independent statistical significance. Finally, the
study was conducted at a tertiary referral centre, which
introduce a risk for selection bias, as the patient`s disease
stages in this setting may be more advanced than that
observed for the average patient with CP.
To enhance knowledge on the subject, future studies
should be performed on larger cohorts with consecutively
inclusion.
CONCLUSION
In patients with CP, low BMI and reduced muscle
function were identified as independent risk factors for
osteoporosis in addition to EPI and vitamin-D deficiency.
These findings underline the relevance of a systematic
approach to bone health evaluation in the context of
CP even in the absence of EPI. Additionally, focus on
modifiable risk factors should be prioritized including,
enzyme replacement therapy in the presence of EPI,
and maintenance of normal nutritional state, vitamin-D
supplementation, and physical activity to preserve muscle
function.
Conflict of Interest
Authors declare to have no conflict of interest.
References
- Bruno MJ, Majumder S, Chari ST. Chronic pancreatitis. Gastrointest Endosc Clin N Am 2005; 15:55–62. [PMID: 15555951]
- Rasmussen HH, Irtun Ø, Olesen SS, Drewes AM, Holst M. Nutrition in chronic pancreatitis. World J Gastroenterol 2013; 19:7267–75. [PMID: 24259957]
- Armas LAG, Recker RR. Pathophysiology of Osteoporosis. New Mechanistic Insights. Endocrinol Metab Clin North Am 2012; 41:475–86. [PMID: 22877425]
- Tignor AS, Wu BU, Whitlock TL, Lopez R, Repas K, Banks PA, et al. High prevalence of low-trauma fracture in chronic pancreatitis. Am J Gastroenterol 2010; 105:2680–6. [PMID: 20736937]
- Bang UC, Benfield T, Bendtsen F, Hyldstrup L, Beck Jensen JE. The risk of fractures among patients with cirrhosis or chronic pancreatitis. Clin Gastroenterol Hepatol 2014; 12:320–6. [PMID: 23644391]
- Dujsikova H, Dite P, Tomandl J, Sevcikova A, Precechtelova M. Occurrence of metabolic osteopathy in patients with chronic pancreatitis. Pancreatology 2008; 8:583–6. [PMID: 18824882]
- Prabhakaran A, Bhasin DK, Rana SS, Bhadada SK, Bhansali A, Rao C, et al. Bone mineral metabolism and bone mineral density in alcohol related and idiopathic chronic pancreatitis. Trop Gastroenterol 2014; 35:107–12. [PMID: 25470873]
- Haas S, Krins S, Knauerhase A, Löhr M. Altered bone metabolism and bone density in patients with chronic pancreatitis and pancreatic exocrine insufficiency. JOP 2015; 16:58–62. [PMID: 25640785]
- Joshi A, Reddy SVB, Bhatia V, Choudhuri G, Singh RK, Singh N, et al. High prevalence of low bone mineral density in patients with tropical calcific pancreatitis. Pancreas 2011; 40:762–7. [PMID: 21441842]
- Haaber a B, Rosenfalck a M, Hansen B, Hilsted J, Larsen S. Bone mineral metabolism, bone mineral density, and body composition in patients with chronic pancreatitis and pancreatic exocrine insufficiency. Int J Pancreatol 2000; 27:21–7. [PMID: 10811020]
- Sikkens ECM, Cahen DL, Koch AD, Braat H, Poley JW, Kuipers EJ, et al. The prevalence of fat-soluble vitamin deficiencies and a decreased bone mass in patients with chronic pancreatitis. Pancreatology 2013; 13:238–42. [PMID: 23719594]
- Lankisch PG, Breuer N, Bruns A, Weber-Dany B, Lowenfels AB, Maisonneuve P. Natural history of acute pancreatitis: a long-term population-based study. Am J Gastroenterol 2009; 104:2797–805; quiz 2806. [PMID: 19603011]
- Vestergaard P, Rejnmark L, Mosekilde L. Osteoporosis is markedly underdiagnosed: a nationwide study from Denmark. Osteoporos Int 2005; 16:134–41. [PMID: 15197546]
- Schneider A, Löhr JM, Singer M V. The M-ANNHEIM classification of chronic pancreatitis: Introduction of a unifying classification system based on a review of previous classifications of the disease. J Gastroenterol 2007; 42:101–19. [PMID: 17351799]
- Seo S, Chun S, Newell MA, Yun M. Association between alcohol consumption and Korean young women’s bone health: a cross sectional study from the 2008 to 2011. Korea National Health and Nutrition Examination Survey. BMJ Open 2015; 5:e007914. [PMID: 26463219]
- Porter SE, Hanley EN. The musculoskeletal effects of smoking. J Am Acad Orthop Surg 2013; 9:9–17. [PMID: 11174159]
- Øyen J, Gram Gjesdal C, Nygård OK, Lie SA, Meyer HE, Apalset EM, et al. Smoking 15 and body fat mass in relation to bone mineral density and hip fracture: the Hordaland Health Study. PLoS One 2014; 9:e92882. [PMID: 24667849]
- Duggan SN, Smyth ND, Murphy A, Macnaughton D, O’Keefe SJD, Conlon KC. High prevalence of osteoporosis in patients with chronic pancreatitis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2014; 12:219–28. [PMID: 23856359]
- Vestergaard P, Rejnmark L, Mosekilde L. Fracture risk associated with the use of morphine and opiates. J Intern Med 2006; 260:76–87. [PMID: 16789982]
- Saito M, Kida Y, Kato S, Marumo K. Diabetes, collagen, and bone quality. Curr Osteoporos Rep 2014; 12:181–8. [PMID: 24623537]
- Starup-Linde J, Eriksen SA, Lykkeboe S, Handberg A, Vestergaard P. Biochemical markers of bone turnover in diabetes patients - A meta-analysis, and a methodological study on the effects of glucose on bone markers. Osteoporos Int 2014; 25:1697–708. [PMID: 24676844]
- Reid IR. Relationships between fat and bone. Osteoporos Int 2008; 19:595–606. [PMID: 17965817]
- Reid IR. Relationships among body mass, its components, and bone. Bone 2002; 31:547–55. [PMID: 12477567]
- Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991; 39:142–8. [PMID: 1991946]
- Stark T, Walker B, Phillips JK, Fejer R, Beck R. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PM R 2011; 3:472–9. [PMID: 21570036]
- Herman T, Giladi N, Hausdorff JM. Properties of the “Timed Up and Go” test: More 16 than meets the eye. Gerontology 2011; 57:203–10. [PMID: 20484884]
- Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser 1994; 843:1–129. [PMID: 7941614]
- Duggan SN, O’Sullivan M, Hamilton S, Feehan SM, Ridgway PF, Conlon KC. Patients with chronic pancreatitis are at increased risk for osteoporosis. Pancreas 2012; 41:1119–24. [PMID: 22836855]
- Lips P, van Schoor NM. The effect of vitamin D on bone and osteoporosis. Best Pract Res Clin Endocrinol Metab 2011; 25:585–91. [PMID: 21872800]
- Johansson H, Kanis JA, Odén A, McCloskey E, Chapurlat RD, Christiansen C, et al. A meta-analysis of the association of fracture risk and body mass index in women. J Bone Miner Res 2014; 29:223–33. [PMID: 23775829]
- Gray M, Di Brezzo R, Fort IL. The effects of power and strength training on bone mineral density in premenopausal women. J Sports Med Phys Fitness 2013; 53:428–36. [PMID: 23828291]
- Martyn-St James M, Carroll S. Meta-analysis of walking for preservation of bone mineral density in postmenopausal women. Bone 2008; 43:521–31. [PMID: 18602880]
- Saller A, Maggi S, Romanato G, Tonin P, Crepaldi G. Diabetes and osteoporosis. Aging Clin Exp Res 2008; 20:280-9. [PMID: 18852539]
- Ward KD, Klesges RC. A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcif Tissue Int 2001; 68:259–70. [PMID: 11683532]



