Keywords
Cholangiopancreatography, Endoscopic Retrograde; Pancreas, /abnormalities; Pancreatitis, /etiology, /prevention and control, /therapy; Recurrence, /prevention and control; Sphincterotomy, Endoscopic; Treatment Outcome
Abbreviations
CAP: chronic abdominal pain without associated pancreatic enzyme elevations; EMP: endoscopic minor papillotomy; RP: recurrent acute pancreatitis; RP+CAP: pancreatitis with continuous pain or incomplete relief between bout
INTRODUCTION
A minority of patients with pancreas divisum becomes symptomatic with recurrent acute pancreatitis [1, 2, 3, 4, 5, 6, 7], chronic pancreatitis [8, 9, 10], or chronic abdominal pain without evidence of pancreatitis [11]. The underlying mechanism in these cases is thought to be a relative outflow obstruction at the site of the minor papilla due to a true or relative stenosis. The finding of chronic obstructive changes confined to the dorsal pancreatic duct supports this hypothesis [8, 12, 13, 14]. Surgical sphincteroplasty [15, 16, 17] as well as endoscopic interventions such as endoscopic minor papillotomy (EMP) [18, 19, 20, 21, 22], insertion of dorsal duct stents [23, 24, 25], dilation [26, 27] and injection of botulinum toxin into the minor papilla [28] have been applied with variable success in symptomatic patients. Currently it is difficult to reliably select patients who will benefit from endoscopic therapy, and data about long-time results after EMP are lacking. We wish to report our personal experience of a large series of EMP for pancreas divisum.
MATERIAL AND METHODS
Patients
The endoscopic database of the Duke University Medical Center was searched for patients who underwent EMP for symptomatic pancreas divisum between June, 1993, and March, 2001. EMP was performed with either a needle knife over a previously placed dorsal pancreatic duct stent (as described elsewhere [29, 30]) or with a conventional Erlangen-type (“pull”) sphincterotome and subsequent placement of 3 or 5 French stents into the minor pancreatic duct to protect against early scarring and obstruction by edema. Pure cutting current was used. Stents were typically removed within 2-4 weeks to avoid stent-induced damage to the pancreatic duct. Patients with pancreatic resection prior to or within 2 weeks after EMP (n=2) and those who were less than 18 years at the time of follow-up (n=1) were excluded. Eighty-nine patients were included in the study. The median age at the time of EMP was 49 years (range: 17-78 years); 31 patients (34.8%) were male and 58 (65.2%) were female.
The ERCP reports of the 89 patients included in the study were retrospectively reviewed. Irregularities or dilatations of the pancreatic ductal system were reported in 61 patients (68.5%).
Follow-up Study
For patients who met the study inclusion criteria, a registered nurse or physician conducted a telephone interview using a questionnaire. Thirty-three patients had moved, leaving no forwarding addresses or telephone number, two patients refused to participate and one patient was not competent to answer the questionnaire and was therefore excluded. Thus, 53 patients (59.6%) were available for follow-up. The median age at the time of EMP was 50 years (range: 17-78 years; P=0.377 vs. the 36 excluded patients); 19 patients (35.8%) were male and 34 (64.2%) were female (P=0.825 vs. the 36 excluded patients). Median follow-up was 29 months (range: 13-91 months).
Symptoms
Symptoms before and after EMP were recorded at the telephone interview. Patients were grouped into those with recurrent acute pancreatitis (n=30; 56.6%), those with pancreatitis and continuous pain or incomplete relief between bouts (n=14; 26.4%) and those with chronic abdominal pain but no evidence of pancreatitis (n=9; 17.0%). Relief of symptoms after EMP was considered “immediate improvement”. Patients with no symptoms or minimal symptoms (less or equal to 2 on a VAS scale from 0 to 10) after EMP and no recurrence of symptoms were considered as having “longterm improvement”. Those who had recurrent symptoms which resolved with repeat EMP were also considered as having “long-term improvement”.
STATISTICS
Contingency tables were analyzed by means of the Fisher's exact test (2x2 tables) or the hierarchical log-linear models. Age was analyzed by means of the Student's t-test. Two-tailed P values less than 0.05 were considered statistically significant. Statistical analysis was performed by running the SPSS 8.0 for Windows.
ETHICS
The study was approved by the Duke University Medical Center Institutional Review Board.
RESULTS
Complications
Post-ERCP pancreatitis occurred in 10 of the 89 patients included in the study (11.2%). The pancreatitis was “mild” in 6 and “moderate” in 4 patients, according to a commonly used grading system [31]. In one of those patients, the pancreatitis was felt to be due to pancreatic stent occlusion one week after minor papillotomy. In another, it was related to proximal stent migration. A 54 year old female patient died during follow up. She underwent EMP for pancreatitis and continuous abdominal pain (RP+CAP). Repeat ERCP with pancreatic duct stenting resulted in transient improvements of her symptoms. She finally underwent pancreaticoduodenectomy (Whipple procedure) for chronic pancreatitis. The operation was complicated by small bowel necrosis and sepsis, which led to multiple reoperations and long term hospitalization. The patient died 3 years after the initial EMP and one year after surgery.
A stricture developed in the pancreatic neck of a 45 year old woman in whom a 5 French, 5 cm pancreatic stent was left in place for 6 weeks after EMP. She became free of symptoms after stent removal and endoscopic stricture dilation.
Stenting of the Dorsal Pancreatic Duct prior to EMP
Six patients had trials of dorsal duct stents prior to EMP: two developed pancreatic duct strictures which were thought likely to be stent induced. The first patient was a 40 year old woman with a history of pancreatitis and chronic abdominal pain (RP+CAP). She responded well to a one month trial of a 5 French, 3 cm stent and subsequent EMP. Her symptoms recurred after 6 months. At that time, a mild-to-moderate stricture in the pancreatic head was demonstrated by ERCP. Endoscopic stricture dilation resulted in transient improvement of her symptoms only. The patient underwent surgical sphincteroplasty without lasting benefit. Finally, a lateral pancreaticojejunostomy (Puestow procedure) was performed. She continued to have pain requiring narcotic analgesia.
The second patient was a 60 year old man with recurrent bouts of pancreatitis and radiographic findings consistent with chronic pancreatitis. He underwent repeated stenting of the dorsal pancreatic duct with 5 French, 3 cm stents over a three year period. During that time, a stricture developed in the head of the pancreas, with “upstream” ductal dilatation. It was not clear if the stricture was the result of chronic pancreatitis or induced by pancreatic duct stenting. The patient responded well to EMP, endoscopic stricture dilation and short term stenting, but his symptoms recurred after 8 months. 6 years after the initial EMP, he finally underwent a Puestow-procedure with a favorable response.
Response to EMP
The outcome after EMP is summarized in Figure 1. Thirty-two out of 53 patients (60.4%) had immediate improvement after minor papillotomy; 21 patients did not. Of the 32 patients with immediate response, pain recurred in 17 (53.1% of the immediate responders) after a median of 6 months (range: 1-24 months). Of the 17 patients with recurrent symptoms, repeat endoscopic interventions were performed in 8 (EMP in 7 patients, pancreatic stent removal and dilation of a stent induced stricture in 1 patient), with long-term improvement in 2 patients. Summarizing these data: 17 (32.1%) patients had long term improvement (15 had no recurrence and 2 required a second endoscopic intervention) and 36 (67.9%) patients had no long-term improvement (21 had no initial improvement, 15 had recurrence).
Figure 1. Outcome after endoscopic minor
papillotomy.
Nine patients underwent pancreatic surgery during follow-up: one underwent both major and minor surgical sphincteroplasty, one had a pancreatic tail resection; a cystojejunostomy was performed in 2 and a pancreaticojejunostomy in 5 patients, one of whom had recurrent symptoms after sphincteroplasty of the minor papilla; in 3 of these patients, pancreaticojejunostomy was combined with a partial pancreatic resection.
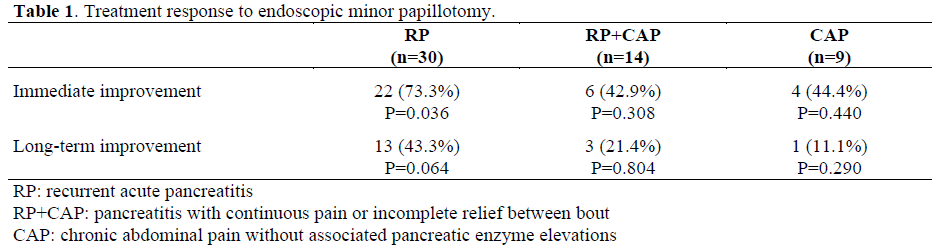
The response to EMP for the different groups are summarized in Table 1. Patients with well defined bouts of pancreatitis (RP) had significantly (P=0.036) better immediate improvement than those with pancreatitis who reported continuous pain or incomplete relief between bouts (RP+CAP) and those with chronic abdominal pain without clinical evidence of pancreatitis (CAP) (immediate improvement: 73.3%, 42.9% and 44.4%, respectively; long-term-improvement: 43.3%, 21.4% and 11.1%, respectively).
Thirty-six (67.9%) of the follow-up patients had irregularities within the dorsal ductal system while 17 (32.1%) had normal dorsal ducts. There was a non-significant trend towards better outcome for patients with regular and nondilated dorsal pancreatic ducts vs. irregular/dilated dorsal duct (immediate improvement: 76.5% vs. 52.8%, P=0.137; long-term-improvement: 41.2% versus 27.8%, P=0.360; Table 2). Differences in the clinical presentation prior to EMP were small between these groups: RP 11/17 (64.7%) vs. 19/36 (52.8%), P=0.529; RP+CAP 2/17 (11.8%) vs. 12/36 (33.3%), P=0.113; CAP 4/17 (23.5%) vs. 5/36 (13.9%), P=0.245; regular dorsal duct vs. irregular/dilated dorsal duct, respectively.

DISCUSSION
The prevalence of pancreas divisum in patients who undergo ERCP is about 4-8% in Western populations and less than 2% in Asians [2, 6, 8, 14, 32, 33, 34, 35, 36]. In most patients, pancreas divisum is an incidental finding; only a small subset of these patients develops symptoms. It has been postulated that minor papilla stenosis is a necessary predisposing factor in the evolution of symptomatic disease [4, 11, 16]. Therapeutic interventions aim to relieve the obstruction by improving pancreatic drainage via the minor papilla. Surgical sphincteroplasty has been shown to be effective [4, 5, 7, 15, 16, 17, 37, 38, 39, 40, 41]. Endoscopic interventions such as minor papillotomy or dilation and subsequent dorsal duct stent placement provide less invasive alternatives. EMP was first described in 1978 [42]. This has been followed by several series of endoscopic interventions such as EMP, dorsal pancreatic duct stenting or dilation, with results comparable to surgical sphincteroplasty. The only randomized controlled trial of endoscopic therapy for pancreas divisum was reported by Lans et al. [23]: 19 patients with pancreas divisum and recurrent acute pancreatitis were randomized to dorsal duct stent placement or no treatment. Symptomatic improvement was observed in 90% of patients in the stent-group versus 11% of the controls. The study shows a statistically significant benefit of dorsal duct stenting but is clearly limited by the very small number of patients included.
In the present study, 60% of patients reported improvement after EMP; however, symptoms recurred in about one half of these cases. It is doubtful that patients with transient improvement are true responders to EMP. Since there were no controls with sham procedure, a placebo effect cannot be ruled out in these patients. Furthermore, in patients with acute recurrent pancreatitis, it is impossible to reliably define short term improvement. These patients might have experienced a symptom-free interval anyway, regardless of the endoscopic intervention. However, 8 out of 16 patients with recurrent symptoms had sustained improvement for 6 months or longer. It is natural to suspect restenosis of the papillotomy site in these patients; restenosis is common both after surgical sphincteroplasty and EMP. In a series by Warshaw et al. [16], restenosis occurred in 7 out of 88 patients (8%) after surgical sphincteroplasty. In these patients, repeat sphincteroplasty can be technically difficult. The frequency of restenosis after EMP was estimated at 19% by Lehman et al. [19], and at 11.5% by Kozarek et al. [20]. In the present study, repeat endoscopic interventions for recurrent symptoms were performed in 8 patients, with favorable long-term response in only two. Three of the 6 patients who failed to improve after repeat endoscopic treatment improved after surgery (data not shown): sphincteroplasty of the major and minor papilla in one and lateral pancreatojejunostomy (Puestow) in 2, one of which was preceded by sphincteroplasty of the minor papilla with recurrence of symptoms. We conclude that an attempt at repeat endoscopic therapy is justified in patients with recurrent symptoms. However, patients with ongoing of symptoms often require surgical sphincteroplasty or a surgical drainage procedure. Given that the results of surgical sphincteroplasty are no better than for endoscopic papillotomy, surgeons are increasingly recommending pancreatojejunostomy for patients who fail endoscopic therapy if the dorsal pancreatic duct is dilated. In the present series, which, to the best of out knowledge, is the largest in the literature, long-term response to EMP using strict criteria was only 33%. Previous data suggest a much less favorable outcome for patients with chronic pancreatitis or pain alone than for those with acute recurrent pancreatitis [2, 7, 11, 19, 20, 43, 44]. Our data are in agreement with this. We grouped the patients according to their clinical presentation. Patients with well defined bouts of recurrent acute pancreatitis had significantly higher response rates to EMP than those with pancreatitis and continuous pain, and those with pain alone. However, even for the patients with recurrent acute pancreatitis the results were sobering, less than half were free of symptoms at follow up. This is a poorer result than previously reported (Table 3). This might be explained partially by chronic pancreatic damage that is not reversible by EMP. Sixty-nine percent of the patients included in the present study had radiographic changes in the dorsal pancreatic ductal system, such as strictures or dilatation. Other authors report radiographic evidence of ductal changes consistent with chronic disease in 30- 57% of patients with pancreas divisum [8, 14, 27]. In symptomatic patients, the chronic component likely limits the success of endoscopic or surgical interventions at the minor papilla.

The present study suggests that EMP has an acceptable complication rate: mild or moderate post-procedure pancreatitis was observed in 11% of patients. We accept that this might be an underestimate due to the retrospective design of the study. Lehman et al. reported a similar pancreatitis rate of 13% [19]; however, rates of up to 70% have been reported [30].
In our experience, prolonged stenting of the dorsal pancreatic duct should be avoided because of the risk of inducing pancreatic damage [45, 46]. Radiographic changes affecting the dorsal pancreatic duct occur in 26-89% of patients after prolonged stenting [20, 24, 47, 48, 49, 50]. In the present study, 2 out of 6 patients who underwent prolonged stent treatment prior to EMP, and another patient, in whom a pancreatic stent was left in place for 6 weeks after EMP, developed pancreatic duct strictures. Stent occlusion carries the risk of acute pancreatitis [51] and sepsis [43]. Two out of the 89 patients included in the present study who underwent EMP and placement of a dorsal duct stent developed pancreatitis due to early stent occlusion or proximal stent migration. At our institution, dorsal duct stents are placed after EMP to prevent obstruction secondary to edema and early restenosis. Our policy is to remove the stents within 2-4 weeks if they have not migrated into the duodenal lumen by then.
The limited long-term response to endoscopic interventions emphasizes the importance of selecting patients who are likely to have a favorable outcome. Especially for patients who do not present with well defined bouts of pancreatitis, non-invasive tests to predict the outcome of endoscopic or surgical interventions are desirable. Secretin ultrasound studies have been used for this purpose. In experienced hands, complete imaging of the pancreas with transabdominal ultrasound is possible in 75-90% of cases [52, 53, 54]. A secretin ultrasound test is considered pathologic and indicative of true or relative minor papillary stenosis if prolonged dilatation of the pancreatic duct is observed after intravenous secretin. In a study by Warshaw et al., a positive secretin ultrasound test predicted a positive outcome after surgical sphincteroplasty in 92% of patients with recurrent pancreatitis and chronic pain [16]; the negative predictive value of this test was reported as 75-80% [15]. Despite these promising results, secretin ultrasound has not gained wide acceptance in clinical practice. Secretin is expensive, and until recently has not been widely available for routine use. With the recent FDA approval of synthetic porcine secretin, it may be worthwhile to reevaluate secretin ultrasound. Secretin stimulated magnetic resonance cholangiopancreatography [55] may prove to be an alternative, but has not been evaluated for this purpose so far. Endoscopic dorsal duct stenting has been suggested as a therapeutic trial prior to surgical sphincteroplasty [21, 56, 57]. Siegel et al. [57] reported a favorable outcome after surgery in 10 of 15 patients who had improved with stenting, but in only one of 5 patients who had not improved with stents. However; the study was limited by the small numbers and failure to demonstrate statistical significance. As discussed above, a negative of endoscopic dorsal duct stenting is the high risk of inducing ductal disease.
The results of the present study confirm that, amongst patients with symptomatic pancreas divisum, those with acute recurrent pancreatitis have the most favorable outcome after EMP. In patients with recurrent symptoms after initial response repeat endoscopic treatment can be attempted; however, surgical interventions may eventually be required. Prolonged stenting of the dorsal pancreatic duct can induce irreversible ductal damage and should therefore be avoided. The low overall longterm response to EMP underlines the need for better tests to select patients who are likely to benefit from endoscopic therapy.
References
- Buhler H, Seefeld U, Deyhle P, Largiader F, Ammann R. Clinical significance of pancreas divisum. Schweiz Med Wochenschr 1983; 113:320-4. [PMID 6189182]
- Brenner P, Duncombe V ,Ham JM. Pancreatitis and pancreas divisum: aetiological and surgical considerations. Aust N Z J Surg 1990; 60:899-903. [PMID 2241651]
- Cotton PB. Pancreas divisum--curiosity or culprit? Gastroenterology 1985; 89:1431-5. [PMID 4054536]
- Warshaw AL, Richter JM ,Schapiro RH. The cause and treatment of pancreatitis associated with pancreas divisum. Ann Surg 1983; 198:443-52. [PMID 6625715]
- Keith RG, Shapero TF ,Saibil FG. Treatment of pancreatitis associated with pancreas divisum by dorsal duct sphincterotomy alone. Can J Surg 1982; 25:622-6. [PMID 7139415]
- Bernard JP, Sahel J, Giovannini M ,Sarles H. Pancreas divisum is a probable cause of acute pancreatitis: a report of 137 cases. Pancreas 1990; 5:248-54. [PMID 2343039]
- Richter JM, Schapiro RH, Mulley AG ,Warshaw AL. Association of pancreas divisum and pancreatitis, and its treatment by sphincteroplasty of the accessory ampulla. Gastroenterology 1981; 81:1104-10. [PMID 7286588]
- Morgan DE, Logan K, Baron TH, Koehler RE ,Smith JK. Pancreas divisum: implications for diagnostic and therapeutic pancreatography. AJR Am J Roentgenol 1999; 173:193-8. [PMID 10397125]
- Lu WF. ERCP and CT diagnosis of pancreas divisum and its relation to etiology of chronic pancreatitis. World J Gastroenterol 1998; 4:150-152. [PMID 11819261]
- Wind P, Berger A, Chevallier JM, Frileux P ,Cugnenc PH. Pancreas divisum, chronic pancreatitis and diabetes mellitus. Improvement by pancreaticojejunostomy. Ann Chir 1992; 46:625-9. [PMID 1456695]
- Varshney S ,Johnson CD. Pancreas divisum. Int J Pancreatol 1999; 25:135-41. [PMID 10360226]
- Blair AJ 3rd, Russell CG, Cotton PB. Resection for pancreatitis in patients with pancreas divisum. Ann Surg 1984; 200:590-4. [PMID 6385880]
- Marshall JB ,Eckhauser ML. Pancreas divisum. A cause of chronic relapsing pancreatitis. Dig Dis Sci 1985; 30:582-7. [PMID 3996162]
- Benage D, McHenry R, Hawes RH, O'Connor KW ,Lehman GA. Minor papilla cannulation and dorsal ductography in pancreas divisum. Gastrointest Endosc 1990; 36:553-7. [PMID 2279641]
- Warshaw AL ,Schapiro RH. Pancreas divisum and pancreatitis. Surg Annu 1988; 20:101-20. [PMID 3283959]
- Warshaw AL, Simeone JF, Schapiro RH ,Flavin- Warshaw B. Evaluation and treatment of the dominant dorsal duct syndrome (pancreas divisum redefined). Am J Surg 1990; 159:59-64. [PMID 2403764]
- Lehman GA ,Sherman S. Diagnosis and therapy of pancreas divisum. Gastrointest Endosc Clin N Am 1998; 8:55-77. [PMID 9405751]
- Heyries L, Barthet M, Delvasto C, Zamora C, Bernard JP, Sahel J. Long-term results of endoscopic management of pancreas divisum with recurrent acute pancreatitis. Gastrointest Endosc 2002; 55:376-81. [PMID 11868012]
- Lehman GA, Sherman S, Nisi R ,Hawes RH. Pancreas divisum: results of minor papilla sphincterotomy. Gastrointest Endosc 1993; 39:1-8. [PMID 8454127]
- Kozarek RA, Ball TJ, Patterson DJ, Brandabur JJ, Raltz SL. Endoscopic approach to pancreas divisum. Dig Dis Sci 1995; 40:1974-81. [PMID 7555452]
- Siegel JH, Ben-Zvi JS, Pullano W ,Cooperman A. Effectiveness of endoscopic drainage for pancreas divisum: endoscopic and surgical results in 31 patients. Endoscopy 1990; 22:129-33. [PMID 2103724]
- Liguory C, Lefebvre JF, Canard JM, Bonnel D, Fritsch J, Etienne JP. Pancreas divisum: clinical andtherapeutic study in man. Apropos of 87 cases. Gastroenterol Clin Biol 1986; 10:820-5. [PMID 3803823]
- Lans JI, Geenen JE, Johanson JF, Hogan WJ. Endoscopic therapy in patients with pancreas divisum and acute pancreatitis: a prospective, randomized, controlled clinical trial. Gastrointest Endosc 1992; 38:430-4. [PMID 1511816]
- Ertan A. Long-term results after endoscopic pancreatic stent placement without pancreatic papillotomy in acute recurrent pancreatitis due to pancreas divisum. Gastrointest Endosc 2000; 52:9-14. [PMID 10882955]
- McCarthy J, Geenen JE ,Hogan WJ. Preliminary experience with endoscopic stent placement in benign pancreatic diseases. Gastrointest Endosc 1988; 34:16-8. [PMID 3350298]
- Jacob L, Geenen JE, Catalano MF, Johnson GK, Geenen DJ, Hogan WJ. Clinical presentation and shortterm outcome of endoscopic therapy of patients with symptomatic incomplete pancreas divisum. Gastrointest Endosc 1999; 49:53-7. [PMID 9869723]
- Satterfield ST, McCarthy JH, Geenen JE, Hogan WJ, Venu RP, Dodds WJ, Johnson GK. Clinical experience in 82 patients with pancreas divisum: preliminary results of manometry and endoscopic therapy. Pancreas 1988; 3:248-53. [PMID 3387418]
- Wehrmann T, Schmitt T, Seifert H. Endoscopic botulinum toxin injection into the minor papilla for treatment of idiopathic recurrent pancreatitis in patients with pancreas divisum. Gastrointest Endosc 1999; 50:545-8. [PMID 10502179]
- Siegel JH, Cohen SA, Kasmin FE, Veerappan A. Stent-guided sphincterotomy. Gastrointest Endosc 1994; 40:567-72. [PMID 7988820]
- Cohen SA, Kasmin FE, Siegel JH. Minor papilla sphincterotomy in pancreas divisum. Gastrointest Endosc 1994; 40:117-9. [PMID 8192793]
- Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991; 37:383-93. [PMID 2070995]
- Hayakawa T, Kondo T, Shibata T, Sugimoto Y, Kitagawa M, Suzuki T, et al. Pancreas divisum. A predisposing factor to pancreatitis? Int J Pancreatol 1989; 5:317-26. [PMID 2691589]
- Dhar A, Goenka MK, Kochhar R, Nagi B, Bhasin DK, Singh K. Pancreas divisum: five years' experience in a teaching hospital. Indian J Gastroenterol 1996; 15:7-9. [PMID 8840617]
- Burtin P, Person B, Charneau J, Boyer J. Pancreas divisum and pancreatitis: a coincidental association? Endoscopy 1991; 23:55-8. [PMID 2050007]
- Kim HJ, Kim MH, Lee SK, Seo DW, Kim YT, Lee DK, et al. Normal structure, variations, and anomalies of the pancreaticobiliary ducts of Koreans: a nationwide cooperative prospective study. Gastrointest Endosc 2002; 55:889-96. [PMID 12024146]
- Saowaros V. Pancreas divisum: incidence and clinical evaluation in Thai patients. J Med Assoc Thai 1992; 75:692-6. [PMID 1308537]
- Gregg JA, Monaco AP, McDermott WV. Pancreas divisum. Results of surgical intervention. Am J Surg 1983; 145:488-92. [PMID 6837884]
- Rusnak CH, Hosie RT, Kuechler PM, McHattie JD, Piercey JR ,Cameron RD. Pancreatitis associated with pancreas divisum: results of surgical intervention. Am J Surg 1988; 155:641-3. [PMID 2453123]
- Russell RC, Wong NW ,Cotton PB. Accessory sphincterotomy (endoscopic and surgical) in patients with pancreas divisum. Br J Surg 1984; 71:954-7. [PMID 6498472]
- Madura JA, Fiore AC, O'Connor KW, Lehman GA, McCammon RL. Pancreas divisum. Detection and management. Am Surg 1985; 51:353-7. [PMID 3994178]
- Cooperman M, Ferrara JJ, Fromkes JJ ,Carey LC. Surgical management of pancreas divisum. Am J Surg 1982; 143:107-12. [PMID 7053641]
- Cotton PB. Duodenoscopic papillotomy at the minor papilla for recurrent dorsal pancreatitis. Endosc Dig 1978; 3:27-8.
- Coleman SD, Eisen GM, Troughton AB ,Cotton PB. Endoscopic treatment in pancreas divisum. Am J Gastroenterol 1994; 89:1152-5. [PMID 8053426]
- Bradley EL 3rd ,Stephan RN. Accessory duct sphincteroplasty is preferred for long-term prevention of recurrent acute pancreatitis in patients with pancreas divisum. J Am Coll Surg 1996; 183:65-70. [PMID 8673310]
- Alvarez C, Robert M, Sherman S, Reber HA. Histologic changes after stenting of the pancreatic duct. Arch Surg 1994; 129:765-8. [PMID 7912922]
- Gulliver DJ, Edmunds S, Baker ME, Paine S, Baillie J, Cotton PB, Rice RP. Stent placement for benign pancreatic diseases: correlation between ERCP findings and clinical response. AJR Am J Roentgenol 1992; 159:751-5. [PMID 1529836]
- Kozarek RA. Pancreatic stents can induce ductal changes consistent with chronic pancreatitis. Gastrointest Endosc 1990; 36:93-5. [PMID 2335298]
- Siegel J ,Veerappan A. Endoscopic management of pancreatic disorders: potential risks of pancreatic prostheses. Endoscopy 1991; 23:177-80. [PMID 1860449]
- Rutkovsky FD, Cohen SA, Kasmin FE ,Siegel JH. Minor papilla sphincterotomy in pancreas divisum - complications and response. A J Gastroenterol 1992; 87:1293.
- Barkun AN, Jones S, Putnam WS, Baillie J, Parker S ,Cotton PB. Endoscopic treatment of patients with pancreas divisum and pancreatitis. Gastrointest Endosc 1990; 36:206-7.
- Okolo PI, 3rd, Pasricha PJ ,Kalloo AN. What are the long-term results of endoscopic pancreatic sphincterotomy? Gastrointest Endosc 2000; 52:15-9. [PMID 10882956]
- Reuss J ,Rettenmaier G. Transabdominal ultrasonography in pancreatic diseases. Schweiz Med Wochenschr 1993; 123:1049-58. [PMID 8511536]
- Glaser J, Hogemann B, Krummenerl T, Schneider M, Hultsch E, van Husen N, Gerlach U. Sonographic imaging of the pancreatic duct. New diagnostic possibilities using secretin stimulation. Dig Dis Sci 1987; 32:1075-81. [PMID 3308373]
- Glaser J. Clinical perspectives of a sonographic secretin test. Z Gastroenterol 1997; 35:579-83. [PMID 9273992]
- Hellerhoff KJ, Helmberger H 3rd, Rosch T, Settles MR, Link TM, Rummeny EJ. Dynamic MR pancreatography after secretin administration: image quality and diagnostic accuracy. AJR Am J Roentgenol 2002; 179:121-9. [PMID 12076919]
- Quest L ,Lombard M. Pancreas divisum: opinio divisa. Gut 2000; 47:317-9. [PMID 10940261]
- Siegel JH, Cooperman AM, Pullano W, Hammerman H. Pancreas divisum: observation, endoscopic drainage, and surgical treatment results in 65 patients. Surg Laparosc Endosc 1993; 3:281-5. [PMID 8269244]
- Soehendra N, Kempeneers I, Nam VC, Grimm H. Endoscopic dilatation and papillotomy of the accessory papilla and internal drainage in pancreas divisum. Endoscopy 1986; 18:129-32. [PMID 3732181]


