Keywords
Pancreas
INTRODUCTION
During the last decade, treatment of cystic pancreatic lesions has changed radically. Numerous guidelines have emerged to advise clinicians [1-3]. Previously, all cystic pancreatic lesions apart from pseudocysts were considered for surgery. Today consensus advocates observation in selected patients based on imaging criteria. However, management guidelines relate to specific histopathologic entities, which frequently remain unknown preoperatively [4, 5]. Recent literature has focused on the outcome of a stratified management. The international consensus working group’ recommendations, the “Sendai guidelines”, were updated in 2012, and a larger proportion of sidebranch intraductal papillary mucinous lesions (SB-IPMNs) may be considered for serial imaging, compared to the 2006 guidelines. On the other hand, in patients with small SB-IPMNs (“Sendai negative”) undergoing surgery at a large pancreatic centre in Germany, one in five cysts were found to harbour malignancy [6], highlighting the debate on indication for surgery in this setting [7, 8].
In our tertiary pancreatic centre, the threshold has been low for laparoscopic surgery in patients with distal cystic pancreatic tumours. Surgery includes both a diagnostic and for some patients a therapeutic procedure. It is important to evaluate this approach as current guidelines have limited the indication for surgery. The present investigation was initiated prior to the implementation of new guidelines for cystic pancreatic lesions. The aim was to evaluate the outcome of surgery 1997–2009 with histological diagnosis as endpoint.
METHODS
All patients undergoing laparoscopic pancreatic surgery for cystic pancreatic lesions in the distal pancreas at our tertiary centre between 1997 and 2009 were prospectively included in present study, which was approved by the local ethics committee. Patients with lesions in the pancreatic head were excluded.
Inclusion Criteria
All patients, eligible for the surgical procedure, were considered for inclusion. Indication for surgery was based on a combination radiological findings (computed tomography and magnetic resonance imaging or ultrasonography), patient symptoms and biochemical investigations for hormonally active tumours. A final diagnostic assessment concluded on what was the most likely suspected pathology. If this was a pseudocyst, secondary to pancreatitis, the patient was excluded. When the conclusion was: Most likely a cystic neoplasm in the distal pancreas, the patient was included. The present study was initiated nine years before the Sendai criteria were published [9]. At this time we considered all neoplastic lesions in the distal pancreas (location to the left of the portal vein, i.e. body and/or tail) an indication for surgery.
Based on the combined preoperative radiological and clinical data, the peroperative strategy was chosen according to the following principles: if a lesion was supposed to have a significant malignant potential, distal resection together with splenectomy was preferred. Otherwise, spleen-preserving distal pancreatic resection was chosen [10]. In the case of a small, superficial and tentatively benign lesion, i.e. with significant distance from the main pancreatic duct, enucleation was considered adequate [11]. Radiological diameter <20 mm and distance from the main pancreatic duct >3 mm were criteria for the enucleations.
Surgical Technique
Patients were operated under general anaesthesia, placed in a modified supine position with the left side raised. The first trocar was placed in the umbilicus, one additional 12 mm trocar in the midline between the xiphoid process and the umbilicus and one 12 mm trocar at the level of the umbilicus, pararectally. Occasionally an additional 5 mm trocar was placed subcostally in the medioclavicular line. Two main instruments were used to mobilize the splenic flexure of the colon medially, opening the lesser sac then dissecting the peripancreatic tissue. Also the gastrocolic ligament and the short gastric vessels were divided mobilising the transverse colon. Intraoperative ultrasound was used for exact tumour localisation. In case of spleenpreserving distal pancreatectomy, the splenic vessels were dissected from the pancreas to maintain adequate circulation of the spleen. An EndoGIA® was used to divide the pancreas, and a drain was placed at the resection margin for analysis of amylase in the secreted fluid. The surgical technique has been described in detail earlier [12].
Postoperative complications occurring in-hospital were recorded and retrospectively classified by the Revised Accordion Classification from grade 1 (mild) to 6 (death) [13]. The pancreatic fistula severity grading criteria of the ISGPF was used [14]. These criteria were published after study start, and classification was done retrospectively.
Neoplasms were categorised according to the WHO classification from 2000 [15]. However, the WHO revised its classification in 2010, and now all solid pseudopapillary neoplasms (SPPN) are categorised as low-grade malignancies [16]. Thus, SPPNs originally reported to be benign were recoded into low-grade malignancies.
Lesions were classified according to their pathological diagnosis into two groups: patients with or without malignant potential. For this reason, serous cystic neoplasms (SCN), pseudocysts, retention cysts and lymphoepithelial cysts were classified as neoplasms without malignant potential. Mucinous cystic neoplasms (MCN), SPPNs and intraductal papillary mucinous neoplasm (IPMN) were classified as tumours with malignant potential. Patients with established malignancy were included among the latter.
Statistical analysis was performed using SPSS (IBM SPSS Statistics Version 21 for Windows). Nonparametric statistical tests were used, and variables were compared using the Mann-Whitney test. Statistical significance was set at a p value less than 0.05.
RESULTS
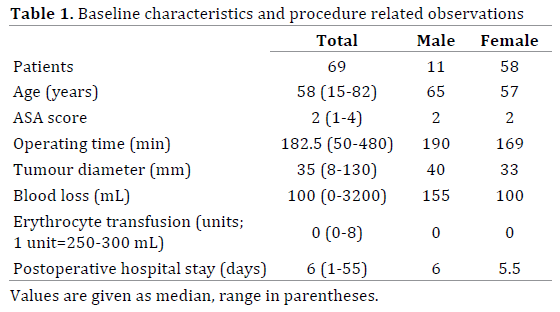
A total of 193 patients underwent resection of the body and/or tail of the pancreas by the laparoscopic approach during the study period. The indication for resection was neoplasm with uncertain malignancy potential, most often a solid tumour. In 69 patients the indication for resection was a cystic neoplastic lesion, which was the inclusion criteria in the present study, as specified above. Baseline characteristics for these 69 patients are shown in Table 1. Sixty-two patients underwent distal pancreatectomies, in whom 19 were spleen-preserving. In seven additional cases enucleations were performed. Overall operating time was median 182.5, range 50-480 minutes. Operating times with and without splenectomy were median 167 and 220 minutes, respectively (P=0.19), and median 127.5 minutes in enucleations.
Histology of the resected specimens is summarized in Table 2. Histopathologically, 57 patients (83%) had benign and 12 patients (17%) had malignant lesions, two invasive IPMNs and ten SPPNs. There were three IPMNs with moderate dysplasia. All 12 MCNs were reported as benign by the pathologists.

When the patients were grouped according to the lesions’ malignant potential, distal laparoscopic resections had been performed in 27 patients (39%) with neoplasms with malignancy or a malignant potential (Figure 1).
Figure 1. Histological diagnosis of the resected specimens
Left: Number (and proportion) of resected benign and malignant lesions
Right: Number (and proportion) of resected specimens with/without malignant potential
In two patients with IPMN the tumour diameter was less than 30 mm, both with moderate dysplasia, i.e. borderline tumours. The diameter of the tumour in the first was 29 mm; this patient had a positive family history of pancreatic cancer. The second had a 15 mm tumour and a two year history of abdominal pain, nausea and weight loss.
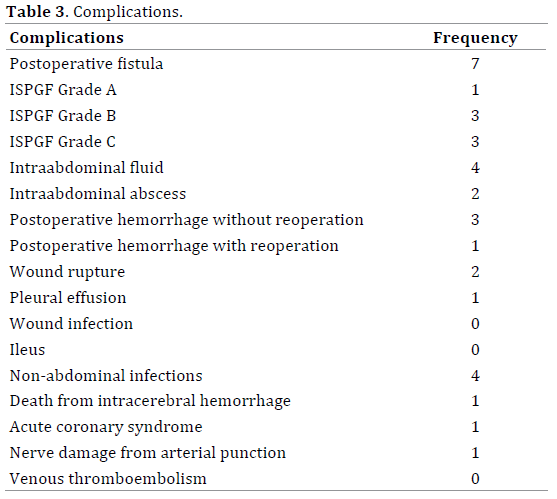
Complications are summarised in Table 3. Twenty-three patients had 27 complications, 15 of these were mild; Accordion Classification grade 1 through 6 were 15, 6, 3, 2, 0 and 1, respectively. Fistulas complicated the postoperative period in seven patients (10%). ISGPF group classification is specified in table 3. Two patients were reoperated for bleeding and wound rupture (at the site of specimen removal), respectively. Two other patients with pseudocysts were converted to a laparotomy, one for the construction of a jejunal anastomosis, the other because of a bleeding that could not be controlled laparoscopically. One patient suffered a cerebral bleeding shortly after a distal pancreatectomy with splenectomy, and died 11 days postoperatively. The complication rate did not differ between patients having lesions with or without a malignant potential (37% vs. 31%, P>0.6). Overall, length of hospital stay was median 6 days (range 1 to 55 days).
In three patients the pathologist reported a positive microscopic margin, one with SCN and two with SPPN. The latter two patients have been subject to follow-up, and there have been no recorded recurrences of the neoplasms with an observation of 9 to 57 months. R0 resection was verified in the remaining patients.
DISCUSSION
The proportion of patients with malignant or premalignant cystic neoplasms was 39%; 61% had no malignant potential. The majority had SCNs or pseudocysts. These numbers illustrate the final outcome of the present selection criteria, ie, no preoperative endoscopic ultrasound examination and hence no analyses of cyst fluid for CEA and/or amylase. However, the morbidity after laparoscopic surgery on the distal pancreas was low, and the majority of the complications were mild.
In this study the majority of the patients underwent surgery for a benign lesion (83%). There are no previous Scandinavian reports on the results of laparoscopic surgery in cystic pancreatic lesions in this period of time. Our results are comparable to previous studies. In two larger studies by Song and Mabrut the proportion of patients with benign tumours was 75 and 87%, respectively [17, 18].
To avoid surgery in benign cystic lesions, the neoplasms must first be correctly identified. Contrast-enhanced triphasic CT has been the preferred modality both to localize and characterize a cystic lesion, and also because it properly defines the relationship to surrounding organs and identifies metastases. MRI has been considered most suitable to identify mural nodules and cysts communicating with the pancreatic ducts. Due to technological advances, CT now performs similarly [19]. Commonly, studies of cystic lesions are focused on the differentiation between mucinous and nonmucinous, or benign and malignant, analogous to the management algorithms. The accuracy of both CT and MRI has proven suboptimal in this respect [20-25]. Considering our patient cohort, it is of special concern that the sensitivity of CT in diagnosing SCNs has been reported as low as 25% [22, 26]. A central scar is commonly considered diagnostic, but is reported to be present in only 22% of cases [27]. EUS-FNA is now widely available, but whether the added information is of clinical use, is debated. The recently published International guidelines on the management of IPMN and MCN [1] recommends EUS in several clinical scenarios. One of these is the differentiation between an oligocystic SCN and MCN, but only 4 of our patients had an oligocystic SCN. The European guidelines on cystic tumours of the pancreas do not recommend EUS as part of the routine workup, but merely as an option in difficult cases [2]. Low levels of CEA (carcino embryonic antigen) in cyst fluid from SCNs was found by Tatsuta et al. in 1986 [28]. A pooled analysis by van der Waaij et al. demonstrated that a CEA <5 ng/mL suggested a SCN or pseudocyst with a specificity of 95% [29]. The sensitivity for a SCN was 75%. These findings suggest that many of the SCNs in our study cohort could have been diagnosed by EUS-FNA.
Overall morbidity in our study was 33%, and fistula rate was 10%. The literature on laparoscopic distal pancreatectomy for the subgroup of cystic lesions is limited [30]. The previously reported fistula rates in similar studies have ranged from 8 to 50%[ 10, 31]. Contrary to our findings, a higher proportion of grade A fistulas would be expected [17]. Mortality in laparoscopic distal pancreatectomy is low. When summarizing the data from similar studies (including more than 50 patients), there were 3 reported deaths in 950 patients (0.3%) who underwent laparoscopic distal pancreatic resections [17, 18, 32-36]. The occurrence of a postoperative cerebral haemorrhage in one patient is not specifically attributable to laparoscopic pancreatic surgery, but nonetheless highlights the overall risk of surgery and the principle that patient selection is essential in surgical practice in general.
In recent reports the most prevalent cystic neoplasm of the pancreas has been IPMN [17, 37, 38], but only 4 patients had this neoplasm in the present cohort. SCN was the predominant neoplasm (42%). A higher prevalence of SCN in the Western than the Eastern hemisphere has been suggested [39]. Resection of SCN is today restricted to patients with symptoms, which is correlated with size. Two studies have demonstrated that when tumour diameter exceeds 40 mm, SCNs are frequently symptomatic [40, 41]. In the present study, 19 of the 29 SCNs had a diameter less than 40 mm. We conclude that surgery most likely was avoidable in the majority of these patients.
Gaujoux et al. compared the management of patients with cystic lesions of the pancreas in two sequential time periods (1995-2005 and 2005-2010), and found significant differences[38]. The handling of the cystic lesions changed significantly between these two periods. During the first time period 43% of the patients underwent initial resection, decreasing to 33% in the second. Furthermore, the rate of resected SCNs decreased from 34% to 13%. The authors interpreted this as a result of an increased ability to identify lesions radiographically, the use of EUS-FNA with cyst fluid analysis of CEA and a general acknowledgement that serous lesions are benign.
In our study 11 patients had pseudocysts. The patients were included because there was an explicit suspicion of a cystic neoplasm after preoperative work-up. EUS with FNA might have changed the management of these patients, but there are no adequate cyst fluid markers to make a certain diagnosis of a pseudocyst [42]. Publications on radiology have frequently been biased by the exclusion of pseudocysts.
Only patients accepted for surgery were included in the database. Some lesions were both cystic and solid in appearance, and were mainly excluded from this study (and regarded as solid).
In some of these the cystic component was the dominant feature and histology revealed ductal adenocarcinomas, a constellation that should always be considered in cystic lesions of the pancreas [43].
The approach described in this paper means no followup group including the risk for developing cancer. We even must take into account what it means for the single patient to be in a follow-up group (QoL), even if the risk for developing cancer is very low. Based on improved technology and better knowledge of preoperative diagnostics, it is even important to evaluate the current approach based on existing guidelines.
In conclusion, most postoperative complications were mild after laparoscopic distal resection of cystic pancreatic lesions, but this fact does not justify the present high proportion of patients with benign lesions (61%). The death of one patient after postoperative intracerebral hemorrhage underlines that improved preoperative patient selection is mandatory. Endoscopic ultrasound examination (EUS), enabling aspiration of cyst fluid and fine needle aspiration (FNA) is an additional option for the preoperative workup.
Conflicting Interest
The authors had no conflicts of interest
References
- Tanaka M, Fernandez-Del Castillo C, Adsay V, Chari S, Falconi M, Jang JY, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012;12:183-197. [PMID: 22687371]
- Del Chiaro M, Verbeke C, Salvia R, Kloppel G, Werner J, McKay C et al. European experts consensus statement on cystic tumours of the pancreas. Dig Liver Dis 2013. [PMID: 23415799]
- Khalid A, Brugge W. ACG practice guidelines for the diagnosis and management of neoplastic pancreatic cysts. Am J Gastroenterol 2007;102:2339-2349. [PMID: 17764489]
- Correa-Gallego C, Ferrone CR, Thayer SP, Wargo JA, Warshaw AL, Fernandez-Del Castillo C. Incidental pancreatic cysts: do we really know what we are watching? Pancreatology 2010;10:144-150. [PMID: 20484954]
- Del Chiaro M, Segersvard R, Pozzi Mucelli R, Rangelova E, Kartalis N, Ansorge C et al. Comparison of Preoperative Conference-Based Diagnosis with Histology of Cystic Tumors of the Pancreas. Ann Surg Oncol 2014. [PMID: 24385209]
- Fritz S, Klauss M, Bergmann F, Hackert T, Hartwig W, Strobel O et al. Small (Sendai Negative) Branch-Duct IPMNs: Not Harmless. Ann Surg 2012;256:313-320. [PMID: 22791105]
- Schmidt CM. Is surgical intervention for cystic neoplasms of the pancreas being underutilized? J Gastrointest Surg 2014;18:184-186. [PMID: 24170607]
- Allen PJ. Operative resection is currently overutilized for cystic lesions of the pancreas. J Gastrointest Surg 2014;18:182-183. [PMID: 24165874]
- Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Falconi M, Shimizu M et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 2006;6:17-32. [PMID: 16327281]
- Pryor A, Means JR, Pappas TN. Laparoscopic distal pancreatectomy with splenic preservation. Surg Endosc 2007;21:2326-2330. [PMID: 17593458]
- Crippa S, Bassi C, Salvia R, Falconi M, Butturini G, Pederzoli P. Enucleation of pancreatic neoplasms. Br J Surg 2007;94:1254-1259. [PMID: 17583892]
- Rosok BI, Marangos IP, Kazaryan AM, Rosseland AR, Buanes T, Mathisen O et al. Single-centre experience of laparoscopic pancreatic surgery. Br J Surg 2010;97:902-909. [PMID: 20474000]
- Porembka MR, Hall BL, Hirbe M, Strasberg SM. Quantitative weighting of postoperative complications based on the accordion severity grading system: demonstration of potential impact using the american college of surgeons national surgical quality improvement program. J Am Coll Surg 2010;210:286-298. [PMID: 20193891]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005;138:8-13. [PMID: 16003309]
- Klöppel G. Histological typing of tumours of the exocrine pancreas. 2nd ed. ed. Berlin: Springer, 1996.
- Bosnan FT. WHO classification of tumours of the digestive system. Lyon: IARC, 2010.
- Song KB, Kim SC, Park JB, Kim YH, Jung YS, Kim MH et al. Single-center experience of laparoscopic left pancreatic resection in 359 consecutive patients: changing the surgical paradigm of left pancreatic resection. Surg Endosc 2011;25:3364-3372. [PMID: 21556993]
- Mabrut JY, Fernandez-Cruz L, Azagra JS, Bassi C, Delvaux G, Weerts J et al. Laparoscopic pancreatic resection: results of a multicenter European study of 127 patients. Surgery 2005;137:597-605. [PMID: 15962401]
- Katz DS, Friedel DM, Kho D, Georgiou N, Hines JJ. Relative accuracy of CT and MRI for characterization of cystic pancreatic masses. AJR Am J Roentgenol 2007;189:657-661. [PMID: 17715114]
- Fisher WE, Hodges SE, Yagnik V, Moron FE, Wu MF, Hilsenbeck SG et al. Accuracy of CT in predicting malignant potential of cystic pancreatic neoplasms. HPB (Oxford) 2008;10:483-490. [PMID: 19088937]
- Visser BC, Yeh BM, Qayyum A, Way LW, McCulloch CE, Coakley FV. Characterization of cystic pancreatic masses: relative accuracy of CT and MRI. AJR Am J Roentgenol 2007;189:648-656. [PMID: 17715113]
- Curry CA, Eng J, Horton KM, Urban B, Siegelman S, Kuszyk BS et al. CT of primary cystic pancreatic neoplasms: can CT be used for patient triage and treatment? AJR Am J Roentgenol 2000;175:99-103. [PMID: 10882255]
- Pongpornsup S, Piyapittayanan S, Charoensak A. MDCT imaging findings for characterization pancreatic cystic lesion: differentiation between benign and malignant pattern. J Med Assoc Thai 2011;94:369-378. [PMID: 21560846]
- Visser BC, Muthusamy VR, Yeh BM, Coakley FV, Way LW. Diagnostic evaluation of cystic pancreatic lesions. HPB (Oxford) 2008;10:63-69. [PMID: 18695762]
- Procacci C, Biasiutti C, Carbognin G, Accordini S, Bicego E, Guarise A et al. Characterization of cystic tumors of the pancreas: CT accuracy. J Comput Assist Tomogr 1999;23:906-912. [PMID: 10589565]
- Khashab MA, Shin EJ, Amateau S, Canto MI, Hruban RH, Fishman EK et al. Tumor size and location correlate with behavior of pancreatic serous cystic neoplasms. Am J Gastroenterol 2011;106:1521-1526. [PMID: 21468008]
- Sun HY, Kim SH, Kim MA, Lee JY, Han JK, Choi BI. CT imaging spectrum of pancreatic serous tumors: based on new pathologic classification. Eur J Radiol 2010;75:e45-55. [PMID: 20056368]
- Tatsuta M, Iishi H, Ichii M, Noguchi S, Yamamoto R, Yamamura H et al. Values of carcinoembryonic antigen, elastase 1, and carbohydrate antigen determinant in aspirated pancreatic cystic fluid in the diagnosis of cysts of the pancreas. Cancer 1986;57:1836-1839. [PMID: 2420441]
- van der Waaij LA, van Dullemen HM, Porte RJ. Cyst fluid analysis in the differential diagnosis of pancreatic cystic lesions: a pooled analysis. Gastrointest Endosc 2005;62:383-389. [PMID: 16111956]
- Fernandez-Cruz L, Martinez I, Gilabert R, Cesar-Borges G, Astudillo E, Navarro S. Laparoscopic distal pancreatectomy combined with preservation of the spleen for cystic neoplasms of the pancreas. J Gastrointest Surg 2004;8:493-501. [PMID: 15120376]
- Teh SH, Tseng D, Sheppard BC. Laparoscopic and open distal pancreatic resection for benign pancreatic disease. J Gastrointest Surg 2007;11:1120-1125. [PMID: 17623260]
- Melotti G, Butturini G, Piccoli M, Casetti L, Bassi C, Mullineris B et al. Laparoscopic distal pancreatectomy: results on a consecutive series of 58 patients. Ann Surg 2007;246:77-82. [PMID: 17592294]
- Kim SC, Park KT, Hwang JW, Shin HC, Lee SS, Seo DW et al. Comparative analysis of clinical outcomes for laparoscopic distal pancreatic resection and open distal pancreatic resection at a single institution. Surg Endosc 2008;22:2261-2268. [PMID: 18528619]
- Kooby DA, Gillespie T, Bentrem D, Nakeeb A, Schmidt MC, Merchant NB et al. Left-sided pancreatectomy: a multicenter comparison of laparoscopic and open approaches. Ann Surg 2008;248:438-446. [PMID: 18791364]
- DiNorcia J, Schrope BA, Lee MK, Reavey PL, Rosen SJ, Lee JA et al. Laparoscopic distal pancreatectomy offers shorter hospital stays with fewer complications. J Gastrointest Surg 2010;14:1804-1812. [PMID: 20589446]
- Vijan SS, Ahmed KA, Harmsen WS, Que FG, Reid-Lombardo KM, Nagorney DM et al. Laparoscopic vs open distal pancreatectomy: a single-institution comparative study. Arch Surg 2010;145:616-621. [PMID: 20644122]
- Yoon WJ, Lee JK, Lee KH, Ryu JK, Kim YT, Yoon YB. Cystic neoplasms of the exocrine pancreas: an update of a nationwide survey in Korea. Pancreas 2008;37:254-258. [PMID: 18815545]
- Gaujoux S, Brennan MF, Gonen M, D'Angelica MI, DeMatteo R, Fong Y et al. Cystic lesions of the pancreas: changes in the presentation and management of 1,424 patients at a single institution over a 15-year time period. J Am Coll Surg 2011;212:590-600; discussion 600-593. [PMID: 21463795]
- Yoon WJ, Brugge WR. Pancreatic cystic neoplasms: diagnosis and management. Gastroenterol Clin North Am 2012;41:103-118. [PMID: 22341252]
- Tseng JF, Warshaw AL, Sahani DV, Lauwers GY, Rattner DW, Fernandez-del Castillo C. Serous cystadenoma of the pancreas: tumor growth rates and recommendations for treatment. Ann Surg 2005;242:413-419; discussion 419-421. [PMID: 16135927]
- Malleo G, Bassi C, Rossini R, Manfredi R, Butturini G, Massignani M et al. Growth pattern of serous cystic neoplasms of the pancreas: observational study with long-term magnetic resonance surveillance and recommendations for treatment. Gut 2011. [PMID: 21940725]
- Park WG, Mascarenhas R, Palaez-Luna M, Smyrk TC, O'Kane D, Clain JE et al. Diagnostic performance of cyst fluid carcinoembryonic antigen and amylase in histologically confirmed pancreatic cysts. Pancreas 2011;40:42-45. [PMID: 20966811]
- Marangos IP, Buanes T, Rosok BI, Kazaryan AM, Rosseland AR, Grzyb K et al. Laparoscopic resection of exocrine carcinoma in central and distal pancreas results in a high rate of radical resections and long postoperative survival. Surgery 2012;151:717-723. [PMID: 22284762]


