Keywords
Cachexia; Depression; Exocrine Pancreatic Insufficiency; Intestinal Obstruction; Jaundice; Pain; Pancreas; Pancreatic Neoplasms; Stents
INTRODUCTION
Palliative care should be offered at the initiation of treatment for people who are diagnosed with pancreatic cancer, given the poor relative survival rate and the intractable symptom profile of those who have this lifelimiting disease. The clinical manifestations of pancreatic cancer can include pain, unexplained weight loss, nausea, vomiting (gastric outlet obstruction), steatorrhea (malabsorption), dyspepsia, depression, deep venous thrombosis, pruritus, and jaundice. Unfortunately, there are no specific warning signs of pancreatic cancer. New onset diabetes with no risk factors has been associated with pancreatic cancer [1]. Only few studies were presented at the 2011 American Society of Clinical Oncology (ASCO) Annual Meeting and three of them are summarized below.
Biliary Stent Complications
Espinoza et al. (Abstract #e14665) reviewed charts of patients with chemo-naïve advanced pancreatic cancer who were enrolled on three clinical studies consisting of gemcitabine-based combination chemotherapy regimens and assessed the biliary stent outcomes including stent complication rate, rate of treatment delays due to stent complications, and total number of endoscopic interventions per patient [2]. Outcomes were compared for patients with plastic stent vs. metal stent. Among 22 required stent placements, 9 patients had metal stent, 13 had plastic stent at the start of treatment who had regular stent exchanges performed.
Fifty-four percent (n=7) patients in the plastic stent group had stent complications during treatment while 22% (n=2) in the metal stent group had complications. These episodes led to treatment delays in 31% (n=4) patients in the plastic stent group. There was no treatment delays in the metal stent group related to the stent complications. Metal stent group underwent an average of 2.85 endoscopic or percutaneous procedures compared to 1 in the metal stent group.
This study supports the placement of metal stent. This issue is more pertinent in patients who will require myelosuppressive combination chemotherapy regimens for their treatment of pancreatic cancer.
Anticoagulation in Patients with Splanchnic Venous Thrombosis
With advances in CT-imaging, an increasing number of incidental venous thromboembolism, including splanchnic thromboembolism, is being diagnosed in patients with pancreatic cancer. However, its natural history and management remain poorly characterized. Kar et al. (Abstract #e14622) presented their data on an important aspect of pancreatic cancer [3]. Eighty-one patients with advanced pancreatic cancer with splanchnic thromboembolism identified on CT imaging were included. All baseline and follow up CT scans were reviewed to record thrombus site, type and progression on follow up.
Primary sites of splanchnic thromboembolism included:
• portal vein (49%);
mesenteric
• splenic vein (23%).
Forty-eight percent received anticoagulation: 90% received low molecular weight heparin while the rest 10% were administered with warfarin.
The most common complications associated with splanchnic thromboembolism are shown in Table 1.
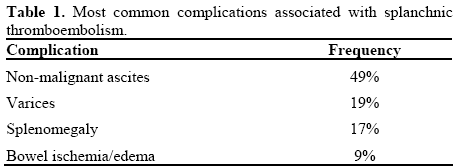
The investigators found that median survival in patients with ascites vs. those without ascites was 23 vs. 38 weeks (P=0.09) on univariate analysis. Minor bleeding (7%) was the only adverse event attributable to anticoagulation
The authors concluded that progressive splanchnic thromboembolism is associated with an increased rate of complications and poor survival in patients with advanced pancreatic cancer. Moreover, anticoagulation in this setting is safe and may reduce risk of splanchnic thromboembolism-related ascites. However, the impact of anticoagulation on survival warrants to be investigated in future studies.
Semuloparin for Prevention of Venous Thromboembolism in Patients with Cancer Receiving Chemotherapy: the SAVE-ONCO Study
Pancreatic cancer is a hypercoagulable condition, and venous thromboembolism affects up to 17% to 57% of pancreatic cancer patients. Initiating chemotherapy further increases the risk. For cancer patients initiating chemotherapy, there is currently no approved treatment for the primary prevention of venous thromboembolism risk [4]. Semuloparin significantly decreases the risk of venous thromboembolism by 64% compared to placebo in cancer patients initiating a chemotherapy regimen, according to results of the phase III study “Evaluation of AVE5026 in the Prevention of Venous Thromboembolism in Cancer Patients Undergoing Chemotherapy” (SAVE-ONCO) reported at the 2011 ASCO Annual Meeting by Agnelli et al. (Abstract #LBA9014) [5].
Semuloparin is an investigational ultra-low-molecularweight heparin with high anti-factor Xa and residual anti-factor IIa activities. Agnelli et al. randomized 3,212 patients with locally advanced or metastatic solid malignancies initiating chemotherapy to receive subcutaneous semuloparin, 20 mg qd, or placebo, until a change in chemotherapy. Study participants had diagnoses of lung, colon-rectal, stomach, ovary, pancreas, or bladder cancer. The primary efficacy outcome was the composite of any symptomatic deep vein thrombosis, non-fatal pulmonary embolism, and venous thromboembolism-related death. Of 3,212 randomized patients, about two-thirds had metastatic disease. The median treatment duration was about 3.5 months. Twenty (1.2%) of the 1,608 semuloparintreated patients and 55 (3.4%) of the 1,604 placebotreated patients had a thromboembolic event, amounting to a 64% risk reduction in the event rate (hazard ratio, HR=0.36; 95% confidence interval, CI: 0.21-0.60; P<0.0001, intent-to-treat analysis). The treatment effect was consistent for deep vein thrombosis and pulmonary embolism, with a 59% risk reduction in pulmonary embolism rate (odds ratio, OR=0.41; 95% CI: 0.19-0.85). No heterogeneity in the benefit was observed for cancer type or stage.
Semuloparin was well tolerated with a similar rate of treatment-emergent adverse events as placebo. The rate of clinically relevant bleeding was 2.8% with semuloparin compared with 2.0% with placebo (HR=1.40; 95% CI: 0.89-2.21).
The authors concluded that their data have demonstrated the benefit of thromboprophylaxis using semuloparin in patients receiving chemotherapy without an increase in major bleeding.
Conclusions
In a nut shell, the palliation of symptoms is arguably the most important aim in treating patients with advanced pancreatic cancer. The distressing symptoms that most patients with pancreatic cancer experience heighten the importance of early palliative-care intervention. At diagnosis patients often present with fatigue, loss of appetite, impaired sense of well-being, and pain. In addition to traditional palliative measures of managing pain and symptoms, surgery and endoscopy may in some instances play a role in palliation. In addition, thromboembolic disease in pancreatic cancer poses a life-threatening complication and is often regarded as paraneoplastic syndrome associated with pancreatic cancer. Effective management of this risk factor is very important in the management of pancreatic cancer. Future research needs to understand the effect of early palliative care interventions not only on quality of life measures but also on survival.
Conflict of interest
The author has no potential conflicts of interest
References
- Fazal S, Saif MW. Supportive and palliative care of pancreatic cancer. JOP. J Pancreas (Online) 2007 Mar 10;8(2):240-53.
- Espinoza AM, Ko AH, Ostroff JW, Venook AP, Bergsland EK, Kelley RK, et al. Biliary stent complications in clinical trials for advanced pancreatic cancer. J Clin Oncol 2011; 29(Suppl.):e14665.
- Kar SP, Bhosale P, Overman MJ, Weatherly J, Xiao L, Wolff RA, Javle MM. Role of anticoagulation (AC) in patients with advanced pancreatic cancer (APC) with splanchnic venous thrombosis (SVT). J Clin Oncol 2011; 29(Suppl.):e14622.
- Sohail MA, Saif MW. Role of anticoagulation in the management of pancreatic cancer. JOP. J Pancreas (Online) 2009Mar 9;10(2):82-7.
- Agnelli G, George DJ, Fisher W, Kakkar AK, Lassen MR, Mismetti P, et al. The ultra-low molecular weight heparin (ULMWH) semuloparin for prevention of venous thromboembolism (VTE) inpatients with cancer receiving chemotherapy: SAVE ONCO study. J Clin Oncol 2011; 29(Suppl.):LBA9014

