Keywords
Gene Expression; Immunotherapy; Pancreatic Neoplasms
Abbreviations
CFTR cystic fibrosis transmembrane conductance
regulator; MRI magnetic resonance imaging; RAP recurrent acute
pancreatitis; s-MRCP secretin enhanced magnetic resonance
cholangiopancreatography
INTRODUCTION
Pancreas divisum is the most common congenital
anatomic abnormality of the pancreas. During the sixth
week of gestation, the pancreas normally develops from
the fusion of the dorsal and ventral pancreatic buds. The
dorsal bud forms the head, body, and tail while the ventral
bud develops into the uncinate process. In the majority of
individuals, the union of these structures allows for a fusion
of their ductal systems such that the main pancreatic duct
serves as the path for emptying of pancreatic secretions
into the duodenum via the major duodenal papilla. A
normal variant anatomy is present in approximately 30%
of individuals, where the proximal dorsal pancreatic duct
persists as an accessory pancreatic duct and empties via
the minor duodenal papilla [1]. On the contrary, in typical
Pancreas divisum, the fusion of the dorsal and ventral
ductal systems fails, forming two distinct conduits with
the dorsal duct draining the majority of the pancreas via
the minor papilla and the ventral duct draining only the
inferior portion of the head of the pancreas via the major
papilla [2]. The normal anatomy of the pancreas as well as anatomic variant findings in pancreas divisum is illustrated
in Figure 1. Another anatomic variant, incomplete pancreas
divisum, is infrequent, and presents as a narrow and often
inadequate connection between the dorsal and ventral
pancreatic ducts, with the majority of drainage occurring
via the smaller minor papilla [3]. Autopsy series have
reported the incidence of pancreas divisum to be in the
order of 5-10% of the general population [4, 5]. Although
pancreas divisum is a congenital anomaly present at birth,
it is often not diagnosed until the fifth decade of life, when
it becomes symptomatic [6, 7]. With increasing use of
cross-sectional diagnostic imaging, pancreas divisum is
being diagnosed earlier in asymptomatic patients.
Figure 1. Pancreatic ductal anatomy variants.
The clinical significance of pancreas divisum is often
considered when it is found in patients with idiopathic
acute or recurrent pancreatitis. Cotton [6] first suggested a
correlation between pancreas divisum and development of
pancreatitis in a retrospective series of patients undergoing
endoscopic retrograde cholangiopancreatography (ERCP).
While the overall incidence of pancreas divisum was
3.6% in the series, patients with unexplained recurrent
pancreatitis had a much higher incidence of 25.6%.
Although this study was weakened by a referral bias and
did not consider alternative etiologies for pancreatitis,
such as genetic or autoimmune causes, it did lead to
further interest in a potential role of pancreas divisum in
the development of acute and recurrent pancreatitis. The
proposed mechanism for pancreatitis in pancreas divisum
is an obstructive pancreatopathy, with the narrow minor
papilla bearing the responsibility for draining the majority
of the pancreas by way of the dorsal pancreatic duct [6, 8].
In an attempt to quantify this, Staritz et al. [9] performed
ERCP with manometry on patients with pancreas divisum
and found relatively increased pressures in the dorsal duct
as compared to the ventral duct. However, the evidence is
equivocal: Satterfield et al. [10] found no difference in both
basal and phasic manometric pressures from the major
and minor papilla in patients with pancreas divisum and
acute pancreatitis. From an anatomic standpoint, Wang et al. [11] used magnetic resonance imaging (MRI) and
magnetic resonance cholangiopancreatography (MRCP) to
support the dorsal obstructive hypothesis by showing that
isolated dorsal pancreatic involvement was more common
in patients with pancreatitis and pancreas divisum, 44.74%
as compared to 22.22% in controls, with pancreatitis but
without pancreas divisum.
With increasing use of MRI and MRCP in the past twenty
years, the detection of pancreas divisum is increasingly
common in patients undergoing cross-sectional imaging.
MRCP has been shown to have the same diagnostic
accuracy in the diagnosis of pancreas divisum as ERCP
[12]. Furthermore, secretin-enhanced MRCP (S-MRCP)
may enhance detection of pancreas divisum by stimulating
bicarbonate and fluid secretion into the pancreatic ducts,
allowing for improved visualization of anatomic features
[13]. A meta-analysis of 10 studies with 1474 patients
showed that secretin-enhanced MRCP had increased
diagnostic performance with sensitivity of 86% as
compared to 52% for standard MRCP, thus strengthening
the role of non-invasive imaging for the diagnosis of
pancreas divisum [14]. With increased access to radiology
facilities with MRI/MRCP capabilities, these imaging
modalities will continue to serve as the new standard in
diagnosis of pancreas divisum.
Therapeutic Interventions
Therapeutic interventions for patients with recurrent
acute pancreatitis (RAP) and pancreas divisum aim to
relieve the relative obstructive pancreatopathy caused by
a stenotic minor papilla. While surgical intervention such
as minor papilla sphincteroplasty has been performed with
some success [15, 16, 17], endoscopic therapy is favored
as a less invasive treatment modality. Endotherapy for
pancreas divisum may include dorsal duct pancreatic
stent placement [18] or, more frequently, endoscopic
minor papillotomy [19]. In a randomized controlled trial,
patients with pancreas divisum were randomized to
either dorsal duct stent placement (in 10 patients) or no
intervention in controls (9 patients). With a mean followup
of about 30 months, no patients in the stent group
required hospitalization for abdominal pain but five out of
the nine patients in the control group were readmitted for
pain management. RAP was documented in one of the ten
stented patients and seven of the nine control patients [20].
In a long-term efficacy study endoscopic therapy, twentyfour
patients with RAP and underlying pancreas divisum
were treated with sphincterotomy of the minor papilla (8
patients) or dorsal duct stent insertion (16 patients). Acute
pancreatitis recurred in two of the eight patients treated
with sphincterotomy of the minor papilla and there was
no recurrence in patients that received a stent with a
median duration of follow-up of 39 months. On the other
hand, complication rate was less significant in the minor
papillotomy group (25%) as compared to the dorsal duct
stent group (44%) [21]. These endoscopic therapies have
shown clinical benefits in patients with RAP associated with
pancreas divisum, while patients with chronic pancreatitis
associated with pancreas divisum, or abdominal pain without pancreatitis, may not be ideal candidates for
these interventions [22, 23, 24]. Additionally, endotherapy
in patients with RAP due to Pancreas divisum has been
shown to decrease interval endosonographic findings of
chronic pancreatitis, suggesting that earlier therapy may
be warranted in these patients [25]. However, while the
typical rate of post-ERCP pancreatitis is estimated at 3.5%
[26], this risk is increased to as high as 10.6% with dorsal
duct cannulation and minor sphincter papillotomy [27].
Therefore, the benefits must be weighed against the risks
of endotherapy, with particular consideration to the added
risk of post-ERCP pancreatitis with endoscopic minor
papillotomy.
Is Endotherapy Alone the Answer?
Although patients with RAP and pancreas divisum
undoubtedly benefit from minor papillotomy, there is
ongoing debate about the true cause of the pancreatitis: is it
the anatomy alone, or are other comorbidities responsible?
Spicak et al. [28] used MRCP and ERCP to study the impact
of pancreas divisum on the natural course of chronic
pancreatitis. They found that pancreas divisum did not
modify the age of onset of CP, and, despite the presence
of pancreas divisum, a majority of their patients still had
abnormalities of the ventral duct (75% in patients with, and
72% in patients without, a history of alcohol abuse), with
a low frequency having dorsal duct involvement (25% and
28%, respectively). With these findings, the investigators
theorized that pancreas divisum in itself does not modify
the natural course of chronic pancreatitis.
Genetic Mutations
This argument was further advanced by the observation
that genetic mutations associated with pancreatitis may
be seen in higher frequencies in patients with pancreas
divisum. Pramod et al. [29] found SPINK-1 mutations were
more common in patients with pancreas divisum with RAP
(41.6%) as compared to healthy controls without pancreas
divisum (2%). The mutation was present in similar
frequency in patients without pancreas divisum who had
idiopathic chronic pancreatitis (43.3%) and idiopathic
RAP (35.7%) suggesting that in this population, SPINK-1 mutation and not pancreas divisum may be a common
factor leading to development of pancreatitis.
Anomalies of the CFTR gene have also been associated
with development of pancreatitis in patients with pancreas
divisum. Dray et al. [30] reported two cases of young
female patients with pancreas divisum and RAP who were
found to have a mildly abnormal CFTR genotype (IVS8-
5T-TG12) which led to RAP with only mild upper airway
manifestations. They theorized that the mild CFTR protein
dysfunction and resulting impaired epithelial ion transport
results in abnormal pancreatic fluid secretion, leading to
RAP in pancreas divisum. Gerlud et al. [31] showed that
patients with pancreas divisum and RAP had a decrease in CFTR function intermediate between patients with cystic
fibrosis and healthy controls. They hypothesized that in
addition to increased viscosity of pancreatic fluid, CFTR dysfunction may also cause an excessive host inflammatory
response that may further narrow the already smaller
pancreatic duct orifice in pancreas divisum, predisposing
patients to pancreatitis. In a recent MRCP study, Bertin et
al. [32] enrolled consecutive patients with acute recurrent
and chronic pancreatitis and found that the frequency
of pancreas divisum was greater in patients with CFTR associated
pancreatitis (47%), as compared to healthy
controls (7%) and alcohol-induced pancreatitis (7%).
With these findings, the investigators suggested CFTR mutations or other polymorphisms in patients with
pancreas divisum might explain why only a subset of
patients with this disorder develops pancreatitis. On the
other hand, in their editorial for the Bertin et al. study,
DiMagno and DiMagno [33] caution that ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¦Ã¢â¬Åcorrelation does
not equal causationÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâàand suggest that CFTR mutations and
pancreas divisum may co-exist without influencing genetic
susceptibility to pancreatitis. Recently, Ballard et al. [34]
found that in individuals with adult-onset pancreatic
disease, the discovery of high risk mutations may be
facilitated with using complete gene sequencing. Further
study into the association of CFTR mutation and pancreas
divisum, perhaps using complete gene sequencing, will be
needed to settle this debate.
Summary
Although pancreas divisum has been an anatomic
finding described in the literature for since the 19th
century, the debate as to whether it causes pancreatitis, or
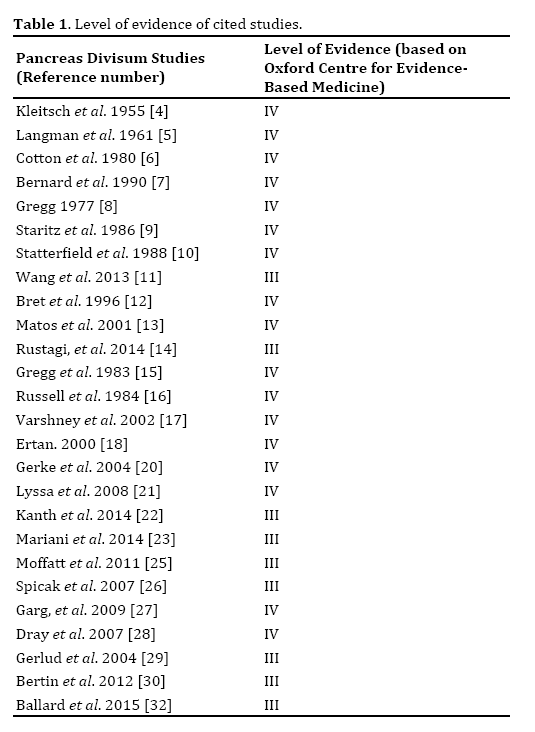
is simply a bystander, lives on to this day. Historically, the study of pancreas divisum has been limited to uncontrolled
and observational studies as evidenced in this paper
(Table 1). Clinicians should be aware of this entity: given
the prevalence of close to 10% in the general population,
with the increasing use of cross-sectional imaging it
will become a more common incidental finding. When
encountered in a patient with idiopathic RAP, genetic
testing should be considered. Research into the outcomes
of minor papilla endotherapy in the subset of patients with
pancreas divisum and genetic anomalies, such as CFTR mutation, should be pursued in the future.
Conflict of Interest
The authors declare that there is no conflict of interests
regarding the publication of this paper.
References
- Schoenwolf G, Bleyl S, Brauer P, Francis-West P. Larsen's Human Embryology. (5th edu), Philadelphia, PA: Elsevier, 2015.
- Klein SD, Affronti JP. Pancreas divisum, an evidence-based review: part I, pathophysiology. Gastrointest Endosc 2004; 60:419-425. [PMID: 15332034]
- MortelÃÆÃâÃâ ââ¬â¢ÃÆââ¬Å¡Ãâé KJ, Rocha TC, Streeter JL, Taylor AJ. Multimodality imaging of pancreatic and biliary congenital anomalies. Radiographics 2006; 26:715-731. [PMID: 16702450]
- Kleitsch WP. Anatomy of the pancreas: A study with special reference to the duct system. ANA Arch Surgery 1955; 71:795-802. [PMID: 13268234]
- Dawson W, Langman J. An anatomical-radiological study of the pancreatic duct patternin in man. Anat Rec 1961; 139: 59-68. [PMID: 14025604]
- Cotton PB. Congenital anomaly of pancreas divisum as a cause of obstructive pain and pancreatitis. Gut 1980; 21:105-114. [PMID: 7380331]
- Bernard JP, Sahel J, Giovannini M, Sarles H. Pancreas divisium is a probable cause of acute pancreatitis: A case report of 137 cases. Pancreas 1990; 5:248-254. [PMID: 2343039]
- Gregg JA. Pancreas divisum: Its association with pancreatitis. Am J Surg 1977; 134:539-543. [PMID: 920876]
- Staritz M, HÃÆÃâÃâ ââ¬â¢ÃÆââ¬Å¡Ãâütteroth T, Meyer zum BÃÆÃâÃâ ââ¬â¢ÃÆââ¬Å¡Ãâüschenfelde KH. Pancreas divisum and pancreatitis. Gastroenterology 1986; 91:525-526. [PMID: 3721136]
- Satterfield ST, McCarthy JH, Geenen JE, Hogan WJ, Venu RP, Dodds WJ, Johnson GK. Clinical experience in 82 patients with pancreas divisum: Preliminary results of manometry and endoscopic threapy. Pancreas 1988; 3:248-254. [PMID: 3387418]
- Wang DB, Yu J, Fulcher AS, Turner MA. Pancreatitis in patients with pancreas divisum: Imaging features at MRI and MRCP. World J Gastroenterol 2013; 19:4907-4916. [PMID: 23946595]
- Bret PM, Reinhold C, Taourel P, Guibaud L, Atri M, Barkun AN. Pancreas divisum: evaluation with MR cholangiopancreatography. Radiology 1996; 199:99-103. [PMID: 8633179]
- Matos C, Metens T, DeviÃÆÃâÃâ ââ¬â¢ÃÆââ¬Å¡Ãâère J, Delhaye M, Le Moine O, Cremer M. Pancreas divisum: evaluation with secretin-enhanced magnetic resonance cholangiopancreatography. Gastrointest Endosc 2001; 53:728-733. [PMID: 11375579]
- Rustagi T, Njei B. Magnetic resonance cholangiopancreatography in the diagnosis of pancreas divisum: A systematic review and meta-analysis. Pancreas 2014; 43:823-828. [PMID: 24743381]
- Gregg JA, Monaco AP, McDermott WV. Pancreas divisum: Results of surgical intervention. The Am J Surg 1983; 145:488-492. [PMID: 6837884]
- Russell RC, Wong NW, Cotton PB. Accessory sphincterotomy (endoscopic and surgical) in patients with pancreas divisum. Br J Surg 1984; 71:954-957. [PMID: 6498472]
- Varshney S, Johnson CD. Surgery for pancreas divisum. Ann R Coll Surg Engl 2002; 71:954-957. [PMID: 12092866]
- Ertan A. Long-term results after endoscopic pancreatic stent placement withouut pancreatic papillotomy in acute recurrent pancreatitis due to pancreas divisum. Gastrointest Endosc 2000; 52:9-14. [PMID: 10882955]
- Vila JJ, Kutz MM. Sphincterotomy of the minor papilla. Video J Encyclop GI Endosc 2013; 1:588-592.
- Lans JI, Geenen JE, Johanson JF, Hogan WJ. Endoscopic therapy in patients with pancreas divisum and acute pancreatitis: a prospective, randomized, controlled clinical trial. Gastrointest Endosc 1992; 38:430-4. [PMID: 1511816]
- Heyries L, Barthet M, Delvasto C, Zamora C, Bernard JP, Sahel J. Long-term results of endoscopic management of pancreas divisum with recurrent acute pancreatitis. Gastrointest Endosc 2002; 55:376-81. [PMID: 11868012]
- Gerke H, Byrne MF, Stiffler HL, Obando JV, Mitchell RM, Jowell PS, et al. Outcome of endoscopic minor papillotomy in patients with symptomatic pancreas divisum. JOP 2004; 5:122-131. [PMID: 15138333]
- Chacko LN, Chen YK, Shah RJ. Clinical outcomes and nonendoscopic interventions after minor papilla endotherapy in patients with smymptomatic pancreas divisium. Gastrointest Endosc 2008; 68:667-673. [PMID: 18436218]
- Kanth R, Samji NS, Inaganti A, Komanapalli SD, Rivera R, Antillon MR, et al. Endotherapy in symptomatic pancreas divisum. Pancreatology 2014; 14:244-250. [PMID: 25062871]
- Mariani A, Di Leo M, Petrone MC, Arcidiacono PG, Giussani A, Zuppardo RA, Cavestro GM, et al. Outcome of endotherapy for pancreas divisum in patients with acute recurrent pancreatitis. World J Gastroenterol 2014; 14:17468-17474.75. [PMID: 25516660]
- Andriulli A, Loperfido S, Napolitano G, Niro G, Valvano MR, Spirito F, et al. Incidence rates of post-ERCP complications: a systemic survey of prospective studies. Am J Gastroenterol 2007; 102:1781-1788. [PMID: 17509029]
- Moffatt DC, CotÃÆÃâÃâ ââ¬â¢ÃÆââ¬Å¡Ãâé GA, Avula H, Watkins JL, McHenry L, Sherman S, et al. Risk factors for ERCP-related complications in patients with pancreas divisum: a retrospective study. Gastrointest Endosc 2011; 73:963-970. [PMID: 21392753]
- Spicak J, Poulova P, Plucnarova J, Rehor M, Filipova H, Hucl T. Pancreas divisum does not modify the natural course of chronic pancreatitis. J Gastroenterol 2007; 42:135-139. [PMID: 17351802]
- Garg PK, Khajuria R, Kabra M, Shastri SS. Association of SPINK1 gene mutation and CFTR gene polymorphisms in patients with pacreas divisum presenting with idiopathic pancreatitis. J Clin Gastroenterol 2009; 43:848-852. [PMID: 19593166]
- Dray X, Fajac I, Bienvenu T, Chryssostalis A, Sogni P, Hubert D. Association of pancreas divisum and recurrent acute pancreatitis with the IVS8-5T-12TG allele of the CFTR gene and CFTR gene dysfunction. Pancreas 2007; 35:90-93. [PMID: 17575549]
- Gelrud A, Sheth S, Banerjee S, Weed D, Shea J, Chuttani R, et al, Freedman SD.,. Analysis of cystic fibrosis gener product (CFTR) function in patients with pancreas divisum and recurrent acute pancreatitis. Am J Gastroenterol 2004; 99:1557-62. [PMID: 15307877]
- Bertin C, Pelletier AL, Vullierme MP, Bienvenu T, Rebours V, Hentic O, et al., Pancreas divisum is not a cause of pancreatitis by itself but acts as a partner of genetic mutations. Am J Gastroenterol 2012; 107:311-317. [PMID: 22158025]
- DiMagno MJ, Dimagno EP. Pancreas divisum does not cause pancreatitis, but associates with CFTR mutations. Am J Gastroenterol 2012; 107:318-320. [PMID: 22306946]
- Ballard DD, Flueckiger JR, Fogel EL, McHenry L, Lehman GA, Watkins JL, et al. Evaluating adults with idiopathic pancreatitis for genetic predisposition: Higher prevalence of abnormal results with use of complete gene sequencing. Pancreas 2015; 44:116-21. [PMID: 25251442]


