Keywords
Abdominal Injuries; Duodenum; Wounds and Injuries
Abbreviations PD: pancreaticoduodenectomy; PJ: pancreaticojejunostomy; PPTD: pancreas preserving total duodenectomy
INTRODUCTION
Severe duodenal injury is rare and remains a challenging problem [1, 2, 3, 4, 5]. The major concern is failure of the repair with resultant abdominal septic complications and fistula formation [2, 3, 4]. Complex enteric reconstruction and drainage procedures [5] have been employed for extensive damage to the duodenum: duodenal diverticulization [6], pyloric exclusion [7, 8], duodenal resection and anastomosis (duodenoduodenostomy, duodenojejunostomy) [9], ampullojejunostomy [10], duct reimplantation [11], pancreaticoduodenectomy [12, 13], pancreas preserving total duodenectomy [14, 15, 16] and bioprosthetic repair of enteric wall defects [5] Successful management depends on an appropriately selected procedure. Duodenum related morbidity ranges from 12% to 63% and the mortality rates range from 6% to 29% [1]. This paper reports our experience with pancreas-preserving total duodenectomy (PPTD) for complex duodenal injury.
CASE REPORTS
The details of two patients are presented in Table 1. Both patients had diffuse peritonitis. Contrast enhanced computed tomography (CECT) revealed pneumoperitoneum and extravasation of contrast from the duodenum (Figure 1). In one patient (Case 2), CECT revealed a non-enhancing right kidney.
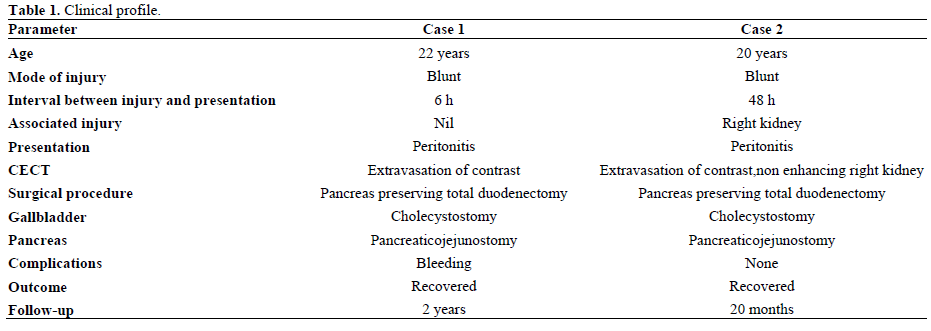
Figure 1. CECT showing extravasation of oral contrast from
duodenum.
At laparotomy, there was complete disruption of the duodenum (Figure 2). The ampulla was visible as a button on the pancreatic head .The duodenum was completely mobilized and carefully separated from the pancreas. Bleeding from the pancreatic surface was carefully secured. The viability of the ampulla was not in doubt. Reconstruction was achieved by end-to-side invagination pancreaticojejunostomy without duct to mucosa suturing of ampulla. The jejunum was fixed to the intact head of the pancreas anteriorly and posteriorly by interrupted nonabsorbable sutures beyond the ampulla. The head of the pancreas and the ampulla rested neatly within the jejunal C and this made the pancreaticojejunostomy easy to perform. Gastrointestinal continuity was restored by end-to-side gastrojejunostomy. Biliary decompression was achieved through a cholecystostomy. A feeding jejunostomy tube was placed distal to the gastrojejunostomy to decompress the pancreatico jejunostomy (Figure 3). A 16F portex tube drain was placed adjacent to the pancreatic-enteric anastomosis. In one patient (Case 2), a right nephrectomy was also performed as renal vessels were thrombosed.
Figure 2. Complex duodenal injury with extensive laceration.
Figure 3. Diagrammatic representation of the operative procedure.
One patient (Case 1) was re-explored 36 hours later for bleeding from the drain placed near the pancreas. There was diffuse ooze from the retroperitoneum. The anastomoses were intact.
Jejunostomy tube feeding was started after 5 days. An upper gastrointestinal gastrografin study ten days later revealed no anastomotic leak and the patients were then put on oral feeding.
A tube cholecystogram carried out 3 weeks later revealed a normal common bile duct and free flow of contrast into the jejunum (Figure 4). The Cholecystostomy tube was subsequently removed. The patients are well at the two-year follow-up with no symptoms; liver function tests are normal
Figure 4. Cholecystocholangiogram showing normal common bile duct and free flow of contrast into the jejunum.
DISCUSSION
The surgical management of duodenal injury is complex and options vary from external drainage to complex reconstruction procedures to pancreaticoduodenectomy. Each of these procedures has its own limitations. Primary repair is associated with high duodenum related morbidity [1]. Duodenal fistula rates range from 0 to 16.2% [17, 18], and the mortality rate ranges from 10% to 29% [2, 18]. The role of pyloric exclusion is controversial [1, 2, 7, 8]. Recent studies found no difference in morbidity or mortality rates in patients undergoing pyloric exclusion versus primary repair [8, 19]. Dubose et al. [4] (results from the National Trauma Data Bank) reported no statistically significant difference in mortality or occurrence of abdominal septic complications in those undergoing pyloric exclusion versus primary repair. They further reported that pyloric exclusion contributes to longer hospital stays and confers no survival or outcome benefit. Pancreaticoduodenectomy (PD) for trauma is a formidable procedure with the attendant risks of anastomosis to the undilated bile and pancreatic ducts and soft pancreas [13, 19].
PPTD has been introduced as an alternative to PD for familial adenomatous polyposis, benign villous tumours of the duodenum and isolated duodenal injury [14, 15, 16, 20, 21]. PPTD was introduced as an alternative to PD on the basis of lower morbidity and mortality rates [16]. In a study comparing PPTD with classical PD for patients with familial adenomatous polyposis, no clear advantage was reported as PPTD was not associated with lower morbidity and mortality rates [20]. Another recent study reported that the morbidity of PPTD is similar to PD, but PPTD preserves the whole pancreas and reduces the number of anastomoses [21]. Muller et al. [22] have reported that PPTD is a safe surgical procedure which avoids pancreatic head resection, and shows advantages over the pylorus preserving Whipple procedure. They reported a hospital mortality of 4.3% and a 30% morbidity rate after PPTD.
PPTD is a relatively new procedure for complex traumatic injury of the duodenum. Advantages of PPTD over classical PD include preservation of the entire pancreas and avoidance of anastomoses to undilated biliary and pancreatic ducts and the cut surface of a soft pancreas. Anastomosis in unfavorable situations is associated with a high risk of anastomotic leakage [23].Various methods of reconstruction following PPTD include anastomosis between the papilla and the small bowel, sphincteropapillotomy and an opened major papilla anastomosed to an opening in the small intestine [15] and no pancreatic enteric anastomosis [24]. We used the dunking procedure: the head of the pancreas was fixed with the jejunum by interrupted nonabsorbable sutures. The entire common bile duct and pancreatic duct were preserved. In the two patients reported, no morbidity resulted from PPTD.
Biliary diversion is a useful addition for the management of duodenal injuries [25]. Decompression via a quadruple tube technique to protect the duodenal repair is reported to reduce the risk of duodenal fistula [26]. Biliary diversion, in our study, was possibly helpful in protecting the pancreaticojejunostomy (PJ) in the immediate postoperative period by reducing the amount of bile entering the jejunum. A cholecystocholangiogram revealed adequate biliary drainage. Both patients are well on follow-up.
The role of prophylactic octreotide administration remains controversial. Though there are reports suggesting the use of prophylactic octreotide in pancreaticoduodenal injuries [27, 28], most of the studies have not mentioned its use in duodenal injuries [1, 3, 15, 19]. Moreover, the selective use of octreotide to prevent postoperative complications and mortality in patients undergoing pancreatic surgery also remains debatable [29, 30].
The ampulla was preserved in both of our patients and we did not institute external drainage of pancreatic duct with a stent. The use of a pancreatic duct stent for the drainage of pancreatic duct though an attractive strategy remains debatable: some report a reduced leakage rate [31], while others have not found it effective in significantly reducing the leak rate [32, 33].
CONCLUSION
The present report demonstrates the usefulness of PPTD for complex duodenal injury. PPTD is an organ preserving and problem-focused technique which avoids the hazards of anastomosing undilated bile and pancreatic ducts. The duodenum is removed and the entire pancreas is preserved. PPTD thus is a protective strategy which provides adequate treatment for complex duodenal injury and prevents duodenum and pancreas related morbidity.
Conflict of interest The authors have no potential conflict of interest
References
- Bozkurt B, Ozdemir BA, Kocer B, Unal B, Dolapci M, Cengiz O. Operative approach in traumatic injuries of the duodenum. Acta Chir Belg 2006; 106:405-8. [PMID 17017693]
- Jansen M, Du Toit DF, Warren BL. Duodenal injuries: surgical management adapted to circumstances. Injury 2002; 33:611-5. [PMID 12208065]
- Rathore MA, Andrabi SI, Najfi SM, Chaudhry Z, Chaudhry AM. Injuries to the duodenum--prognosis correlates with body Injury Severity Score: a prospective study. Int J Surg 2007; 5:388-93. [PMID 17613290]
- DuBose JJ, Inaba K, Teixeira PG, Shiflett A, Putty B, Green DJ, et al. Pyloric exclusion in the treatment of severe duodenal injuries: results from the National Trauma Data Bank. Am Surg 2008; 74:925- 9. [PMID 18942615]
- Eckert MJ, Perry JT, Sohn VY, Keylock JB, Munaretto JA, Beekley AC, Martin MJ. Bioprosthetic repair of complex duodenal injury in a porcine model. J Trauma 2009; 66:103-9. [PMID 19131812]
- Berne CJ, Donovan AJ, White EJ, Yellin AE. Duodenal "diverticulization" for duodenal and pancreatic injury. Am J Surg 1974;127:503-7. [PMID 4545015]
- Kashuk JL, Moore EE. Should pyloric exclusion for duodenal and pancreatico-duodenal injuries be abandoned? J Trauma 2007; 63:452-3. [PMID 17693855]
- Seamon MJ, Pieri PG, Fisher CA, Gaughan J, Santora TA, Pathak AS, et al. A ten-year retrospective review: does pyloric exclusion improve clinical outcome after penetrating duodenal and combined pancreaticoduodenal injuries? J Trauma 2007; 62:829-33. [PMID 17426536]
- Clendenon JN, Meyers RL, Nance ML, Scaife ER. Management of duodenal injuries in children. J Pediatr Surg 2004; 39:964-8. [PMID 15185235]
- Kawarada Y, Tani K, Yoshimine S, Mizumoto R. Blunt injury of duodenum with avulsion of papilla of Vater--report of a case. Jpn J Surg 1984; 14:499-504. [PMID 6530845]
- Cooke HS. Avulsion of the ampulla of Vater following blunt trauma. Aust N Z J Surg 1990; 60:393-6. [PMID 2334362]
- Degiannis E, Boffard K. Duodenal injuries. Br J Surg 2000; 87:1473-9. [PMID 11091233]
- Stawicki SP, Schwab CW. Pancreatic trauma: demographics, diagnosis, and management. Am Surg 2008; 74:1133-45. [PMID 19097525]
- Eisenberger CF, Knoefel WT, Peiper M, Yekebas EF, Hosch SB, Busch C, Izbicki JR. Pancreas-sparing duodenectomy in duodenal pathology: indications and results. Hepatogastroenterology 2004; 51:727-31. [PMID 15143902]
- Imamura M, Komoto I, Doi R, Onodera H, Kobayashi H, Kawai Y. New pancreas-preserving total duodenectomy technique. World J Surg 2005; 29:203-7. [PMID 15650799]
- Chung RS, Church JM, vanStolk R. Pancreas-sparing duodenectomy: indications, surgical technique, and results. Surgery 1995; 117:254-9. [PMID 7878529]
- Asensio JA, Demetriades D, Berne JD, Falabella A, Gomez H, Murray J, et al. A unified approach to the surgical exposure of pancreatic and duodenal injuries. Am J Surg 1997; 174:54-60. [PMID 9240953]
- Timaran CH, Martinez O, Ospina JA. Prognostic factors and management of civilian penetrating duodenal trauma. J Trauma 1999; 2:330-5. [PMID 10452469]
- Velmahos GC, Constantinou C, Kasotakis G. Safety of repair for severe duodenal injuries. World J Surg 2008; 32:7-12. [PMID 17952703]
- de Castro SM, van Eijck CH, Rutten JP, Dejong CH, van Goor H, Busch OR, Gouma DJ. Pancreas-preserving total duodenectomy versus standard pancreatoduodenectomy for patients with familial adenomatous polyposis and polyps in the duodenum. Br J Surg 2008; 95:1380-6. [PMID 18844249]
- Al-Sarireh B, Ghaneh P, Gardner-Thorpe J, Raraty M, Hartley M, Sutton R, Neoptolemos JP. Complications and follow-up after pancreas-preserving total duodenectomy for duodenal polyps. Br J Surg 2008; 95:1506-11. [PMID 18991295]
- M?ller MW, Dahmen R, K?ninger J, Michalski CW, Hinz U, Hartel M, et al. Is there an advantage in performing a pancreaspreserving total duodenectomy in duodenal adenomatosis? Am J Surg 2008; 195:741-8. [PMID 18436175]
- de Castro SM, Busch OR, van Gulik TM, Obertop H, Gouma DJ. Incidence and management of pancreatic leakage after pancreatoduodenectomy. Br J Surg 2005; 92:1117-23. [PMID 15931656]
- Koshariya M, Jagad RB, Kawamoto J, Papastratis P, Kefalourous H, Porfiris T, et al. Pancreas-preserving total duodenectomy without pancreato-enteric anastomosis. Hepatogastroenterology 2007; 54:2123-2128. [PMID 18251174]
- Leppaniemi A. Management of pancreatic and duodenal injuries. Lietuvos Chirurgija (Lithuanian Surgery )2007; 5:102-7.
- Crippa S, Falconi M, Bettini R, Barugola G, Germenia S, Salvia R, Pederzoli P. Isolated blunt duodenal trauma: delayed diagnosis and favorable outcome with "quadruple tube" decompression. JOP. J Pancreas (Online) 2007; 8:617-20. [PMID 17873470]
- Lochan R, Sen G, Barrett AM, Scott J, Charnley RM. Management strategies in isolated pancreatic trauma. J Hepatobiliary Panc Surg 2009; 16:189-96. [PMID 19214372]
- Ivanov PA, Grishin AV, Korneev DA, Ziniakov SA. Injuries of pancreatoduodenal organs. Khirurgiia (Mosk) 2003; 12:39-43. [PMID 14671603]
- Kollmar O, Moussavian MR, Richter S, de Roi P, Maurer CA, Schilling MK. Prophylactic octreotide and delayed gastric emptying after pancreaticoduodenectomy: results of a prospective randomized double-blinded placebo-controlled trial. Eur J Surg Oncol 2008; 34:868-75. [PMID 18299182]
- Alghamdi AA, Jawas AM, Hart RS. Use of octreotide for the prevention of pancreatic fistula after elective pancreatic surgery: a systematic review and meta-analysis. Can J Surg 2007; 50:459-66. [PMID 18053374]
- Poon RT, Fan ST, Lo CM, Ng KK, Yuen WK, Yeung C, Wong J. External drainage of pancreatic duct with a stent to reduce leakage rate of pancreaticojejunostomy after pancreaticoduodenectomy: a prospective randomized trial. Ann Surg 2007; 246:425-35. [PMID 17717446]
- Winter JM, Cameron JL, Campbell KA, Chang DC, Riall TS, Schulick RD, et al. Does pancreatic duct stenting decrease the rate of pancreatic fistula following pancreaticoduodenectomy? Results of a prospective randomized trial. J Gastrointest Surg 2006; 10:1280-90. [PMID 17114014]
- Kleespies A, Albertsmeier M, Obeidat F, Seeliger H, Jauch KW, Bruns CJ. The challenge of pancreatic anastomosis. Langenbecks Arch Surg 2008; 393:459-71. [PMID 18379817]





