Keywords
Dog-1 protein, C elegans; Interstitial Cells of Cajal; Pancreas
Abbreviations
CD: cluster of differentiation; CEA: carcinoembryonic antigen; CECT: contrast enhanced tomogram scan; CT: computerized tomogram scan; DOG-1: discovery on gastrointestinal stromal tumor 1; EGIST: extragastrointestinal stromal tumors; EUS: endoscopic ultrasound; FNA: fine needle aspiration; GANT: gastrointestinal autonomic nerve cell tumor; GIST: gastrointestinal stromal tumors; H&E: hematoxylin and eosin stain; HPF: high power field; MRI: magnetic resonance imaging; PDGFR-α: platelet derived growth factor-alfa; pEGIST: pancreatic extragastrointestinal stromal tumors; SMA: smooth muscle actin; US: ultrasonography; VEGF: vascular endothelial growth factor
INTRODUCTION
Santiago Raman y Cajal, a Spanish neurohistologist, described specialized “interstitial neurons” in tubular gut in the year 1892 by using light microscopy, for which he shared Nobel prize in Physiology or Medicine with Camillo Golgi in the year 1906 [1]. It was not until early 1970s, when light and electron microscopic studies by M.S. Faussone-Pellegrini et al. reaffirmed Cajal’s observations and renamed these “neuron like cells” as “interstitial cells of Cajal”. Since then, interstitial cells of Cajal has been a pacemaker symbol for gastrointestinal motility [2, 3]. Noteworthy is the fact, the cells, which are now named interstitial cells of Cajal, were stained for the first time by Cajal in 1892 with methylene blue.
The interstitial cells of Cajal continues to appeal morphologists for its specific light and electron microscopic characteristics, physiologists as pacemaker of the tubular gut, pathologists for the motility disorders and origin of gastrointestinal stromal tumors (GISTs), pharmacologists and oncologists for usage of imatinib mesylate and family of drugs that selectively block tyrosine kinase activity in GISTs, and the molecular biologists for specific mutations in GISTs which might influence the prognosis [4].
Gastrointestinal stromal tumors, first coined by Mazur and Clark in 1983, are the most common primary, non epithelial, mesenchymal tumors of the tubular gastrointestinal tract which arise from the interstitial cells of Cajal. These are the result of gain of function mutation of c-KIT (up to 90%) or platelet derived growth factor-alfa (PDGFR-α; 5 to 7%) protooncogenes leading to ligand independent activation of tyrosine kinase protein receptors in interstitial cells of Cajal and concomitant downstream activation of signal transduction pathways [4, 5, 6, 7]. Recently, discovery on gastrointestinal stromal tumor 1 (DOG-1, also called TMEM16A/FLJ10261/ORAOV2/anoctamin 1), a calcium regulated chloride channel protein, and protein kinase C theta (a signalling molecule in T-cell activation) have been shown to be the most specific diagnostic biomarker of GISTs, though ready availability is a major concern [8, 9, 10, 11].
The most common sites of GISTs are stomach (40- 70%), small intestine (20-40%), and rarely esophagus, colon, and rectum (less than 10%). A subset of GISTs arises from extragastrointestinal sites, most common being soft tissues of retroperitoneum, omentum and mesentery, and are categorized as extragastrointestinal stromal tumors (EGISTs) [12, 13, 14, 15]. While latter part of 20th century saw the “interstitial cells of Cajal cat walk” in the digestive tract, the first decade of 21st century has been devoted to the discovery and ultrastructural characterization of interstitial Cajal like cells in virtually every extragastrointestinal anatomic sites of the human body. Not surprisingly, EGISTs have been reported to arise from these sites [16, 17, 18, 19, 20, 21, 22, 23, 24]. Detailed light microscopic, transmission electron microscopy, and immunohistochemical studies have revolutionized the interstitial Cajal like cells research. Pioneers in this filed are the Bucharest team led by Laurentiu M Popescu and other co-workers [16, 25, 26, 27, 28]. With this, the quite established dogma “interstitial cells of Cajal: a pacemaker symbol confined exclusively to the cavitary organs like tubular gut’ has thus been overpassed!
Pancreas, a non cavitary parenchymal organ, is embryologically related to the tubular gut. However, unlike their gastrointestinal counterparts, pancreatic EGISTs (pEGISTs) are extremely rare and only sporadically reported in the world literature, with unpredictable biological behavior. The year 2004 was marked by the report of two cases of c-KIT positive stromal tumors in the pancreas: first by Yamaura et al. [29] from Japan and second by Neto et al. [30] from Brazil. In the following year, Popescu and co-workers described, for the first time, interstitial Cajal like cells in the rat and human exocrine pancreas (pancreatic interstitial Cajal like cells) by means of light microscopic, transmission electron microscopy, and immunohistochemistry studies [25, 26]. Since then, only 19 cases have so far been reported from around the world [29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47]. Hence, in the EGIST race, pancreas remains second only to the soft tissue as the site of this group of neoplasms. Since its first characterization in 2005, pancreatic interstitial Cajal like cells are frequently been re-explored by several researchers with newer concepts in terminologies, function, and their probable associated pathologies [16, 27, 28].
This manuscript summarizes all the reported cases of pEGISTs in regard to clinical characteristic, diagnostic modalities used, pathology, immunohistochemical characteristics, management, and outcome. Furthermore the recent developments in the field of pancreatic interstitial Cajal like cells are briefly discussed.
MATERIAL AND METHODS
The selection of case reports (January 2000 - September 2012) was done at random, based on key words ‘pancreatic GISTs’, ‘pancreatic EGISTs’, ‘pancreatic interstitial cells of Cajal’ using the search engine of PubMed, PubMed Central, Google Scholar, and the Directory of Open Access Journals. Fischer exact test was employed to measure the statistical significance of different parameters for prognostication
RESULTS
The clinical presentation, imaging modalities used for their characterization, management, pathology, and follow-up data of reported cases of pEGIST are summarized in Tables 1 to 5.
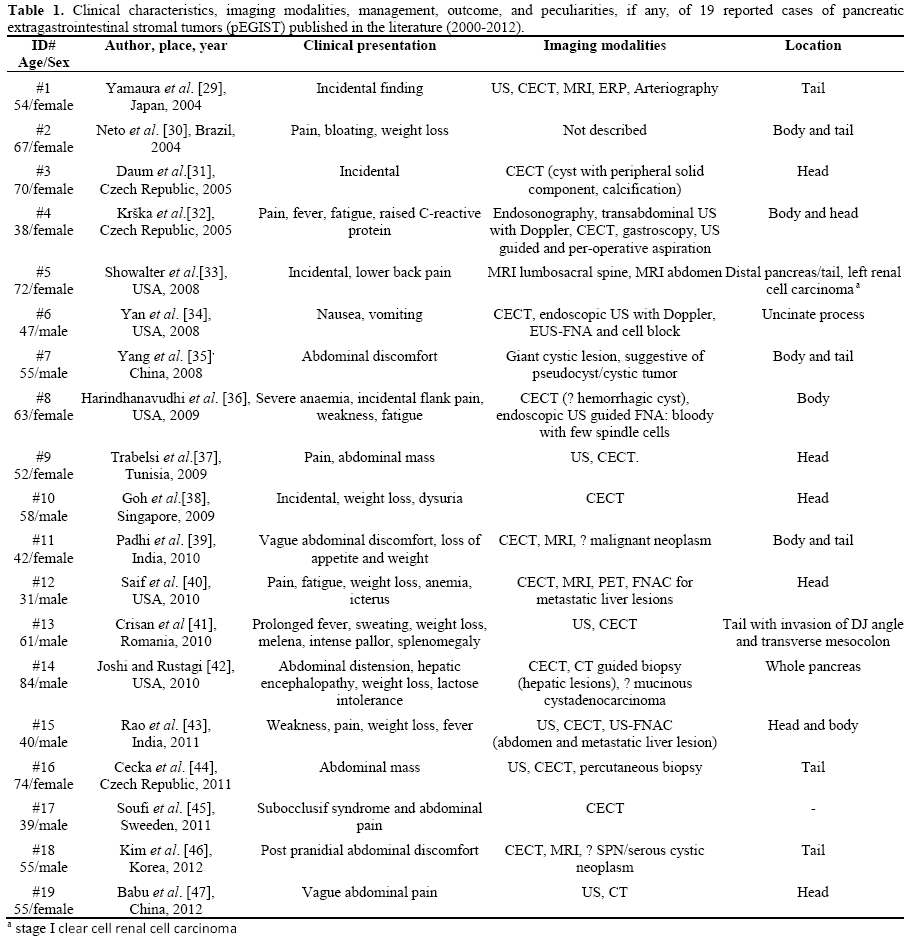
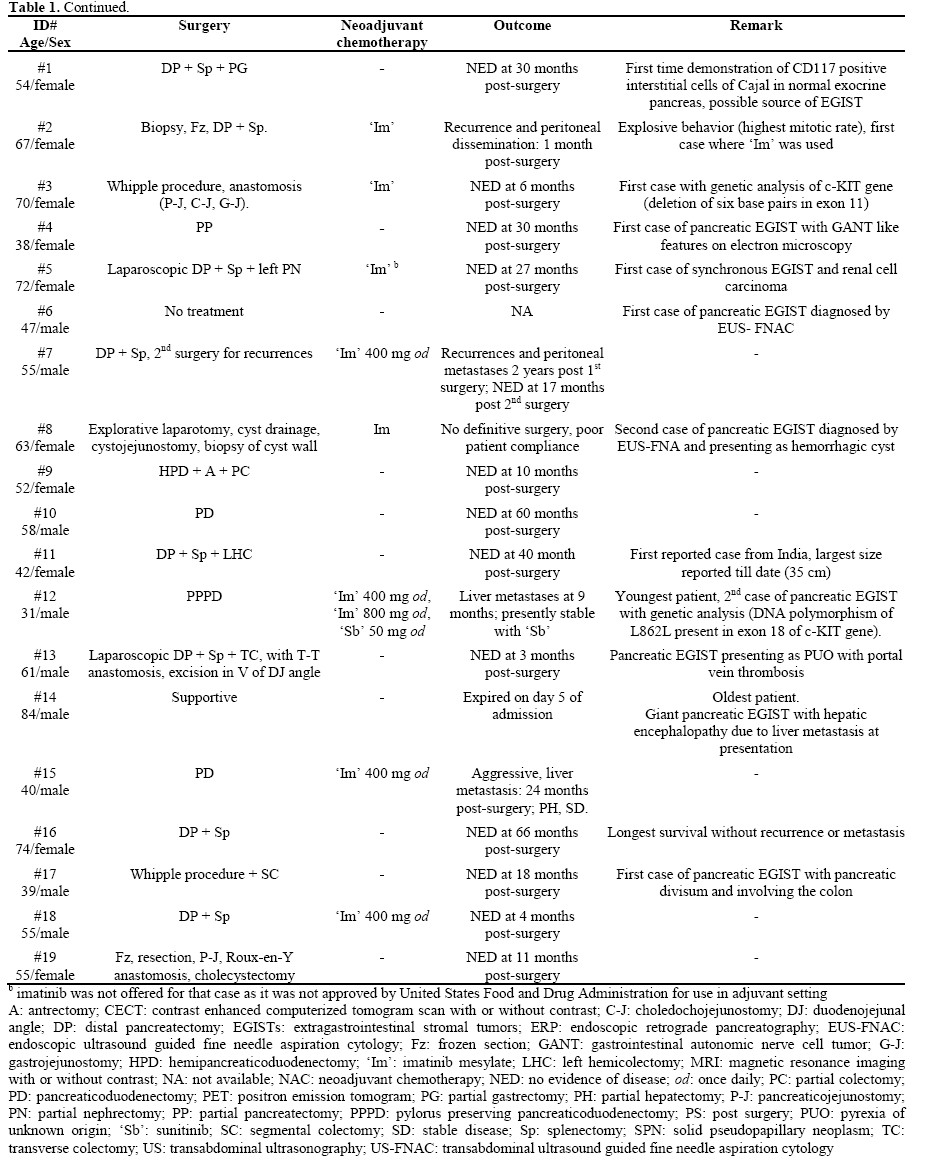
Clinical Presentation (Tables 1 and 2)
Most patients with gastrointestinal stromal tumors (GISTs) are older than 50 years at first presentation, though syndromic GISTs may occur in younger age group. Vague abdominal discomfort/pain is the most common symptom followed, next in frequency, by anemia secondary to gastrointestinal mucosal ulceration and/or intratumoral hemorrhage [7]. In this context, the gender predilection for pEGIST has been equal (male:female ratio: 9:10) with an age range of 31 to 84 years (mean: 55.6 years). Thirteen of 19 (68.5%) patients (5 males, 8 females) were older than 50 years of age at first presentation, whereas 6/19 (31.5%) (4 males, 2 females) were under the age of 50 years. Seventy-nine percent (15/19) patients were symptomatic at first presentation with pain abdomen/discomfort (n=11, 57.9%), weight loss/fatigue (n=8, 42.1), and abdominal distension (n=4, 21.1%) constituting the three most common symptoms/signs.
The spectrum of diseases causing fever of unknown origin has shown a significant change over years. Although infections still remain the most common cause, the incidence of non infectious etiologies seems to have increased in recent years. With the advent of advanced imaging modalities, more number of cases of fever of unknown origin attributable to underlying malignancies has been on rise. A recent multicenter study [48] analyzed 154 patients with fever of unknown origin and in 22 (14.3%), it was attributed to an underlying malignancy. Rarely, stromal tumor and pancreatic carcinoma were reported to be the underlying pathology (1 patient each). Crisan et al. [42] described a unique case of EGIST arising from the tail of the pancreas which was characterized by prolonged fever (as a dominant presentation) secondary to portal vein and inferior vena cava thrombosis, whereas in few others [31, 43] it occurred as a part of inflammatory syndrome characterized by raised Creactive protein and erythrocyte sedimentation rate. Joshi and Rustagi [41], described a fatal case of pEGIST in an 84-year-old male who presented with markedly distended abdomen, worsening mental confusion, jaundice, elevated levels of blood ammonia, and liver transaminases suggestive of hepatic encephalopathy which was secondary to liver metastasis, a feature rarely reported in GIST/EGIST. Soufi et al. [45] described another unusual case pEGIST associated with pancreatic divisum (a developmental anomaly of pancreas) presenting with subocclusive syndrome and involving the colon.
Renal Cell Carcinoma and GIST
Synchronous occurrence of GIST with a tumor of different histogenesis is thought be rare [49]. GIST and papillary renal cell carcinoma may occur as recurrent familial tumors related to mutations in the protooncogenes, c-MET and c-KIT (both of which are tyrosine kinase receptor molecules), suggesting a common co-regulatory mechanism. It has been postulated that antecedent use of Gleevec® (imatinib mesylate) for prior GIST may be a potential risk factor for development of secondary papillary renal cell carcinoma [50, 51]. On the other hand, there have been sporadic reports of clear cell renal cell carcinoma associated with GIST [52, 53]. Showalter et al. [33] described for the first time, and the only of such kind till date, the occurrence of synchronous clear cell renal cell carcinoma (left side, stage I) and pEGIST in an elderly Afro-American female, though no genetic testing was done till last follow-up.
Imaging Characteristics (Tables 1 and 2)
The accuracy of computerized tomogram (CT) imaging to predict a malignant vs. benign cystic lesion of the pancreas ranges between 76% and 82%. The accuracy of CT determination of the histopathological diagnosis of a pancreatic cystic lesion is less than 50% [54, 55]. Contrast enhanced abdominal computerized tomogram (CECT: 16/19, 84.2%), magnetic resonance imaging (MRI T1 and T2W: 5/19, 26.3%), transabdominal ultrasonography (US: 7/19, 36.8%), and endoscopic US (EUS: 3/19, 15.8%) [34, 37] with or without Doppler were used to localize, characterize, and delineate the tumors, for pre-operative fine needle aspiration (FNA) for diagnosis [34, 37, 43], and characterizing the associated pathology. Eight of 19 (42.1%) tumors occurred in the head of pancreas, 5 in tail (26.3%), 4 involved both body and tail (21.1%) and one occurred in the uncinate process (5.3%). Rarely (n=1, 5.3%) they did involve the entire pancreas [41]. The tumors ranged from few incidental masses to huge masses fulfilling the entire abdominal cavity. In most, the lesions were lobulated and showed heterogeneous enhancement in CECT and MRI with contrast (both solid and cystic/hemorrhagic). Padhi et al. [39] described the largest pEGIST (35x30x25 cm) which was hypointense in T1W MRI, hyperintense (cystic) with heterogeneous enhancement in T2W MRI (hemorrhagic and calcific foci) (Figure 1a-d). The lesions also showed variable vascularity with arterial phase enhancement of solid component [29, 34, 38, 39, 40]. The US features were that of predominantly hypoechoic (cystic/hemorrhagic/fluid like/? necrotic) masses with focal hyperechogenicities (? calcifications). However, in none there was any radiologic evidence of communication with or abnormality of major and/or minor pancreatic duct or bile duct, a feature supposed to be against the possibility of ductal adenocarcinoma [55]. Furthermore, in none tumor markers (CA 19-9 and carcinoembryonic antigen (CEA)) were found to be elevated, a finding that corroborated with the radiological findings.
Endoscopic US guided FNA (EUS-FNA) plays an important role in the diagnosis of pancreatic cystic lesions. Successful diagnosis of pancreatic lesions via FNA depends on the adequacy of the specimen. FNA of a solid mass has higher accuracy rate compared to a cystic lesion [54]. Besides this, EUS has been a sensitive tool in delineating the tumors arising from pancreatic head and/or the adjacent duodenal wall [34, 35]. Yan et al. [34] reported the first case of pEGIST involving the uncinate process diagnosed by EUSFNA. Harindhanavudhi et al. [37] reported the first case of EGIST in the body of pancreas, which presented with hemorrhagic cyst diagnosed by EUSguided FNA.
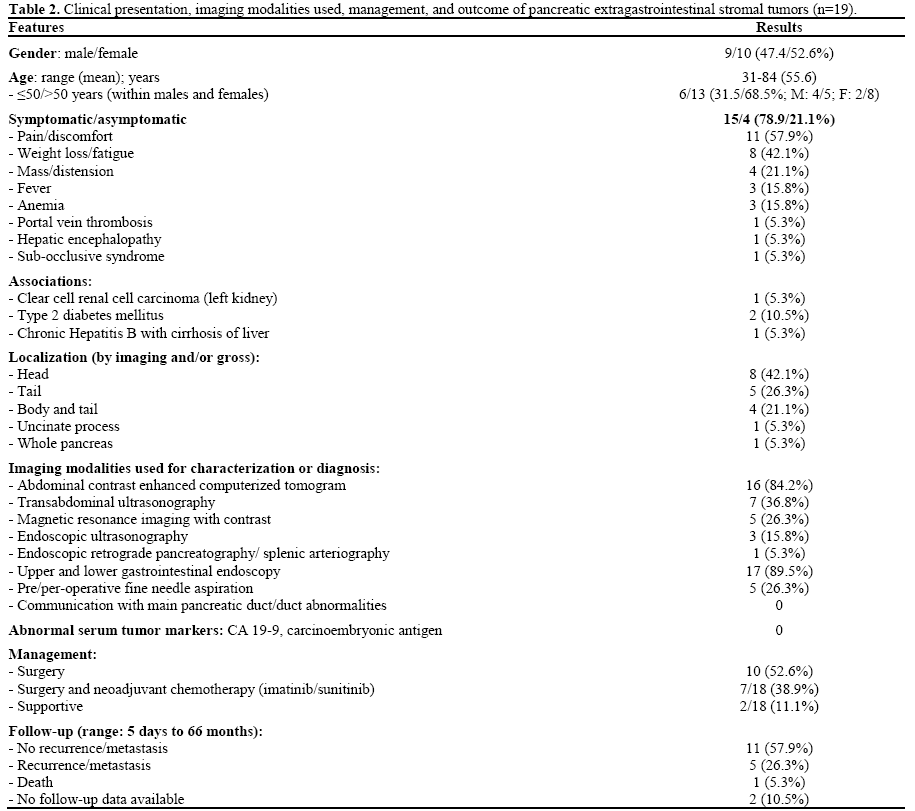
Gross and Microscopic Pathology (Table 3, Figure 2ab, Figure 3a-d)
On gross evaluation, the tumors ranged from 2.4 cm to 35 cm with mean size of 14 cm. Twelve (63.2%) of 19 were larger than 10 cm (hence high risk category) [56] of which 8 occurred in females. Gross morphology was described in 17 cases. Majority (12, 70.6%) were purely or predominantly solid with focal cystic components, 3 (17.6%) were predominantly cystic with peripheral solid areas, and 2 (11.8%) were entirely cystic, whereas areas of hemorrhage and/or necrosis were additionally present in 4 out of 19 cases (21.1%). In only two cases (10.5%), presence of peripheral compressed pancreatic tissue was described. Rest it was not. The lesions simulated solid pseudopapillary neoplasm in one (5.2%), malignant cystic epithelial neoplasm in 3 (15.8%; 2 serous, 1 mucinous), and ductal adenocarcinoma in rest (15/19, 78.9%).
On hematoxylin and eosin (H&E) stained tissue sections, the tumors showed variable cellularity comprising exclusively or predominantly of fusiform/spindled cells in short intersecting fascicles and focal storiform pattern (most common; 13/19, 68.4%) resembling a smooth muscle tumor, whereas six tumors (31.6%) demonstrated variable admixture of spindled and epithelioid stromal cells, simulating sarcomatoid carcinoma. In 7 (36.8%), the lesions were characterized by foci of perivascular hyalinization and/or nuclear pallisading reminiscent of a neural tumor. Areas of myxoid degeneration, cyst formation, and hemorrhage were observed in 5 cases (26.3%), coagulative necrosis in 4 (21.1%), whereas 3 tumors (15.8%) exhibited moderate to marked nuclear pleomorphism. Infiltration of tumor cells with mast cells (Giemsa stain) and inflammatory cells were noted in 5 (26.3%), thus simulating inflammatory pseudotumor (myofibroblastic tumor). In contrast to gastrointestinal counterparts, pure epithelioid morphology (so called leiomyoblastomas) and Skenoid fibers were not seen in any of the pEGIST. Using threshold values of 2 mitotic figures/50 high power field (HPF), 11/15 (73.3%) showed more than 2 mitotic figures/50 HPF, whereas 4/15 (26.7%) had 2/50 HPF or less, and in rest (4/19, 21.1%) the mitotic activity was not described.
Immunohistochemical Characteristics (Table 4, Figures 4ab)
Diagnosis of GISTs/EGISTs relies heavily on the c- KIT/CD117 immunohistochemistry staining, which can detect these tumors in most cases (up to 95%), making this antigen the most sensitive and specific means of confirming the diagnosis. Approximately 5% of GISTs are c-KIT negative and harbor PDGFR-α mutation, thus suggesting an alternate pathway of carcinogenesis [4, 5, 6].
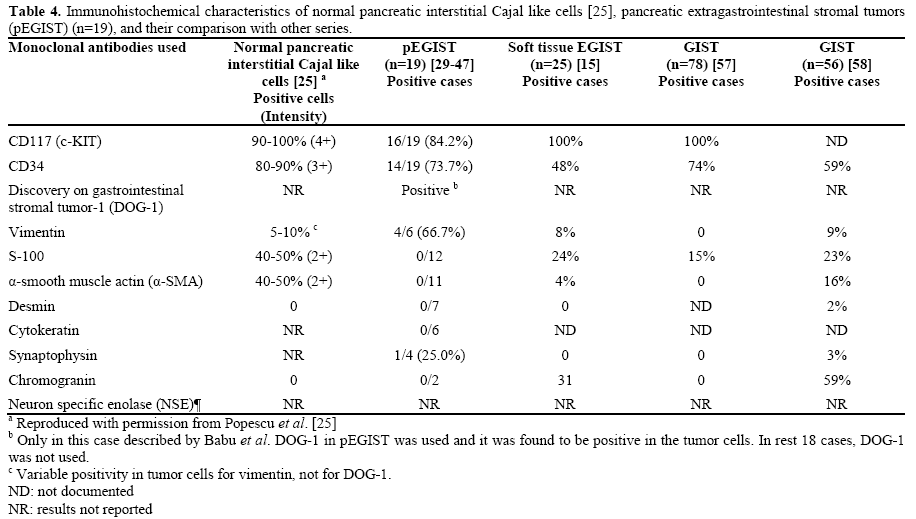
Immunohistochemistry findings in pEGISTs closely resembled those of resident pancreatic interstitial cells of Cajal as described by Popescu et al. [25] and GISTs arising from other anatomic sites. Sixteen of 19 (84.2%) pEGISTs showed strong diffuse cytoplasmic positivity for CD117/c-KIT, and 14/19 (73.7%) were positive for CD34, thus making these two as most sensitive marker at this site. The tumor cells were consistently negative for S-100 (12/12), α-smooth muscle actin (SMA, 11/11), desmin (7/7), cytokeratin (6/6), and chromogranin (2/2), a feature in contrast to other studies [15, 57, 58]. Babu et al. [47] recently described a case of DOG-1 positive pEGIST. Krska et al. [31] described a case of pEGIST which showed positivity for synaptophysin and gastrointestinal autonomic nerve cell tumor (GANT) like features in transmission electron microscopy studies. Positivity for neuronal markers like neuron specific enolase has been reported from GISTs involving different anatomic sites [15, 58].
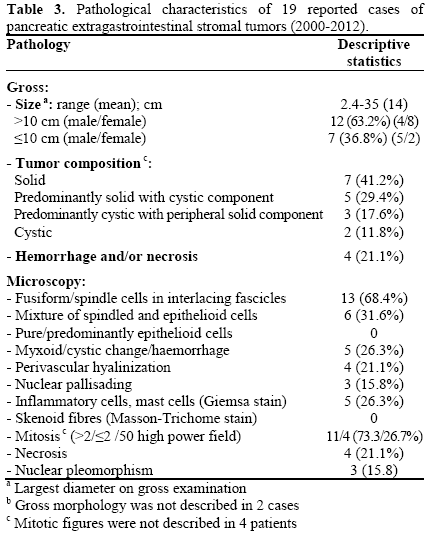
Biological Behavior and Management (Tables 1 and 5)
The biological behavior of GISTs may be unpredictable and depends upon several parameters. A small number of GISTs recur or metastasize despite a histologically benign appearance (i.e., small size and absence of mitoses or low mitotic rate), and large tumor size may not imply early recurrence [55, 59]. Tumors with high cellularity, as defined by frequent areas with overlapping nuclei, mitoses, and necrosis, have been associated with a statistically higher risk of adverse outcome in several studies of both GISTs and EGISTs. The threshold level of mitotic count for adverse outcome has been as low as 2 mitoses/50 HPF in duodenum to as high as greater than 10 mitoses/50 HPF in the stomach (100% metastasis) [12]. In another study involving soft tissue EGISTs [15], cellularity (high versus low), mitosis (<2 or >2 mitoses/50 HPF), and necrosis (present or absent) were found to be important predictor (P<0.001) of an adverse outcome (recurrence/metastasis/death due to tumor) in univariate analysis, whereas only mitosis and necrosis were independent predictors of adverse outcome in multivariate analysis.
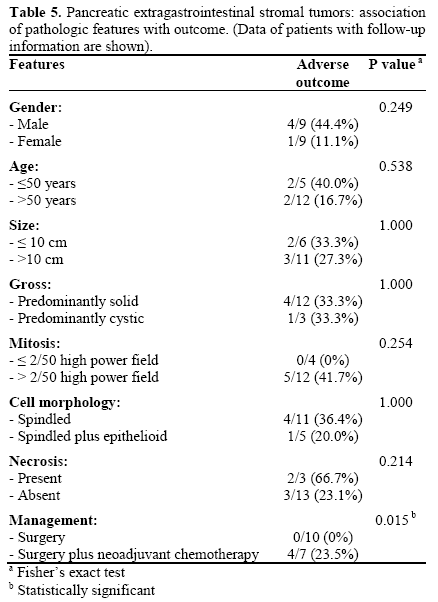
Surgical resection with a negative microscopic resection margin (R0 resection) is the primary mode of management in GIST. The surgical management may be of three types such as primary surgery (at the time of diagnosis), with neoadjuvant chemotherapy, or debulking type in patients with metastatic or advanced disease. Rapid advances in targeted therapies (imatinib, sunitinib, nilotinib, sorafenib, dovitinib, etc) in GIST have dramatically improved the post-operative relapse free survival and are currently advocated in those with R1 (positive microscopic margin) or R2 (gross visible tumor left behind) resection. Observation only is all that recommended in case of R0 resection [60]. Surgery with R0 resection has been the mainstay of management in pEGIST (11/19, 57.9%), whereas 6 patients (31.6%) received surgery with neoadjuvant imatinib, and one (5.3%) received neoadjuvant imatinib and sunitinib following surgery. In one patient of synchronous renal cell carcinoma and pEGIST [33], imatinib was not used as it was not approved by United States Food and Drug Administration for use in neoadjuvant setting at that time. The follow-up period ranged from 5 days to 66 months [41, 44], and 57.9% (11/19) had favorable outcome (no recurrence or metastasis), 5 (26.3%) presented with recurrence and/or metastasis, and only one patient (5.3%) had a fatal outcome. By univariate analysis, none of the clinical and pathological parameters except surgical management (R0 resection) (P<0.05) were found to be important indicator of outcome in these tumors.
PANCREATIC INTERSTITIAL CAJAL LIKE CELLS/TELOCYTES
Yamaura et al. [29] demonstrated, for the first time, the presence of CD117/c-KIT positive interstitial cells in human exocrine pancreas which did not stain for methylene blue. These were speculated to be the possible cell of origin of EGIST at this site. In a landmark discovery, Popescu and his Bucharest team [25] described, for the first time, peculiar interstitial cells in human and rat exocrine pancreas by using routine light microscopy (H&E, methylene blue; Figure 5a), non conventional light microscopy (toludine blue stained epon-embedded semi thin sections, less than 1 μm; Figure 5bc), transmission electron microscopy (semi thin sections; Figure 6ab), and immunohistochemistry (Figure 7a-d). These cells were morphologically and immunophenotypically distinct from other interstitial cells like fibroblasts, fibrocytes, neurons, or any other mesenchymal cells, rather had phenotypic characteristics of the canonical enteric interstitial cells of Cajal. These cells which were named as pancreatic interstitial Cajal like cells are now called as “telocytes”.
By nonconventional microscopy (toludine blue) and transmission electron microscopy studies (Figures 5 and 6), these cells represent a significant proportion of cellular microenvironment in the pancreas (3.3±0.5%; ß-cells, 1-2%), and show a close spatial relationship to capillaries (43%), acini and ductules (40%), stellate cells (14%), nerve fibres (3%), but unrelated to the endocrine microenvironment. These are characterized by a fusiform/pyriform/triangular cell body with 2 to 3 (most common; 88%), extremely long (20-50-100 μm), thin (less than 0.5 μm), dichotomously branched, cytoplasmic processes (telopods) with a moniliform aspect (many dilatations along), caveoli, and numerous mitochondria (8.7±0.8% of cytoplasm). Such lengths of cytoplasmic processes are unusual outside the nervous system, which readily differentiates such cells from other interstitial cells, and thus are considered “ultrastructural hallmark” of telocytes. By transmission electron microscopy studies, pancreatic interstitial Cajal like cells/telocytes satisfies majority of the ‘gold standard’ electron microscopic criteria of prototypical interstitial cells of Cajal [61].
Furthermore, these cells on immunohistochemistry studies have also shown strong positive staining with CD117 and CD34 (90-100%), variable (40-50%) positivity for α-SMA and S-100, rarely for CD68 and vimentin, and negative staining for desmin and chromogranin [25, 26].
FUTURE PERSPECTIVE
The exact physiologic function of pancreatic telocytes remains to be fully elucidated. Possible role in pancreatic morphogenesis during the embryonic life is suggested. A dynamic interaction with acinar, vascular, or sensorineural structures in a paracrine fashion seems plausible. Close association and interaction with pancreatic stellate cells in a juxtacrine fashion may be another mechanism leading to abnormal matrix deposition in pancreatic fibrosis. Though the pacemaker function in the exocrine pancreas is largely unknown, recent studies have also suggested the contrary [16, 25, 26, 27, 28]. Recent studies have also found that telocytes share the expression of several markers with GISTs and perivascular epitheloid cell tumors such as Melan A, CD117, CD63, CD34, SMA, S-100, and vascular endothelial growth factor (VEGF), thus suggesting a common histogenetic origin for these two group of tumors [62]. Possible role in pancreatic ßcell development and function has also been suggested by researchers [63].
Studies involving the utility of DOG-1 (specific biomarker of GIST) in normal pancreas have been contradictory as well as incomplete. DOG-1 expression in pEGIST has been described by Babu et al. [47]. In one study [64], the normal pancreatic tissues showed a distinct positivity confined to the endocrine component close to insulin secreting ß-cells. The location and pattern of DOG-1 expression (granular positivity) in pancreatic islets was similar to neuroendocrine markers like chromogranin A, PGP9.5, and synaptophysin. DOG-1 positivity in fetal and adult pancreatic islets suggests the strong antibody affinity for neuroendocrine cells. Another study [65], showed DOG-1 positivity in the centroacinar cells (exocrine component) and in solid cystic pseudopapillary neoplasms of the pancreas, thus suggesting a novel histogenetic relationship. Therefore, utility of DOG-1 as a GIST marker in pancreas has to be confirmed by large number of prospective studies dealing with neuroendocrine tumors, solid cystic pseudopapillary neoplasms, and CD117 positive stromal tumors.
Mutation in c-KIT exons 11 (most common), 9 (second most common), 13, 17, and PDGFR-α mutations in exons 12, 14, 18 are responsible for GIST carcinogenesis. Mutations in exon 9 and 13 are associated with poorer clinical outcome with more aggressive metastatic behavior. GISTs with missense mutation at exon 11 behave favorably in gastric but not in small intestinal tumors [4]. The molecular biology of pEGIST has been partially elucidated in only two cases [32, 40]. Daum et al. [32] demonstrated, for the first time, deletion of six base pairs in exon 11 of c-KIT gene in their case with a favorable outcome, whereas the case reported by Saif et al. [40] exhibited DNA polymorphism of L862L in exon 18 of c-KIT gene in another which presented with hepatic metastasis. In rest of the cases, genetic testing was not done.
CONCLUSION
With the discovery and characterization of pancreatic telocytes, the origin of stromal tumors reminiscent of GIST seems a real possibility. Though biologically heterogeneous, majority have been amenable to surgical resection, thus conferring a favorable prognosis. Although rare, pEGISTs should be considered as a differential diagnosis of stromal neoplasm in the pancreas. Analysis of a large number of such tumors with genetic analysis of c-KIT protooncogene will probably throw more light on their true nature and biology.
Acknowledgement
The authors sincerely acknowledge the immense help and support extended by none other than Dr Laurentiu M Popescu (Honourable Editor-in- Chief, Journal of Cellular and Molecular Medicine), and his co-workers from the Department of Cellular and Molecular Medicine, “Carol Davila” University of Medicine and Pharmacy, and “Victor Babes” National Institute of Pathology, Bucharest, Romania, and Dr Gianni Bussolati from the Department of Biomedical Sciences and Human Oncology, University of Turin, Turin, Italy for enlightening us with pancreatic interstitial Cajal like cells, telocytes, and allowing to use some of the photographs in this manuscript. The authors are also thankful to Dr Nateshan Bhumika, formerly Assistant Professor, Department of Community and Family Medicine, Pondicherry Institute of Medical Sciences, Puducherry, India for the statistical assistance
Conflict of interest
Nil
Financial support
Nil
References
- Ramon y Cajal S. Histologie du SystemeNerveux de L’Hommeet des Vertebres. Volume 2. Paris: A. Maloine; 1911.
- FaussonePellegrini MS, Cortesini C, Romagnoli P. Ultrastructure of the tunica muscularis of the cardial portion of the human esophagus and stomach, with special reference to the so called Cajal’s interstitial cells. Arch ItalAnatEmbriol. 1977; 82: 157-77.[PMID: 613989]
- Faussone-Pellegrini MS, Thuneberg L. Guide to the identification of interstitial cells of Cajal. Microsc Res Tech 1999; 47: 248-66.[PMID: 10602286]
- Miettinen M and Lasota J. Gastrointestinal stromal tumors: review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch Pathol Lab Med 2006; 130:1466-78. [ PMID:17090188]
- Tan CB, Zhi W, Shahzad G, Mustacchia P. Gastrointestinal Stromal Tumors: A Review of Case Reports, Diagnosis, Treatment, and Future Directions. ISRN Gastroenterol 2012, Article ID 595968, 1-16, doi:10.5402/2012/595968.
- Laurini JA and Carter JE. Gastrointestinal stromal tumors: a review of the literature. Arch Pathol Lab Med 2010; 134:134-41. [PMID: 20073618]
- Levy AD, Remotti HE, Thompson WM, Sobin LH, Miettinen M. Gastrointestinal stromal tumors: radiologic features and pathologic correlation. Radio Graphics 2003; 23:283-304. doi: 10.1148/rg.232025146
- Miettinen M, Wang ZF, Lasota J. DOG1 antibody in the differential diagnosis of gastrointestinal stromal tumors: a study of 1840 cases. Am J Surg Pathol 2009; 33:1401-8. [PMID:19606013]
- West RB, Corless CL, Chen X, Rubin BP, Subramanian S, Montgomery K, Zhu S, et al. The novel marker, DOG-1, is expressed ubiquitously in gastrointestinal stromal tumors irrespective of KIT or PDGFR mutation status. Am J Pathol 2004; 165:107-13.[ PMID: 15215166]
- Sun X-W, Feng Z-J, Huang P, Hao W, Sui X-L. Expression of DOG1, CD117 and PDGFRA in Gastrointestinal Stromal Tumors and Correlations with Clinicopathology. Asian Pacific J Cancer Prev, 2012; 13:1389-1393. [PMID: 22799337]
- Blay P, Astudillo A, Buesa JM, Campo E, Abad M, Garcia- Garcia J, Miquel R, et al. Protein kinase C theta is highly expressed in gastrointestinal stromal tumors but not in other mesenchymalneoplasias. Clin Cancer Res 2004; 10:4089-95. [PMID: 15217944]
- Weiss SW, Goldblum JR. Extra gastrointestinal stromal tumors. In: Enzinger and Weiss's Soft Tissue Tumors; fifth edition. Mosby Elesevier, 2008; 565-79. [ISBN 978-0-323-04628-2]
- Aigaimy A, Wunsch PH. Gastrointestinal stromal tumors: a regular origin in the muscularispropria, but an extremely diverse gross presentation (a review of 200 cases to critically revaluate the concept of so- called extragastrointestinal stromal tumors). Langenbacks Arch Surg 2006; 391:322-9. [PMID: 16402273]
- Miettinen M, Sobin LH, Lasota J. Gastrointestinal stromal tumors presenting as omental masses—a clinicopathologic analysis of 95 cases. Am J Surg Pathol 2009; 33:1267-75. [PMID: 19440146]
- Rieth JD, Goldblum JR, Lyles RH, Weiss SW. Extragastrointestinal (soft tissue) stromal tumors: an analysis of 48 cases with emphasis on histologic predictors of outcome. Mod Pathol 2000; 13:577-85. [PMID: 10824931]
- Popescu LM and Faussone-Pellegrini MS. TELOCYTES – a case of serendipity: the winding way from Interstitial Cells of Cajal (ICC), via Interstitial Cajal-Like Cells (ICLC) to TELOCYTES. J Cell Mol Med 2010; 14 (4):729-40. [PMID: 20367664]
- Bussolati G. Of GISTs and EGISTs, ICCs and ICs. Virchows Arch. 2005; 447:907-8. [Epub 2005 Sep 21].
- Hinescu ME, Ardeleanu C, Gherghiceanu M, Popescu LM. Interstitial Cajal like cells in human gallbladder. J Mol Histol 2007; 38:275-84. [PMID: 17541711]
- Rasmussen H, Rumessen JJ, Hansen A, Smedts F, Horn T. Ultrastructure of Cajal-like interstitial cells in the human detrusor. Cell Tissue Res 2009; 335:517-27. [PMID: 19142665]
- Ahmadi O, de L Nicholson M, Gould ML, Mitchell A, Stringer MD. Interstitial cells of Cajal are present in human extrahepatic bile ducts. J Gastroenterol Hepatol. 2010; 25:277-85. [PMID: 19793166]
- Long KB, Butrynski JE, Blank SD, Ebrahim KS, Dressel DM, Heinrich MC, et al. Primary extragastrointestinal stromal tumor of the pleura: report of a unique case with genetic confirmation. Am J Surg Pathol 2010; 34:907-12. [PMID: 20442644]
- Petrou A, Alexandrou P, Papalambros A, Saetta A, Fragkou P, Kontos M, et al. A malignant gastrointestinal stromal tumor of the gall bladder immunoreactive for PDGFRA and negative for CD117 (c-KIT). HPB Surgery 2011; Article ID 327192, doi:10.1155/2011/327192.
- Terada T. Gastrointestinal stromal tumor of the uterus: a case report with genetic analyses of c-kit and PDGFRA genes. Int J Gynecol Pathol 2009; 28:29-34. [PMID: 19047911]
- Luo XL, Liu D, Yang JJ, Zheng MW, Zhang J, and Zhou XD. Primary gastrointestinal stromal tumor of the liver: a case report. World J Gastroenterol 2009; 15 (15):3704-7. [PMID: 19653356]
- Popescu LM, Hinescu ME, Ionescu N, Ciontea SM, Cretoiu D, Ardelean C. Interstitial cells of Cajal in pancreas. J Cell Mol Med 2005; 9:169-90. [PMID: 15784175]
- Popescu L, Hinescu M, Radu E, et al. CD117/c-kit positive interstitial (Cajal-like) cells in human pancreas. J Cell Mol Med 2005; 9: 738-9. [PMID: 15963268]
- Nicolescu MI and Popescu LM. Telocytes in the interstitium of human exocrine pancreas: ultrastructural evidence. Pancreas 2012 Aug; 41(6):949-56. [PMID: 22318257]
- Wang XY, Diamant NE, Huizinga JD. Interstitial cells of Cajal: pacemaker cells of the pancreatic duct? Pancreas 2011; 40(1):137-43. [PMID: 21160371]
- Yamaura K, Kato K, Miyazawa M, Haba Y, Muramatsu A, Miyata K, Koide N. Stromal tumor of the pancreas with expression of c-kit protein: report of a case. J Gastroenterol Hepatol 2004; 19:467-70. [PMID 15012791]
- Neto MR, Machuca TN, Pinho RV, Yuasa LD, Bleggi-Torres LF. Gastrointestinal stromal tumor: report of two unusual cases. Virchows Arch 2004; 444:594-6. [PMID 15118853]
- Krska Z, Pesková M, Povýsil C, Horejs J, Sedlýcková E, Kudrnová Z. GIST of pancreas. Prague Med Rep 2005; 106:201-8. [PMID 16315768]
- Daum O, Klecka J, Ferda J, Treska V, Vanecek T, Sima R, et al. Gastrointestinal stromal tumor of the pancreas: Case report with documentation of KIT gene mutation. Virchows Arch 2005; 446:470-2. [PMID 15756592]
- Showalter SL, Lloyd JM, Glassman DT, Berger AC. Extragastrointestinal stromal tumor of the pancreas: case report and a review of the literature. Arch Surg 2008; 143:305-8. [PMID 18347279]
- Yan B M, Pai R K, Dam J V. Diagnosis of pancreatic gastrointestinal stromal tumor by EUS guided FNA. JOP. J Pancreas (Online) 2008; 9:192-6. [PMID 18326928]
- Yang F, Long J, Di Y, Fu DL, Jin C, Ni QX, Zhu HG. A giant cystic lesion in the left epigastric region. Pancreatic malignant gastrointestinal stromal tumour (GIST).Gut 2008; 57:1494-1636. [PMID: 18941004]
- Goh BK, Kesavan SM, Wonk WK. An unusual cause of pancreatic head tumor. Gastroenterol 2009; 137; e5-e6.
- Harindhanavudhi T, Tanawuttiwat T, Pyle J, Silva R. Extra- Gastrointestinal Stromal Tumor Presenting as Hemorrhagic Pancreatic Cyst Diagnosed by EUS-FNA. JOP. J Pancreas (Online) 2009; 10:189-91. [PMID 19287116]
- Trabelsi A, Yacoub-Abid L B, Mtimet A, Ben Abdelkrim S, Hammedi F, Ben Ali A, Mokni M. Gastrointestinal stromal tumor of the pancreas: A case report and review of the literature. North Am J Med Sci 2009; 1:324-6. [PMID: 22666718]
- Padhi S, Kongara R, Uppin SG, Uppin MS, Prayaga AK, Sundaram C, Nagari B, and Shastry AR. Extragastrointestinal Stromal Tumor Arising in the Pancreas: A Case Report with a Review of the Literature. JOP. J Pancreas (Online) 2010; 11(3):244- 8. [PMID: 20442520]
- Saif MW, Hotchkiss S, Kaley K. Gastrointestinal stromal tumors of the pancreas. JOP. J Pancreas (online) 2010; 11(4):405-406. [PMID: 20601822]
- Joshi J and Rustagi T. Pancreatic extragastrointestinal stromal tumor: An unusual presentation of a rare diagnosis. Gastrointest Cancer Res 2010; Suppl 1:S29-S30, Abstr 0917 [PMCID: PMC3047023].
- Crisan A, Nicoara E, Cucui V, Cornea G, Laza R. Prolonged fever associated with gastrointestinal stromal tumor-case report. J Exp Med Surg Res 2010; 17 (3):219-224.
- Rao RW, Vij M, Singla N, and Kumar A. Malignant pancreatic extra-gastrointestinal stromal tumor diagnosed by ultrasound guided fine needle aspiration cytology. A case report with a review of the literature. JOP. J Pancreas (online) 2011; 12(3):283-86.
- Cecka F, John B, Ferko A, Subrt Z, Nikoliv DH, Tycova V. Long term survival of a patient after resection of a gastrointestinal stromal tumor arising from the pancreas. Hepatobiliary Pancreat Dis Int 2011; 10:330-332. [PMID: 21669581]
- Soufi M, Bouziane M, Kharrasse G, Bouziane C. An unusual case of a pancreatic head tumor: GIST with pancreatic divisum. P0219. 19th United European Gastroenterology Week, Stockholm, Monday, October 24, 2011.
- Kim HH, Koh YS, Park EK, Seoung JS, Hur YH, Kim JC, Cho CK. Primary Extragastrointestinal stromal tumor arising in the pancreas: report of a case. Surgery Today 2012; 42:386-90. [PMID: 22258729]
- Babu SR, Kumari S, Zhang Y, Su A, Wang W, Tian B. Extra gastrointestinal stromal tumor arising in the pancreas: a case report and literature review. J Gastroenterol Hepatol Res 2012; 1:80-83. [doi:10.6051/j.issn.2224-3992.2012.01.059]
- Kucukardali Y, Oncul O, Cavuslu S, Danaci M, Calangu S, Erdem H, Topcu AW. The spectrum of diseases causing fever of unknown origin in Turkey: a multicenter study. Int J Infect Dis 2008; 12:71-79. [PMID: 17629532 ]
- Arnogiannaki N, Martzoukou I, Kountourakis P, Dimitriadis E, Papathanasaki A, Nastoulis E, Gazalidou M. Synchronous presentation of gastrointestinal stromal tumors and other primary neoplasms: A single center experience. In Vivo; 2010; 24 (1):109-15. [PMID: 20133985 ]
- Resorlu B, Baltaci S, Resorlu M, Kankaya D, Savas B. Coexistence of papillary renal cell carcinoma and gastrointestinal stromal tumor in a case. Turk J Gastroenterol 2007; 18(1):47-49. [PMID: 17450496]
- Au WY, Ho KM, Shek TW. Papillary renal cell carcinoma and gastrointestinal stromal tumor: a unique association. Ann Oncol 2004; 15 (5):843-44. [PMID: 15111359]
- Betigeri AM, Pasupathi P, Bakthavathsalam G, Pugazhenthi B. Co-existence of conventional renal cell carcinoma with gastrointestinal stromal tumor. Int J Biolog Med Res 2010; 1 (3): 88- 89.
- Burgees P, O’Shea M, Gaskin D, Jonnalagadda R. Co-existence of colonic carcinoma, renal cell carcinoma, and gastrointestinal stromal tumor- a case report. Int J Surg Case Report 2010; 1(2):6-8. doi: 10.1016/j.ijcr.2010.06.002.
- Visser BC, Yeh BM, Qayyum A, Way LW, McCulloch CE, Coakley FV. Characterization of cystic pancreatic masses: relative accuracy of CT and MRI. AJR Am J Roentgenol 2007; 189:648-56. [PMID 17715113]
- Anand MKN, Boylan C, Gupta N, Amin Z, Coombs BD, Schmiedl UP, Krasney RM, Karani J. Pancreatic adenocarcinoma imaging. Medscape 2011 (article ID 370909).
- Fletcher CD, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ, Miettinen M. Diagnosis of gastrointestinal stromal tumors: a concensus approach. Human Pathol 2002; 33: 459-65. [PMID: 12094370]
- Kindblom LG, Remotti HE, Aldenborg F, Meis-Kindblom JM. Gastrointestinal pacemaker cell tumor (GIPACT): gastrointestinal stromal tumors show phenotypic characteristics of the interstitial cells of Cajal. Am J Pathol 1998; 152:12459-69. [PMID: 9588894]
- Erlandson RA, Klimstra DS, Woodruff JM. Subclassification of gastrointestinal stromal tumors based on evaluation by electron microscopy and immunohistochemistry. Ultrastruct Pathol 1996; 20:373-93. [PMID: 8837346]
- Ghaffer MA. Large gastrointestinal stromal tumor size does not imply early recurrence. Int Med Case Reports J 2010; 3:13-17.
- Demetri GD, vonMehren M, Antonescu CR, et al.,“NCCN task force report: Update on the management of patients with gastrointestinal stromal tumors,”JNCCN Journal of the National Comprehensive Cancer Network, vol. 8, supplement 2, S1-S44, 2010.
- Huizinga JD, Thuneberg L, Vanderwinden JM, Rumessen JJ. Interstitial cells of Cajal as targets for pharmacological intervention in gastrointestinal motor disorders. Trends Pharmacol Sci 1997; 18:393-403. [PMID: 9357324]
- Ardeleanu C and Bussolati G. Telocytesare the common cell of origin of both PEComas and GISTs: an evidence-supported hypothesis. J Cell Mol Med 2011; 15 (12): 2569-74. [PMID: 21977985]
- Tirgoviste CI. Pancreatic beta cell clock and telocytes (Editorial). Romanian J Diabetes Nutrn Metabol Dis 2011; 18 (1):
- Ardeleanu C, Arsene D, Hinescu M, Andrei F, Gutu D, Luca L, and Popescu LM. Pancreatic expression of DOG1: a novel Gastrointestinal Stromal Tumor (GIST) biomarker. Appl Immunohistochem Mol Morphol 2009; 17(5): 413-18. [PMID: 19417627]
- Bergmann F, Andrulis M, Hartaig W, Penzel R, Gaida MM, Herpel E, Schiracher P, et al. Discovery on gastrointestinal stromal tumor 1 (DOG1) is expressed in pancreatic centroacinar cells and in solid-pseudopapillary neoplasms-novel evidence for a histogenetic relationship. Human Human Pathol 2011; 42 (6):817-823. [PMID:21295818]

