Keywords
Antioxidants; Caerulein; Cyclosporine; Fibrosis; Oxidative Stress; Pancreas, Pancreatitis; Therapeutics
Abbreviations
CyA: cyclosporin A; GPx: glutathione peroxidase; TAS: total antioxidant status
INTRODUCTION
Chronic pancreatitis is characterized by the irreversible destruction of the pancreatic structure with progressive loss of both exocrine and endocrine functions. Pancreatic fibrosis is a characteristic histopathological feature of chronic alcoholic pancreatitis, the most frequent etiology of this disease and is responsible for pancreatic gland destruction. Over the past few years, the pathogenesis of pancreatic fibrosis has received increased attention, largely due to the identification and characterization of stellate cells, the principal effectors of pancreatic fibrosis [1, 2].
The pancreatic stellate cells are activated when they are exposed to ethanol, to its metabolite acetaldehyde or to oxidant stress. Intracellular oxidative stress is an early phenomenon in cells exposed to the above compounds. Not only the alcohol transformation to acetaldehyde but also the generation of oxidant stress within the cells can activate the stellate cells [3]. The antioxidant deficiency may play a role in the pathogenesis of chronic pancreatitis. Rose et al. observed deficiencies in the intake of selenium, vitamins A, C, E and riboflavin in dietary patients with chronic pancreatitis as compared to a healthy control group [4]. Braganza et al. subsequently demonstrated that antioxidant levels were depleted in patients with this disease, being lowest during painful exacerbations of the process [5]. These antioxidant deficiencies were also observed in patients with both temperate and tropical pancreatitis [5, 6] and led to the hypothesis that chronic pancreatitis was related to oxidative stress, defined as a state of potential injury due to any imbalance between injurious free radicals and protective antioxidants [7]. Morris-Stiff et al. found that chronic pancreatitis is related to antioxidant deficiency [8] and there is evidence that antioxidant supplementation in such cases reduces the demand for analgesics and the frequency of hospital admission due to painful exacerbations [9, 10].
The well-known interdependence of antioxidants, which plays an important role in the organism, encouraged us to use a combination of antioxidants instead of only one, as the low concentration availability of one would interfere with the action or the effect of the others. Interactions of the micronutrients highly support the close interdependence of all antioxidants due to the fact that the low deficiency in one may cause a decrease in the bioactivity of the others, even at recommended doses [11, 12].
In the present study, therefore, we hypothesized that the administration of an antioxidant complex could ameliorate cerulein and cyclosporin A (CyA) pancreatic fibrosis, assessed by changes in oxidative stress and a histopathological study in an experimental rat model.
METHODS
Animals
Forty male Wistar rats weighing 250-300 g were purchased from Harlam Iberica (Barcelona, Spain). They were housed in boxes under conditions of constant temperature and a normal daylight cycle.
Materials
Cerulein was purchased from Pharmacia and Upjohn Laboratories (Nerviano, Milano, Italy). Cyclosporin A was purchased from Novartis Laboratories (Basel, Switzerland). The antioxidant complex was produced by the Unit for Master Formulae, in the Pharmacy Department of our hospital. It was composed of L-methionine, beta-carotene, ascorbic acid (vitamin C), alfa-tocopherol succinate (vitamin E), organic selenium and a sufficient quantity of universal excipient.
Experimental Procedures
Forty rats were divided into four groups of ten.
Group A (Saline). A saline solution was given intraperitoneally to the rats and they were used as a control group.
Group B (Cerulein). At weekly intervals, six episodes of acute pancreatitis were induced in the rats by intraperitoneal administration of two doses of cerulein (10 μg/kg) one hour apart.
Group C (Cerulein+cyclosporin A). Cyclosporin A (20 mg/kg) was given intraperitoneally the day before and the day on which the pancreatitis was induced, and cerulein was given as in Group B.
Group D (Cerulein+cyclosporin A+antioxidants). The animals were treated like the ones in Group C but also received Lmethionine (34 mg/kg), beta-carotene (0.26 mg/kg), ascorbic acid (vitamin C) (13 mg/kg), succinate of alfa-tocopherol (vitamin E) (4 μg/kg), organic selenium (6 μg/kg) orally.
All the rats were sacrificed at the 7th week. To carry out biochemical determinations and histologic study, after excision, total pancreases were excised, trimmed of fat and lymph nodes. Some small pancreatic samples from each rat were immediately embedded in 10% formalin, paraffin-embedded, and stained with hematoxylin-eosin and Masson’s trichrome. The remainder of the pancreas was weighed and pancreatic homogenates were prepared with an homogenizing buffer and by serial use of a Polytron (Kinematica, Luzern, Switzerland). The samples were frozen at - 80ºC until specific determination.
Glutathione Peroxidase (GPx)
We measured the indirect colorimetric activity of cellular glutathione peroxidase in pancreatic extract (Bioxytech GPx-340, OxisResearch, Portland, OR, USA). The values were expressed as mU/g protein.
Total Antioxidant Status (TAS)
The total antioxidant status was analyzed by espectrofotometry (Hitachi 704, Hitachi, Tokyo, Japan) using a commercial kit (Randox Laboratories, Antrim, UK). Results were expressed as mmol/g protein.
Histologic Study
After excision, some small pancreatic samples from each rat were immediately embedded in formalin, paraffin-embedded, and stained with hematoxylin-eosin and Masson’s trichrome. Microscopic findings were scored by pathologists who were experts in pancreatic pathology and who were blinded to the experimental group. The presence of fibrosis (intralobular or interlobular) was evaluated according to the following scoring system: 0, absent; 1, light fibrosis (less than one half lobule or intralobular region lesions); 2, moderate fibrosis (a lesion widely shown in the lobule or intralobular region (one half or more)); 3, intense fibrosis (a lesion shown across lobules and intralobular regions or with destruction of lobular architecture) [13]. The histologic results are expressed according to the score obtained from the rats of each group.
ETHICS
All animals received humane care according to the criteria outlined in the 'Guide for the Care and Use of Laboratory Animals prepared by the National Academy of Sciences [https://www.nap.edu/books/0309053773/html /index.html].
STATISTICS
All data were expressed as mean±standard deviation (SD). The results were analyzed with the computer SPSS package (Statistical Package for Social Sciences, Chicago, IL, USA). Non-parametric test were used. The
Kruskal-Wallis test was applied to evaluate differences among all groups while differences between pairs of groups were evaluated by means of the Mann-Whitney test. Comparisons between frequencies were done by means of the chi-squared test. Twotailed P values less than 0.05 were considered statistically significant.
RESULTS
Fibrosis
The distribution of the score of fibrosis was significantly different among the 4 groups (P=0.001; Table 1).
Group A (Saline). Fibrosis was absent in all rats. Figure 1 shows a normal pancreas without fibrosis (scoring system equal to 0).
Figure 1. Normal pancreatic tissue (Group A, saline).
Group B (Cerulein). Repeated administration of cerulein caused minimal fibrosis (stage 1) or moderate fibrosis (stage 2) in 90% of the rats; however, one rat (10%) in this group did not develop fibrosis. The fibrosis score for this group was 1.1±0.3 (Figure 2).
Figure 2. Minimal fibrosis in pancreatic tissue (Group B, cerulein).
Group C (Cerulein+cyclosporin A). Three rats in this group (30%) did not develop fibrosis (grade 0), but the other 7 (70%) developed different grades (3 light fibrosis, grade 1; 3 moderate fibrosis, grade 2; 1 intense fibrosis, grade 3). In 4 cases (40%), the fibrosis distribution was multifocal and, in 3 cases (30%), the distribution was diffuse. The fibrosis score for this group was 1.2±0.3 (Figure 3).
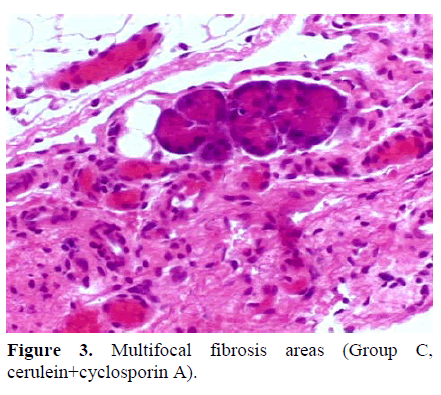
Figure 3. Multifocal fibrosis areas (Group C, cerulein+cyclosporin A).
Group D (Cerulein+cyclosporin A+antioxidants). In this group, only two of the 10 rats (20%) showed light fibrosis (grade 1) and both of them had a focal distribution. The fibrosis score for this group was 0.2±0.4 (Figure 4).
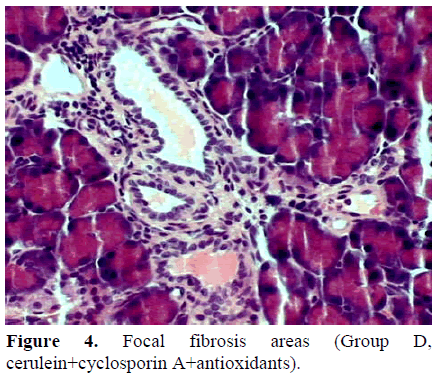
Figure 4. Focal fibrosis areas (Group D, cerulein+cyclosporin A+antioxidants).
Figure 5 shows the mean±SD of the score of fibrosis in the four groups. We did not find significant differences between Groups B and C (1.1±0.3 and 1.2±0.3, respectively; P=0.200) or between Groups A and D (0 and 0.2±0.4 respectively; P=0.200) but, when we compared the control Group A and Group D with Groups B and C, the fibrosis was more severe in Groups B and C, (A vs. B: P<0.001; A vs. C: P=0.003; B vs. D: P=0.003; C vs. D: P=0.030).
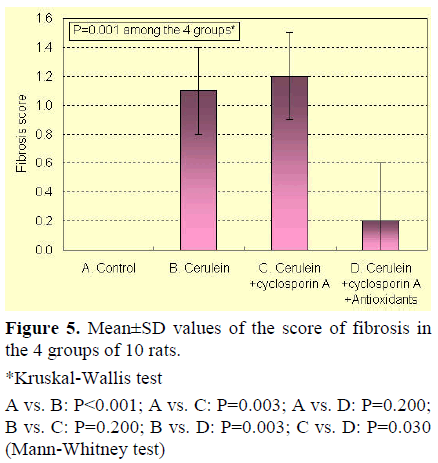
Figure 5. Mean±SD values of the score of fibrosis in the 4 groups of 10 rats.
*Kruskal-Wallis test
A vs. B: P<0.001; A vs. C: P=0.003; A vs. D: P=0.200; B vs. C: P=0.200; B vs. D: P=0.003; C vs. D: P=0.030 (Mann-Whitney test)
Glutathione Peroxidase (GPx)
To evaluate the intensity of oxidative stress, we determined GPx in pancreatic tissue. The results are shown in Figure 6. There were no significant differences in GPx activity between Groups A and D (P=0.739), but the comparison between Group B and the rest of the other Groups (A, C, and D) was significant (P=0.009, P=0.001, and P=0.019, respectively).
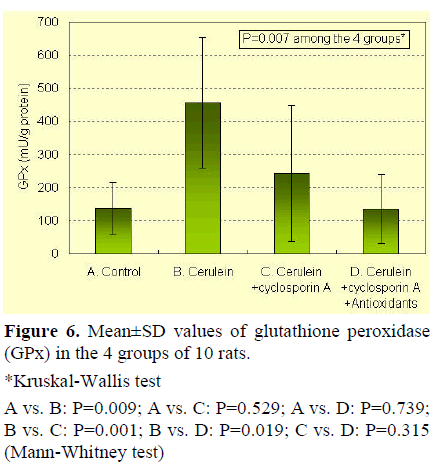
Figure 6. Mean±SD values of glutathione peroxidase (GPx) in the 4 groups of 10 rats.
*Kruskal-Wallis test
A vs. B: P=0.009; A vs. C: P=0.529; A vs. D: P=0.739; B vs. C: P=0.001; B vs. D: P=0.019; C vs. D: P=0.315 (Mann-Whitney test)
Total Antioxidant Status (TAS)
The results for all groups are shown in Figure 7. The cerulein group (B) shows significant differences as compared to the other groups (B vs. A: P<0.001; B vs. C: P<0.001; B vs. D: P=0.002). Moreover, the group with antioxidants (D) shows significant differences with Groups A and C (P<0.001 and P=0.007, respectively).
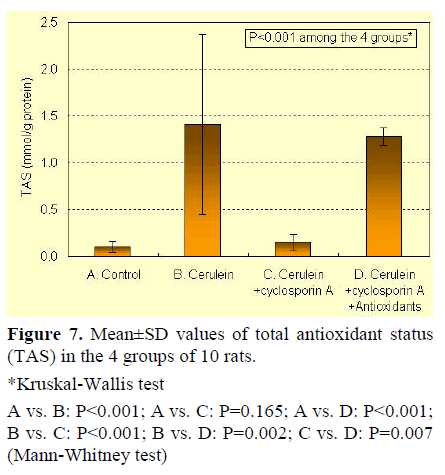
Figure 7. Mean±SD values of total antioxidant status (TAS) in the 4 groups of 10 rats.
*Kruskal-Wallis test
A vs. B: P<0.001; A vs. C: P=0.165; A vs. D: P<0.001; B vs. C: P<0.001; B vs. D: P=0.002; C vs. D: P=0.007 (Mann-Whitney test)
DISCUSSION
Hyperstimulation of the pancreas with supraphysiologic doses of cerulein causes acute pancreatitis with histological and biochemical changes in the rats which duplicate the morphological and biochemical manifestations of human acute pancreatitis [14, 15].
After a single episode of cerulein-induced acute pancreatitis, full recovery of the normal pancreatic architecture occurs. It is now accepted that, during the resolution period, there is an increase in the production of profibrogenic cytokines and matrix components as well as of matrix metalloproteinases [16, 17, 18]. Net accumulation of matrix and tissue fibrosis depends on an imbalance between synthesis and degradation. The maintenance of the injury leads to an excess of matrix production resulting in a progressive accumulation of extracellular matrix components [19].
Oxidative stress plays a role in the early pathogenesis of cerulein-induced acute pancreatitis, as proved by Wisner et al. who injected intravenous polyethylene glycollinked oxygen free radical scavanger enzyme, superoxide dismutase [20]. Schoenberg et al. showed that, after 30 minutes of cerulein infusion, conjugated dienes and malondialdehyde increased, reaching their peak after 3.5 hours and then decreasing to normal values after 12 hours whereas treatment with superoxide dismutase and catalase, either before or after the start of the cerulein infusion, prevented lipid peroxidation [21].
The production of oxygen free radicals occurs early in acute pancreatitis, overwhelming the antioxidant defence system. The acinar cells significantly contribute to the generation of large amounts of oxygen free radicals at the early stages of acute pancreatitis [22]. To clarify the relationship between pancreatic fibrosis and free radicals, Matsumura et al. showed that diethyl dithiocarbamate, an inhibitor of the Cu/Zn-superoxide-dismutase, caused pancreatic fibrosis by oxidative stress without ductal changes [13]. The repetitive induction of pancreatitis by supramaximal doses of cerulein provokes pancreatic weight loss, increase of protein-bound hydroxyproline content, acinar-cell destruction, cellular infiltration, and deposition of collagen fibres. However, 6 weeks after the last administration of cerulein, no differences in the parameters mentioned above could be observed between the controls and the cerulein-treated animals. Thus, repetitive induction of pancreatitis in rats does not result in permanent pancreatic fibrosis [23].
We found that GPx increased in the rats treated with cerulein. The increase in GPx may indicate an adaptative response of acinar cells to oxygen radical generation defending acinar cells against oxidative stress. The generation of intracellular radicals led to an increased concentration of reduced glutathione and enzymatic activities of glutathione related enzymes.
Similar results were observed in another paper in which hepatocarcinoma cells overexpressed CYP2E1 in an ethanoldependent model. When these cells were challenged with ethanol, the glutathione level increased as the enzymes related with enzymatic activities of glutathione increased [24, 25]. Ethanol and pancreas stimulation, or short-term pancreatic obstruction, applied alone led to an increase in pancreatic oxygen free radicals. The induction of ethanol pancreatitis did not lead to the same increase in membrane peroxidation, even though Wittel et al. found an increase in the concentration of cell protective reduced glutathione [26]. We observed an increase of TAS in rats treated with cerulein probably due to a response to the increase of GPx. However, rats treated with cerulein developed fibrosis indicating that the physiological antioxidant reserve may not be enough to prevent the induction of transient fibrosis.
Previous studies have shown that the pancreatic response to cerulein is characterised by inflammatory infiltrates, transient increase of TGF; beta expression, gland atrophy, collagen formation, fibroblast proliferation and acinar necrosis. Despite this, the pancreas completely regenerates with no signs of previous injury [16, 23, 27]. CyA interferes with the normal pancreatic repairing mechanisms so that the pancreatic morphology cannot be completely restored. This process seems to be associated with steadily increased plasma levels of TGF-beta, myofibroblast proliferation and a defective collagenase response to increased collagen formation. CyA greatly distorts pancreatic repair, transforming cerulein-induced pancreatitis into a fibrotic chronic-like disease [28].
Our results demonstrate that the addition of CyA to cerulein induced pancreatic fibrosis as happened when the cerulein was administered alone, but it did not increase the GPx and the TAS which indicates that CyA distorts the physiologic mechanism which increases glutathione related enzymes, thus decreasing the cellular antioxidant capacity. This may be responsible for the transformation of a selflimited process into a chronic-like disease.
The suggestion that antioxidant deficiency could play a role in the pathogenesis of chronic pancreatitis was first published by Rose et al. [4]. Braganza et al. subsequently demonstrated that antioxidant levels were depleted in patients with chronic pancreatitis, a disease characterized by excessive collagenous tissue accumulation in the pancreas, being lowest during painful exacerbations of the process [5]. Van Gossum et al. also observed that patients with alcoholrelated chronic pancreatitis have low blood levels of some antioxidant factors [29]. Other studies have suggested that antioxidant treatment may reduce the need for analgesics, the frequency of hospital admission for painful exacerbations [10], and the indication for pancreatic surgery [9].
In the present study, we observed that the administration of an oral antioxidant complex avoided the development of pancreatic fibrosis. The effector cells of pancreatic fibrosis are probably the pancreatic stellate cells, similar to hepatic stellate cells, the main effector cells in liver fibrosis [1, 2]. These cells are activated by oxidative stress, losing their vitamin A which contains lipid droplets, and transforming them into myofibroblastlike cells which stain for alpha-smooth muscle actine (alpha-SMA). They also become responsive to proliferative and profibrogenic growth factors such as plateletderived growth factor (PDGF), TGF-beta and proinflammatory cytokines, synthesizing and secreting extracellular matrix proteins which induce fibrosis. The oxidative stress generated by cerulein injury, similar to alcoholic pancreatitis, can activate pancreatic stellate cells.
Casini et al. [30] and Apte and Wilson [31] demonstrated the increased expression of the lipid peroxidation product 4-hydroxynonenal in acinar cells adjacent to the areas of fibrosis in patients with chronic alcoholic pancreatitis, indicating the generation of antioxidant stress within the pancreas. This observation supports the hypothesis that oxidative stress is an important activating factor for pancreatic stellate cells [3]. The rats treated with cerulein and cyclosporine A, which received an antioxidant orally, showed higher levels of TAS without an increase in GPx, suggesting that the antioxidative reserve was sufficient to prevent the development of the histologic lesions of fibrosis. These observations agree with the study of Gómez et al. who observed that vitamin E reduces oxidative stress and collagen deposition during experimental chronic pancreatitis [32].
Other reports have demonstrated that cyclosporin A produces fibrosis, being in part responsible for the early failure of some transplanted grafts [33]. We have not analyzed rats treated only with cyclosporine A or cyclosporine A+antioxidant drugs because cyclosporin A alone does not produce significant alterations of the pancreatic architecture [28]. Our objective was to evaluate whether antioxidants administration could ameliorate fibrosis in an experimental model of chronic pancreatitis. Moreover, the analysis of these two groups of rats would increase the complexity of both the results and the conclusions.
In conclusion, we suggest that the administration of an antioxidative complex taken orally could be useful in preventing collagen deposition in chronic pancreatitis.
References
- Apte MV, Haber PS, Applegate TL, Norton ID, McCaughan GW, et al. Periacinar stellate-shaped cells in rat pancreas: Identification, isolation and culture. Gut 1998; 43:128-33. [PMID 9771417]
- Bachem MG, Schneider E, Gross H, Weidenbach H, Schmid RM, Menke A, et al. Identification, culture, and characterization of pancreatic stellate cells in rats and humans. Gastroenterology 1998; 115:421-32. [PMID 9679048]
- Apte MV, Phillips PA, Fahmy RG, Darby SJ, Rodgers SC, McCaughan GW, et al. Does alcohol directly stimulate pancreatic fibrogenesis? Studies with rat pancreatic stellate cells. Gastroenterology 2000; 118:780-94. [PMID 10734030]
- Rose P, Fraine E, Hunt LP, Acheson DW, Braganza JM. Dietary antioxidants and chronic pancreatitis. Hum NutrClinNutr 1986; 40:151-64. [PMID 3957720]
- Braganza JM, Schofield D, Snehalatha C, Mohan V. Micronutrient antioxidant status in tropical compared with temperate-zone chronic pancreatitis. Scand J Gastroenterol 1993;28:1098-104. [PMID 8303214]
- Yadav S, Day JP, Mohan V, Snehalatha C, Braganza JM. Selenium and diabetes in the tropics. Pancreas 1991; 6:528-33. [PMID 1946309]
- Braganza JM. The pathogenesis of chronic pancreatitis. QJM 1996; 89:243-50. [PMID 8733510]
- Morris-Stiff GJ, Bowrey DJ, Oleesky D, Davies M, Clark GW, Puntis MC. The antioxidant profiles of patients with recurrent acute and chronic pancreatitis. Am J Gastroenterol 1999; 94:2135-40. [PMID 10445540]
- Uden S, Schofield D, Miller PF, Day JP, Bottiglier T, Braganza JM. Antioxidant therapy for recurrent pancreatitis: Biochemical profiles in a placebocontrolled trial. Aliment PharmacolTher 1992; 6:229- 40. [PMID 1600043]
- De lasHerasCastaño G, Garcia de la Paz A, Fernandez MD, Fernandez Forcelledo JL. Use of antioxidants in the treatment of the pain in chronic pancreatitis. Rev EspEnferm Dig 2000; 92:375-80. [PMID 10985097]
- Mathew P, Wyllie R, Van Lente F, Steffen RM, Kay MH. Antioxidants in hereditary pancreatitis. Am J Gastroenterol 1996; 91:1558-62. [PMID 8759661]
- Braganza JM, Thomas A , Robinson A. Antioxidants to treat chronic pancreatitis in childhood. Case report and possible implications for pathogenesis. Int J Pancreatol 1988; 3:209-16. [PMID 3361161]
- Matsumura N, Ochi K, Ichimura M, Mizushima T, Harada H , Harada M. Study on free radicals and pancreatic fibrosis. Pancreatic fibrosis induced by repeated injections of superoxide dismutase inhibitor. Pancreas 2001; 22:53-7. [PMID 11138971]
- Niederau C, Ferrell LD, Grendell JH. Caeruleininduced acute necrotizing pancreatitis in mice: protective effects of proglumide, benzotript, and secretin. Gastroenterology 1985; 88:1192-204. [PMID 2984080]
- Goerelick FS, Adler G ,Kem HF. Cerulein induced pancreatitis. In: Go VLW, DiMagno EP, Gardner JP, Lebenthal E, Reber HA, Scheele GA(eds). The Pancreas: Biology, Pathobiology, and Disease. 2nd ed. New York, NY, USA: Raven Press, 1993:501-26.
- Elsasser HP, Adler G, Kern HF. Fibroblast structure and function during regeneration from hormone-induced acute pancreatitis in the rat. Pancreas 1989; 4:169-78. [PMID 2755941]
- Gress TM, Müller-Pillasch F, Yamaguchi H, Adler G, Menke A. Expression and activation of extracellular-matrix degrading proteases and tissueinhibitors of metalloproteinases during regeneration from acute cerulein-induced pancreatitis (Abstract). Pancreas 1996; 13:438.
- Muller-Pillasch F, Gress TM, Yamaguchi H, Geng M, Adler G, Menke A. The influence of Transforming Growth Factor ß1 on the expression of genes coding for matrix metalloproteinases and tissue inhibitors of metalloproteinases during regeneration from cerulean induced pancreatitis. Pancreas 1997; 15:168-75. [PMID9260202]
- Neuschwander-Tetri BA, Burton FR, Presti ME, Britton RS, Janney CG, Garvin PR, et al. Repetitive self-limited acute pancreatitis induces pancreatic fibrogesis in the mouse. Dig Dis Sci 2000; 45:665-74. [PMID 10759232]
- Wisner J, Green D, Ferrell L, Renner I. Evidence for a role of oxygen derived free radicals in the pathogenesis of cerulein induced acute pancreatitis in rats. Gut 1988; 29:1516-23. [PMID 3209108]
- Schoenberg MH, Buchler M, Gaspar M, Stinner A, Younes M, Melzner I, et al. Oxygen free radicals in acute pancreatitis of the rat. Gut 1990; 31:1138-43. [PMID 1707389]
- Urunuela A, Sevillano S, de la Mano AM, Manso MA, Orfao A , De Dios I. Time-course of oxygen free radical production in acinar cells during acute pancreatitis induced by pancreatic duct obstruction. BiochimBiophysActa 2002; 1588:159. [PMID 12385780]
- Elsasser HP, Haake T, Grimmig M, Adler G, Kern HF. Repetitive cerulein-induced pancreatitis and pancreatic fibrosis in the rat. Pancreas 1992; 7:385-90. [PMID 1594561]
- Woods JS, Kavanagh TJ, Corral J, Reese AW, Diaz D, Ellis ME. The role of glutathione in chronic adaptation to oxidative stress studies in a normal rat kidney epithelial (NRK52E) cell model of sustained up regulation of glutathione biosynthesis. ToxicolApplPharmacol 1999; 160:207-16. [PMID 10544055]
- Mari M, Wu D, Nieto N, Cederbaum AI. CYP2E1- dependent toxicity and upregulation of antioxidant genes. J Biomed Sci 2001; 8:52-8. [PMID 11173976]
- Wittel UA, Bachem M, Siech M. Oxygen radical production precedes alcohol-induced acute pancreatitis in rats. Pancreas 2003; 26:e74-80. [PMID 12717277]
- Adler G, HuppT , Kern HF. Course and spontaneous regression of acute pancreatitis in the rat. Virchows Arch A PatholAnatHistol 1979; 382:31-47. [PMID 157597]
- Vaquero E, Molero X, Salas A , Malagelada JR. Myofibroblast proliferation, fibrosis, and defective pancreatic repair by cyclosporin in rats. Gut 1999; 45:269-77. [PMID 10403741]
- Van Gossum A, Closset P, Noel E, Cremer M ,Neve J. Deficiency in antioxidant factors in patients with alcohol-related chronic pancreatitis. Dig Dis Sci 1996; 41:1225-331. [PMID 8654156]
- Casini A, Galli A, Pignalosa P, Frulloni L, Grappone C, Milani S, et al. Collagen type I synthesized by pancreatic periacinar stellate cells (PSC) co-localizes with lipid peroxidation-derived aldehydes in chronic alcoholic pancreatitis. J Pathol 2000; 192:81-9. [PMID 10951404]
- Apte MV, Wilson JS. Stellate cell activation in alcoholic pancreatitis. Pancreas 2003; 27:316-20. [PMID 14576494]
- Gomez JA, Molero X, Vaquero E, Alonso A, Salas A, Malagelada JR. Vitamin E attenuates biochemical and morphological features associated with the development of chronic pancreatitis. Am J PhysiolGastrointest Liver Physiol 2004; 287:G162-9. [PMID 15001429]
- Johnson DW, Saunders HJ, Johnson FJ, Huq SO, Field MJ, Pollock CA. Fibrogenic effects of cyclosporin A on the tubulointerstitium: role of cytokines and growth factors. ExpNephrol 1999; 7:470-8. [PMID 10559645]

