Keywords
Antimetabolites, Antineoplastic; Drug Therapy; Follow-Up Studies; Neoplasm Staging; Palliative Care; Pancreas Neoplasms
Abbreviations
CBR: cinical benefit response; CDDP: cisplatin; dCPT: deoxycitidinetriphosphate; FA: folinic acid; GEM: gemcitabine; KPS: Karnofski performance status; ORR: overall response rate; OS: overall survival; PC: pancreatic cancer; TTP: time to progression; VEGF: vascular endothelial growth factor; 5-FU: 5- fluorouracil
INTRODUCTION
A few years ago the current opinion on pancreatic cancer (PC) was that the only curative option was surgical resection, since this neoplasm is chemo- and radio-resistant. Only about 20% of diagnosed tumors were resectable with 10% confined to the pancreas. Forty percent were locally advanced (T3 N0 M0, T1-3 N1 M0; stage III-UICC) and 50% were metastatic (any T-N, M1; stage IVUICC) [1-6] and the majority was unresponsive to chemo- and/or radio-therapy with many toxic side effects. Nowadays the 5-year survival is still poor, but a multimodal therapeutic approach extends the life span and improves thequality of life. A multimodal therapy includes two or more of following therapeutic approaches: chemoor chemoradio-therapy, adjuvant therapy, neoadjuvant therapy, endoscopic therapy and the newer therapeutic frontiers of immunotherapy, angiogenesis-inhibitors and gene-therapy.
Chemotherapy
Until now, the results of citotoxic chemotherapy have been very disappointing and, as a consequence, it is generally accepted that PC is a chemoresistant neoplasm and there is no significant advantage in employing chemotherapy either as a single agent or in combination treatments for patients outside of clinical trials [7-10]. In the last two decades, only mitomycin C and 5- fluorouracil (5-FU) have been consistently reported to induce a 15-29% overall response rate, so that no standard chemoterapy treatment for advanced PC has been established so far [11, 12]. Combination regimes, such as the FAM (5- FU, adriamycin, and mitomycin C) or the SMF (streptozotocin, mitomycin C, and 5- FU) combinations were shown to induce a nearly 30% overall response rate with an unsatisfactory median survival of less than 6 months and poor control of symptoms [13]. Unfortunately, subsequent trials failed to confirm this response rate on survival, thus showing that combined chemotherapy was not superior to monochemotherapy with 5-FU [2, 4].
Recently it has been pointed out that the evaluation of chemotherapy in advanced PC should be realistically based on palliative endpoints, such as symptom relief and performance status, more than on classical efficacy measures such as time response and survival [14].
Gemcitabine Mechanisms
Gemcitabine (2’,2’-difluorodeoxycytidine), a nucleoside analogue with demonstrated activity in non-small cell lung tumor, breast, bladder and ovarian cancers, has recently been proved to be able to induce durable symptomatic improvement with favourable toxicity profile in patients with PC [15-20]. Gemcitabine is a pro-drug which is converted in vivo into two potent cytotoxic phosphorylate metabolites: gemcitabine diphosphate and gemcitabine triphosphate. The first one blocks deoxycitidinetriphosphate (dCPT) synthesis inhibiting the enzyme ribonucleotide reductase, which controls the normal synthesis of triphosphate deoxynucleotides [21]. Gemcitabine triphosphate is able to inhibit DNA synthesis by direct competition with dCPT for incorporation into the DNA strand [22].
The inclusion of gemcitabine into the DNA causes the so-called masked chain termination, i.e. hiding gemcitabine triphospate from removal by repair enzymes thus slowing the repair process [22]. Moreover, gemcitabine is able to self potentiate its activity since gemcitabine diphosphate inhibits the enzyme deoxycytidine kinase, which convertes gemcitabine into its active metabolites [21]. Both diphosphate and triphosphate metabolites inhibit directly and indirectly the enzymes of deamination which are involved in gemcitabine cellular clearance [22].
These mechanisms may explain why gemcitabine is seen within tumour cells at higher levels, for long periods, and has greater activity in human solid tumors compared with cytosine, arabinoside, which is similar in structure. In addition, pre-clinical in vitro studies have confirmed that gemcitabine behaves as a potent radiosensitizer in pancreatic and other cell lines.
The mechanism of radiosensitization probably involves the depletion of cellular nucleotides that can be achieved with very low tissue concentrations of gemcitabine [13].
Experience with Gemcitabine in Pancreatic Cancer
Phase II studies with weekly gemcitabine in patients with PC were initially carried out in the United States [15] and in Europe [16]. In both studies, the primary objective was to measure the response rate to gemcitabine in patients with measurable disease. In the American Study the treatment plan was for a dosage of 800 mg/m2 to be given weekly for 3 or 4 weeks (one treatment cycle). Increasing the dosage by 25% in subsequent cycles was prescribed in the absence of dose-limiting toxicity, to a maximum dosage of 1500 mg/m2. Forty-four patients entered this study; partial responses were observed in 5 of the 44 patients (11%). In addition, 14 patients (32%) had stable disease for more than 4 months. The Authors concluded that, while there was marginal activity as expressed by a partial response rate, further studies of this drug in patients with PC were definitely warranted. This conclusion was based on observations on the degree and frequency of symptomatic improvement, the durability of some of the remissions and the favourable toxicity profile. In the European study [16], the initial plan was for a dosage of 800 mg/m2 to be given once weekly for 3 or 4 weeks. There was minimal toxicity with this schedule and, after 6 patients, the starting dose was increased to 1000 mg/ m2. As well as assessing the effects of gemcitabine on tumour size, some preliminary information was collected on performance status, analgesic consumption, and pain intensity. Thirty-four patients entered the study, the majority (61%) having metastatic disease, primarily in the liver. A partial response was observed in 6.5% and stable disease in 18.8% of the patients; an improvement in performance status for more than 4 weeks was observed in 17.2 % of the patients; 7.4% had improvement in analgesic consumption, 28% in pain intensity and 27% in nausea; symptomatic improvements lasted for approximately 8 to 12 weeks. The drug was well tolerated. Results of both trials [14, 15] showed that a proportion of patients fel somewhat better on treatment, despite not satisfying the criteria for a partial response. Therefore, gemcitabine did seem to provide useful palliation for some patients.
Two further studies were planned for locally advanced or metastatic PC to assess the impact of the drug on Cinical Benefit Response (CBR): evaluation derived from the assessment of pain, functional impairment by Karnofski performance status (KPS), and weight change. In the study of Rothenberg and coworkers [17], gemcitabine was given in patients refractory to 5-FU, at a dosage of 1000 mg/m2 weekly for 7 weeks followed by a week of rest and then once weekly for 3 of 4 weeks. Sixty-three patients entered the study: CBR positive was noted in 27% of the patientes, with a mean duration of 14 weeks. The treatment was well tolerated with low incidence of serious toxicity (only one patient experienced WHO grade 4 toxicity). More recently, Burris and coworkers [18] reported the definitive results of a phase III study on 126 patients with advanced PC, randomized to gemcitabine (1000 mg/m2 weekly for up to 7 weeks followed by a week of rest, and then 3 times weekly for 4 weeks thereafter) or to 5- FU (600 mg/m2 once weekly). CBR was the primary endpoint: 23.8% of the gemcitabine patients experienced CBR positive versus only 4.8% of the 5-FU patients (P=0.002); the median survival for gemcitabine patients was 5.65 months and for 5-FU patients 4.41 months (P=0.002). Twenty-four percent of gemcitabine patients and 6% of the 5-FU patients were alive at 12 months.
Personal Experience
We carried out a multicenter phase II trial of weekly gemcitabine on a series of patients suffering from PC. Patients with a pathologic diagnosis of PC which was locally advanced (stage III-UICC) [23] or metastatic (stage IV) and not amenable to operative surgical resection. Patients who had received previous chemotherapy or irradiation and those with brain metastases were not eligible. Additional inclusion criteria were: a) age 18-75 years; b) adequate bone marrow and biochemical parameters: white blood cell count �3,000/mmc; platelets �90,000/mmc; haemoglobin �9 g/ dL, hematocrit �27%; serum creatinine �1.5 mg/ dL, aspartate and alanine transaminases less than 3 times the upper normal limit. Patients were required to have an estimated life expectancy of at least 3 months, a baseline KPS ranging from 50 to 90, and a baseline analgesic comsumption of �10 mg/day of morphine equivalent. Gemcitabine hydrocloride (Gemzar®, Ely Lilly, Sesto Fiorentino, Italy) was administred on an outpatient basis, once a week for 3 weeks, followed by a week rest period; the starting dose was 1000 mg/m2.
The drug was diluted in normal saline and administered intravenously over 30 minutes; 5 mg of tropisetron chloroidrate (Navoban®, Novartis, Origgio-Varese, Italy) preceded the infusion. Dose modification was based on blood cell counts (samples from the day before treatment); dose reduction of 50% was carried out for grade 2 hematological toxicity; one week interruption was performed for grade 3 toxicity or greater. Treatment continued until there was evidence of disease progression or until there was significant clinical deterioration because of tumor-related symptoms.
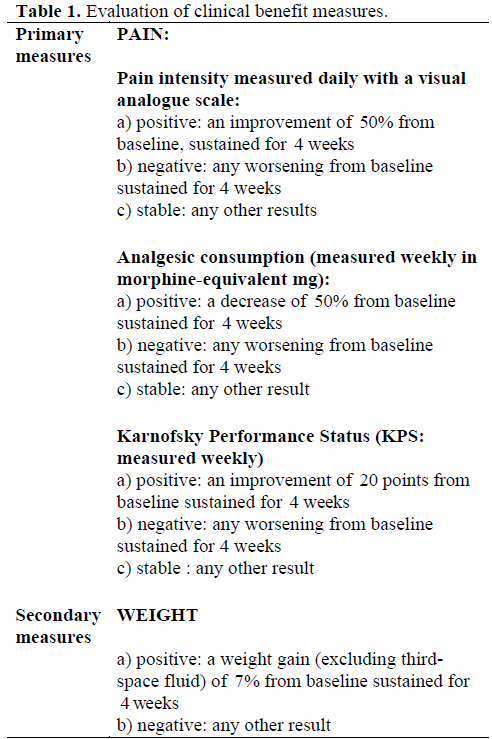
Evaluation of efficacy was based on CBR and objective response. CBR evaluation constituted the primary end point of the study and was evaluated as stated in Table 1. Another measure of efficacy, such as objective tumor response, was also assessed. Complete tumor response, partial response and progressive disease were defined in accordance with standard criteria [15]. Responses were evaluated by two external oncologists who were not directly involved into the study.
Safety was evaluated at baseline and during therapy using WHO criteria [18]. Patients were followed weekly with updating, physical examinations, complete blood counts, blood chemistry profiles, and urinalysis.
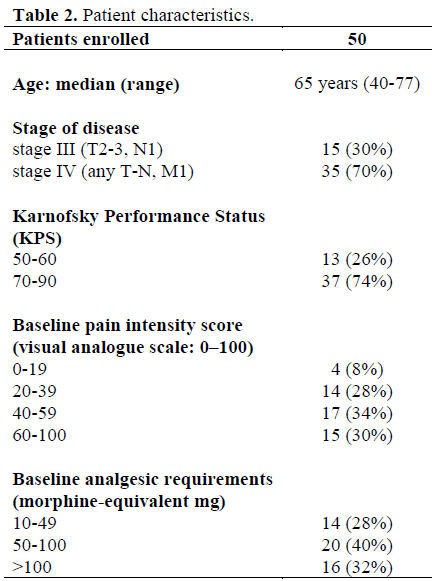
Fifty patients entered the study between July 1996 and April 1997; the main clinical characteristics of these patients are indicated in Table 2. Positive CBR was observed in 16 of the 50 patients (32%; 95% CI: 25-38%); improvement in pain was observed in 16 patients (32%), KPS in 11 patients (22%), and weight in 8 (16%). Median time to achieve improvement was 5 weeks. Objective response rates were: overall response in 8 patients (16%; 95% CI: 5-21%); stable disease in 17 patients (34%; 95% CI: 18- 41%), and progression in 26 patients (52%). Median time progression was 3.2 months.
The drug was generally well-tolerated. The incidence of hematologic toxicity was low: leukopenia/thrombocytopenia (WHO grade 3) was observed in 10 patients (20%), and anemia (WHO grade 3) was found in 5 patients (10%) and two patients required a red blood cell transfusion. The incidence of nausea and vomiting (WHO grade 1-2) was 20% (10 patients), while infective episodes (WHO grade 2) were observed in 5 patients (10%). Other side effects included flu-like symptoms in 6 patients (12%) and mild hair loss in 3 patients (6%).
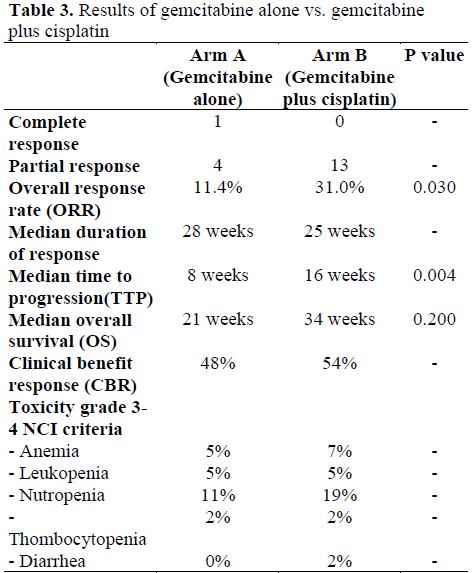
A second randomized phase II study was performed with gemcitabine alone vs. gemcitabine plus cisplatin in a multicenter trial carried out by the southern Italy Oncology Group (GOIM). The treatment schedules were as follows: arm A) gemcitabine at 1000 mg/m2 over 30-minute infusion one day; arm B) gemcitabine at same modality of arm A followed by cisplatin 25 mg/m2. Both treatments were administered weekly for 7 consecutive weeks followed by one week of rest and then for 3 times per week for 4 weeks. In arm B, in the 4th week of the 1st cycle, only gemcitabine was administered. One hundred and seven patients with bidimensionally measurable disease entered the study (arm A: 54 patients; arm B: 53 patients) but only 86 were evaluable for response (A: 44; B: 42). Characteristics of the two groups were (A vs. B): stage III and IV UICC; median age: 63 vs. 60 years; median performance status: 70 vs. 70; sites of disease: primary tumour 40 vs. 35, liver 19 vs. 20, lymph nodes 16 vs. 17, lung 2 vs. 1, multiples sites 27 vs. 29; patients evaluable for clinical benefit were 39 vs. 35. The results of this study are summarized in Table 3 and, as can be seen, the combination gemcitabine and cisplatin is more effective than gemcitabine alone in the treatment of advanced PC in terms of overall response rate (ORR), median time to progression (TTP) and median overall survival (OS). Both regimens showed a low toxicity profile and high response in clinical benefit.
Recently another multicenter phase II study was carried out by the same previous medical group using four drugs: gemcitabine (GEM), cisplatin (CDDP), folinic acid (FA) and 5-FU in locally advanced and/or metastatic pancreatic adenocarcinoma. Twenty patients were enrolled; all had bidimensionally measurable neoplastic disease and their characteristics were: sex: 12 males and 8 females; median age: 66 years (range 42-75); median KPS: 80 (range 50-100). Sites of disease were: primary tumor 19, liver 9, lymphonodes 3, others 5, and 12 patients had multiples disease sites. The treatment schedule was: CDDP 25 mg/m2, GEM 1000 mg/m2, 5-FU 300 mg/m2, FA 100 mg/m2. Drugs were administered weekly for 7 consecutive weeks followed by one week rest, and then for 3 weeks out of every four. In the 4th week of the first cycle only GEM was administered. At present, 15 patients are evaluable for activity; 2 patients were excluded for toxicity and for 3 patients it is too early to evaluate. The following were observed in the evaluable patients: 3 showed partial response, 7 showed stable disease and 5 showed progression (objective response rate: 20%; tumor growth control rate: 75%). In 17 patients evaluable for toxicity, neutropenia in 29%, leukopenia in 29%, anemia in 12%, mucosites in 12%, nausea vomiting in 12%, and diarrhea in 6% were observed as main grade 3-4.
When comparing the last two studies reported, the addition of FA and 5-FU to CDDP plus GEM does not seem to increase the efficacy while an increased toxicity has been observed.
Intra-Arterial Chemoterapy
Attempts at intra-arterial administration of antineoplastic agents were started about 1982 [24]. Recently a new approach (Phase I study) was carried out with a 5-FU intra-arterial continuous infusion combined with systemic gemcitabine with an increase in dosage for both drugs [25]; this new routine, using two well-recognized antineoplastic drugs for pancreatic cancer, showed the advantage of reducing systemic toxicity of 5-FU, because the large extraction by the liver during the first passage, with high concentration into the tumor mass; moreover, using the Zanon- Grosso technique [26, 27], there is a continuous percutaneous access for delivering the drug. This treatment reduces drug toxicity and improves liver metastases control.
Combined Chemo-Irradiation Treatment
The present radiosensitizing drugs, 5-FU and for the most part gemcitabine, have allowed combined therapy with radiation (Phase I studies): Blackstock HW et al., Mc Ginn CJ et al. [28, 29]. These studies demonstrated that weekly or biweekly gemcitabine combined with radiotherapy is feasible with acceptable toxicity.
Van Riel JM et al. [30], in a phase II study, used the schedule GEM 300 mg/m2 and 800 cGY external beam radiation on days 1, 8, and 15 and when possible after 2 weeks rest GEM 1000 mg/m2 on days 1, 8, and 15 every 28 days until disease progression or unacceptable toxicity. The same therapeutic scheme, as a neoadjuvant treatment, demonstrated complications, related to the potent radiosensitizing properties of gemcitabine, such as upper gastrointestinal ulcers, fibrosis of the stomach and surrounding tissues and enteral fistulae after surgical therapy; new and lower GEM doses will be required in the neoadjuvant phase.
Other Palliative and Supportive Treatments
Patients with common bile duct blockage can benefit by endoscopic stent placement. Anorexia, weight loss and weakness as side effects of therapeutic agents and effects of the cancer on metabolism may, in part, be treated using a diet that includes high energy supplements. Some surgical procedures may considered for treatment of pain in addition to analgesic drugs: alcoholization of celiac ganglion, thoracoscopic splanchnicectomy.
Future Treatments
Immunotherapy. In active immunotherapy vaccines, produced by patient tumoral antigenes, allow amplification of the immune response and attack the neoplasm without causing normal tissue damage [1]. Studies with vaccines, carried out using tumorspecific K-ras peptide, are in progress. In passive immunotherapy antibodies made in the laboratory are injected to seek out pancreatic cancer cells which contain abnormal K-ras proteins, CEA or other neoplastic proteins. The same monoclonal antibodies with radioactive atoms in combination with gemcitabine, as a radiosensitizer, are aimed at the cancer cells [30].
Gene-therapy. Based on recombinant DNA technology many therapeutic approaches aim at stopping the oncogene (e.g. K-ras) or repairing a tumor suppressor gene (e.g. p53) using an adenovirus or retroviral vector [30, 31]. Non-viral systems, currently being studied, represent future vectors such as cationic lipids, polylysine, protamine, antibodies [32].
Angiogenesis and matrix metalloproteinase inhibitors. Solid tumors cannot grow larger than 1 mm without inducing the formation of new blood vessels to supply nutritional needs [33]. The new vessel development depends on the activation of proteins promoting endothelial cell growth and movement (angiogenin, epidermal growth factor, tumor necrosis factor-a, vascular endothelial and fibroblast growth factors, etc). Angiogenesis and metastasis require matrix metalloproteinases, enzymes that break down the surrounding tissue, the extracellular matrix, during blood vessel and tumor invasion. Blocking angiogenesis, with agents againts endothelial cells of the tumor, which have a low mutational rate, in contrast with high mutational rate tumor’s cells, reduces tumor acquired drug resistance [34].
Angiogenesis is regulated by natural inhibitors such as angiostatin, endostatin, interferons, interleukin 1a-b, metalloproteinases inhibitors, etc., but in tumors the vascular endothelial growth factor (VEGF) is upregulated by mutations of the Kras oncogene which occur in 75-90% of pancreatic adenocarcinoma. Monoclonal antibodies against VEGF and VEGF receptor blockers are undergoing clinical study [35]. Other anti-angiogenesis agents are: endostatin (produced by E. coli), interferon-alpha (fibroblast growth factor blocker) [34] and also thalidomide.
Matrix metalloproteinases are a family classified according to the substrate specificity of the hydrolyzing enzymes: collagenases, gelatinases, stromelysins for proteoglycans and glycoproteins and metalloelastases for elastin [36]. These agents do not affect cancer cells but delay tumor growth and reduce metastases. At the moment a phase II study of marimastat (BB-2516) demonstrates a significant decay in the rise of CA 19.9 [37] and a beneficial effect on survival as comapared with historical controls [36].
Conclusion
Therapeutic options in PC, even if less limited than in the past time, remain inefficacious for life-expectancy. A large number of chemotherapeutic agents have been tested in the advanced stage, but the mean tumor objective response is very small. Other therapeutic approaches, such as chemoradiotheraphy and intraoperative radiotherapy, have proven to be useless or of little value.
Palliative end points such as quality of life, performance status or disease-related symptom control should represent a priority in advanced PC, together with a careful evaluation of toxicity due to the side effects of the treatment used.
The results of previous published trials and of our study suggest that gemcitabine is the first cytotoxic agent with a positive impact on disease-related symptoms also having a low toxicity profile.
Further studies will focus on the evaluation of this drug in patients at an earlier stage of cancer and on combination regimes for patients in the advanced stage. In this phase, the radiosensitizing properties of gemcitabine appear to be promosing [28-29].
References
- Yeo CJ. Pancreatic cancer symposium. J Am CollSurg 1998; 187:429-42.
- Warshaw AL, Castillo CFD. Pancreatic adenenocarcinoma. New Engl J Med 1992; 326:455-65.
- Moossa AR, Gamagami RA. Diagnosis and staging of pancreatic neoplasms. SurgClin North Am 1995; 75:781-890.
- Lillemoe KD. Current management of pancreatic carcinoma. Ann Surg 1995; 221:133-48.
- Bramhall SR, AllumWH ,Jones AG, Allwood A, Cummins C, Neoptolemos JP. Incidence treatment and survival in 13560 patients with pancreatic cancer: an epidemiological study in the West Midlands. Br J Surg 1995; 82:111-5.
- Beger HG, Link KH, Poch B, Gansauge F. Pancreatic cancer recent progress in diagnosis and treatment. In: Neoptolemos JP, Lemoine NR, eds. Pancreatic Cancer: Molecular and Clinical Advances. Oxford: Blackwell Science Ltd, 1996: 227-35.
- Livingston EH, Welton MI, Reber HA. Surgical treatment of pancreatic cancer. The United States experience. Int J Pancreatol1991; 9:153-7.
- Taylor I. Should further studies of chemotherapy be carried out in pancreatic cancer? Eur J Cancer 1993; 29:1076-8.
- Moore M. Activity of gemcitabine in patients with pancreatic adenocarcinoma. Cancer 1996; 78 (Suppl. 1): 633-6.
- Ahlgren JD. Chemotherapy for pancreatic adenocarcinoma. Cancer 1996; 78:655-63.
- Mallinson CN, Rake MO, Cocking JB, Fox CA, Cwynarski MT, Diffey BL, et al. Chemotherapy in pancreatic cancer: results of a controlled, prospective, randomised, multicentre trial. Br Med J 1980; 281:1589- 91. [81087611]
- Arbuck SG. Chemotherapy for pancreatic cancer. BallieresClinGastroenterol 1990; 4:953-68.
- Bkkevold KE. Chemotherapy of unresectable pancreatic cancer. In: Beger HG, Warshaw AL, Russell RCG, Bucher M, Carr- Locke D, Neoptolemos JP, Sarr MG, eds. The Pancreas. Oxford: Blackwell Science Ltd, 1998: 1120-38.
- Rothenberg ML, Abbruzese JL, Moore MJ, Portenoy RK, Robertson JM, Wanebo HG. A rationale for expanding the endpoints for clinical trials in advanced pancreatic carcinoma. Cancer 1996; 78:627-32.
- Casper ES, Green MR, Kelsen DP, Heelan RT, Brown TD, Flombaum CD, et al. Phase II trial of gemcitabine (2’,2’- difluorodeoxycytidine) in patients with adenocarcinoma of the pancreas. Invest New Drugs 1994; 12:29 34. [95049289]
- Carmichael J, Fink U, Russell RC, Spittle MF, Harris AL, Spiessi G, Blatter J. Phase II study of gemcitabine in patients with advanced pancreatic cancer. Br J Cancer 1996; 73:101-5. [96146609]
- Rothenberg ML, Moore MJ, Cripps MC, Andersen JS, Portenoy RK, Burris HA 3rd, et al. A phase II trial of gemcitabine in patients with 5-FU-refractory pancreas cancer. Ann Oncol 1996; 7:347-53. [96399432]
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J ClinOncol 1997; 15:2403- 13. [97339557]
- Anderson H, Lund B, Bach F, Thatcher N, Walling J, Hansen HH. Single-agent activity of weekly gemcitabine in advanced nonsmall- cell lung cancer: a phase II study. J ClinOncol 1994; 12:1821-6. [94365627]
- Lund B, Hansen OP, Theilade K, Hansen M, Neijt JP. Phase II study of gemcitabine (2',2'-difluorodeoxycytidine) in previously treated ovarian cancer patients. J Natl Cancer Inst 1994; 86:1530-3. [95018323]
- Huang P, Chubb S, Hertel LW, Grindey GB, Plunkett W. Action of 2',2'- difluorodeoxycytidine on DNA synthesis. Cancer Res 1991; 51:6110-7. [92034728]
- Ghandi V, Plunkett W. Modulatory activity of 2’-2’deoxycytidine on the phosphorilation and cytotoxicity of arabinosyl nucleotides. Cancer Res 1990; 50:3675-80.
- Hermanek P, Sobin LH, eds. UICC TNM classification of malignant tumours. 4th ed. Berlin: Springer-Verlag, 1987.
- Theodors A, Bukowski RM, Hewlett JS, Livingston RB, Weick JK. Intermittent regional infusion of chemotherapy for pancreatic adenocarcinoma. Phase I and II pilot study. Am J ClinOncol 1982; 5:555-8. [83097425]
- Zanon C, Alabiso O, Grosso M, Buosi R, Chiappino I, Clara R, et al. Intra-arterial continuous infusion for treatment of pancreatic and biliary tract cancer. Int J Pancreatol 2000; 27:225-33. [20406937]
- Zanon C, Grosso M, Zanon E, Veltri A, Alabiso O, Bazzan M, et al. Transaxillary access to perform hepatic artery infusion (HAI) for secondary or primitive hepatic tumors. Minerva Chir 1996; 51:755-8. [97122662]
- Grosso M, Zanon C, Zanon E, Corsico M, Gazzera C, Mancini A, Fava C. The percutaneous placement of intra-arterial catheters with "reservoirs" for subcutaneous infusion. The technic and preliminary results. Radiol Med 1997; 94:226-32. [98090006]
- Blackstock AW, Bernard SA, Richards F, Eagle KS, Case LD, Poole ME, et al. Phase I trial of twice-weekly gemcitabine and concurrent radiation in patients with advanced pancreatic cancer. J ClinOncol 1999; 17:2208-12. [20030006]
- McGinn CJ, Smith DC, Szarka CE. A phase I study of gemcitabine in combination with radiation therapy in patients with localized unresectable pancreatic cancer. Proc Am SocOncol 1998:264a.
- Van Riel JM, Giaccone G, Pinedo HM. Pancreaticobiliary cancer: the future aspects of medical oncology. Ann Oncol 1999; 10 (Suppl. 4):296-9. [99365897]
- Carter G, Gilbert C, Lemoine NR. Effect of antisense oligonucleotides targeting K-ras expression in pancreatic cancer cell lines. Int J Oncol 1995; 6:1105-12.
- Searle PF, Green NK, Young L. Genetranfer therapy and pancreatic Cancer. In: Neoptolemos JP, Lemoine NR, eds. Pancreatic Cancer. Molecular and Clinical Advances. Blackwell Science 1998.
- Folkman J. What is the evidence that tumors are angiogenesis dependent?. J Natl Cancer Inst 1990; 82:4-6.
- Boehm T, Folkman J, Browder T, O’Relly MS. Antiangiogenic therapy of sperimental cancer does not induce acquired drug resistance. Nature 1997; 390:404-7.
- Nelson NJ. Inhibitors of angiogenesis enter phase III testing. J Natl Cancer Inst 1998; 90:960-3.
- Bramhall SR. The matrix metalloproteinases and their inhibitorsin pancreatic cancer. Int J Pancreatol 1997; 21:1- 12.
- Rosemurgy A, Harris J, Langleben A. Marimastat a novel metalloproteinase inhibitor in patients with advanced carcinoma of the pancreas. Proc Am SocClinOncol 1996: A207.

