Riccardo Casadei1, Raffaele Pezzilli2, Lucia Calculli3, Donatella Santini4, Giovanni Taffurelli1, Claudio Ricci1, Marielda D’Ambra1, Francesco Minni1
Departments of 1Surgery, 2Internal Medicine, 3Radiology, and 4Pathology,
“S.Orsola-Malpighi” Hospital, Alma Mater Studiorum, University of Bologna. Bologna, Italy
- *Corresponding Author:
- Riccardo Casadei
Department of Surgery; S.Orsola-Malpighi Hospital; Alma Mater
Studiorum - University of Bologna; Via Massarenti n. 9; 40138
Bologna; Italy
Phone: +39-051.341.541
Fax: +39-051.341.483
E-mail: riccardo.casadei@aosp.bo.it
Received July 30th, 2012 – Accepted September 24th 2012
Keywords
Cystadenoma, Mucinous; Male; Neoplasms; Pancreas; Pancreatectomy
INTRODUCTION
Pancreatic cystic neoplasms represent about the 1% of all pancreatic tumors [1]. Among pancreatic cystic tumors, the WHO classification [2] recognized mucinous cystic neoplasm (MCN) as a tumor of the premenopausal female patients, characterized by the presence of an ovarian-type stroma in the pathological examination of the specimen. Herein, we describe a very rare case of a MCN in a male patient with the aim to understand how is possible the presence of this tumor in a male patient.
CASE REPORT
A 65-year-old man was seen as outpatient at our Pancreas Unit in March 2012. He was a drinker of 50 grams of pure alcohol per day from 25 to 65 years of age and heavy smoker (40 cigarettes per day from the 18th to 50th years of age. At the age of 50 years a diagnosis of diabetes mellitus type 2 was made and the patient assumed metformin at a dosage of 2,000 mg per day and glicazide at the dosage of 60 mg per day. He never experienced abdominal pain and the reason why he was admitted to our unit was the ultrasonographic detection of a cyst located in the body-tail of the pancreas of 3.8 cm of diameter one year before. On admission, clinical examination revealed no major abnormalities and his body mass index was 30 kg/m2.
Laboratory investigations were unremarkable, a part the finding of a poor glycemic control (glucose 189 g/dL, reference range: 70-110 g/dL; concentrations of hemoglobin A1c (HbA1c) of 75 mmol/mol, reference range: 20-42 mmol/mol). The tumor markers (CEA, CA 19-9) were normal. Abdominal contrast-enhanced computed tomography was carried out and showed an increase of the unilocular pancreatic cyst from 38 mm, seen one year before at US, to 49 mm in diameter. To better evaluate the presence of a link between the cyst and the pancreatic tree, a magnetic resonance cholangiopancreatography (MRCP) was carried-out. This examination showed a well-shaped pancreatic gland with a 49 mm diameter fluid mass localized in the body, without septa or endoluminal solid components, without a clear communication with the main pancreatic duct (Figure 1). The lesion did not seem to infiltrate the peripancreatic vessels, but, for its size, it seemed to slightly constrict the splenic artery and vein. Finally, contrast enhanced ultrasonography confirmed the strict connection with the splenic vessels, without their infiltration, and revealed the absence of contrast-enhancement in the cyst’s content and wall, as well as the presence of communication with the main pancreatic duct. Because the increase of the cyst, the patient underwent a distal pancreatectomy with spleen resection and standard lymphadenectomy. Macroscopically, the examination of the specimen showed a cystic lesion measuring 40 mm of maximum diameter. The cut surface demonstrated a unilocular cystic pattern with smooth and white inner walls, containing viscous whitish mucin. The cyst showed a peripheral pattern of growth, without communication with the pancreatic ductal system. The remaining parenchyma was normal and the transection margin was 20 mm far from the mass. Microscopically, the cystic lesion showed two distinct components: a mucinous epithelial layer showing low-grade dysplasia and an ovarian-type stroma (according to WHO 2010 [3]). Immunohistochemically, the stromal layer was positive for estrogen, progesterone and calretinin receptors (Figure 2). According to these findings, the cystic lesion was diagnosed as a MCN having ovarian stroma of the pancreas; lymph nodes (n=6) were negative.
Figure 1. Magnetic resonance cholangiopancreatography (MRCP)
showed a 49 mm fluid mass in the body-tail of the pancreas without
septa or mural nodules and without communication with the Wirsung
duct.
Figure 2. a. Microscopically (hematoxylin-eosin x100), an ovarian
type stroma layer, that appears as a band of densely packed spindle
cells, is covered by a mucinous epithelial low grade dysplasia layer. b. Immunohistochemical analysis (x100) of the ovarian type stroma,
showed expression of receptors for estrogen.
The postoperative course was complicated by a pancreatic fistula, grade B, treated with a CT-guided abdominal drainage in post-operative day 7. A contrast enhanced CT scan, performed in postoperative day 12, showed a reduction of the abdominal collection and the patient was discharged in postoperative day 14 with a minimal residual drainage output.
DISCUSSION
In 1996 the WHO classification defined mucinous cystic neoplasms as cystic epithelial neoplasms composed of columnar, mucin-producing epithelium, supported by ovarian-type stroma, usually in premenopausal female patients. The ovarian-type stroma appears as a band of densely packed spindle cells beneath the epithelium; its presence has become a critical requirement to make diagnosis of MCNs [2].
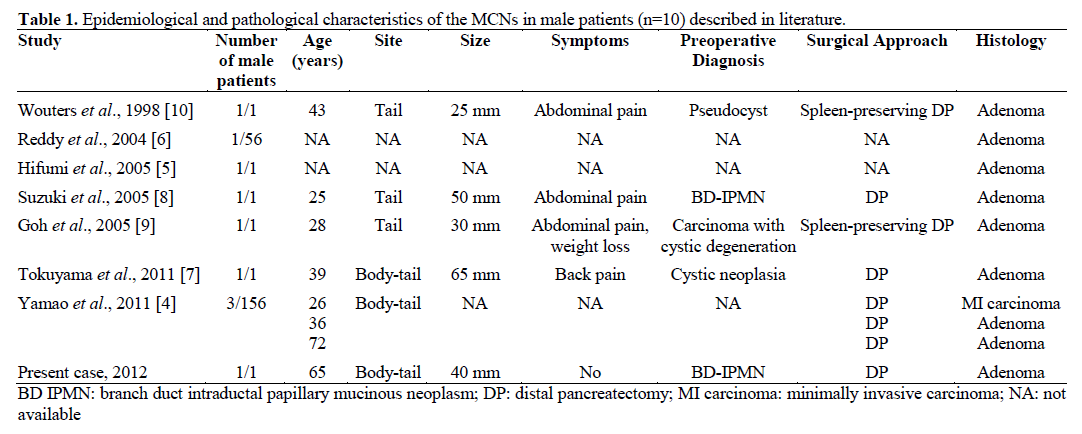
The distinctive aspect of our case was that the ovariantype stroma was found in a male patient. Nine cases only regarding male patients with WHO criteria for diagnosis of MCN have been reported in literature and our case represents the 10th. Among the 9 cases described in literature, 3 cases were demonstrated in a recent multi-institutional study for MCNs with ovariantype stroma by the Japan Pancreas Society, collecting a total of 156 cases of MCNs [4]; one case was described in a Japanese male in 2005 [5]; another case was counted by Reddy et al. [6] in a 56 cases record of MCN in 2004. Only 4 cases were fully described: a 39- year-old man in 2011 [7], a 25-year-old man and a 28- year-old man in 2005 [8, 9], and a 43-year-old man in 1998 [10] (Table 1). Unlike female cases, in which the tumor develops in pre-menopausal age, in male patients the age of diagnosis is highly variable ranging from 25 to 72 years of age (mean age 41.7 years). The majority of patients was symptomatic (4/5; 80%); the tumor was usually benign, located in the tail and with a mean diameter of 42 mm, as in our case. In all cases, the preoperative diagnosis was different from MCN and all patients were treated surgically.
The question why a MCN with ovarian-type stroma affects a male patient is not clear. Currently, there are two hypothesis concerning the origin of ovarian-type stroma in MCNs in male: 1) ovarian stroma arises from rests of embryologic ovarian tissue deposited in the pancreas and this hypothesis is supported by the close proximity of the left ovarian primordium to the bodytail of the dorsal pancreas in fetal life; 2) ovarian stroma represents a recapitulation of periductal fetal mesenchymal connective tissue, the primitive mesenchymal tissue seen around the pancreatic and hepatic ducts in the developing fetus [1, 11]. Furthermore, regardless of its origin, it is also clear that this stroma is hormone sensitive: in fact, it is often admixed with luteal-type cells and it regularly expresses estrogen and progesterone receptors [1, 11]. This finding, together with the first pathogenetic hypothesis, could explain the higher incidence of MCN in peri-menopausal female patients, which are stimulated by progesterone and estrogen during their life.
On the contrary, the second hypothesis seems to be the only one that could explain a MCN’s onset in male patients. According to this, the pathogenesis would start with a process of hormonal reactivation of cells from the periductal fetal mesenchyme, that leads to the proliferation of an ovarian-type stroma and a secondary activation of the ductal epithelium. However, in our opinion, this hypothesis is not able to explain the coexistence of luteal-type cells, typically alpha-inhibin and calretinin immunohistochemically positive, and described resembling luiteinized stroma of the ovary. Nevertheless, these luteinized cells are very similar, morphologically and immunohistochemically, to Leydig cells. Thus, also in a man this tumor may arise from a residual embryonic undifferentiated sexual cord ridge.
In conclusion, the MCN may rarely regard male patients, probably for embryological abnormalities.
Conflicts of interests
The authors have no potential conflict of interest
References
- Adsay VN. Cystic lesions of the pancreas. Mod Pathol 2007; 20:S71-93.
- Bosman, FT, Carneiro F, Hruban RH, Theise ND. In: WHO Classification of Tumours. IARC WHO Classification of Tumours, No 3, 2010.
- Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Falconi M, Shimizu M, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasm and mucinous cystic neoplasms of the pancreas. Pancreatology 2006; 6:17-32.
- Yamao K, Yanagisawa A, Takahashi K, Kimura W, Doi R, Fukushima N, et al. Clinicopathological features and prognosis of mucinous cystic neoplasm with ovarian-type stroma. A multiinstitutional study of the Japan pancreas society. Pancreas 2011; 40:67-71.
- Hifumi M, Fukuda S, Yamane T, Yokomizo H, Kitada H, Kawaguchi T, et al. A case of the pancreatic mucinous cystadenoma in a man with ovarian-type stroma, expressing estrogen and progesteron receptors. Nihon ShokakibyoGakkaiZasshi 2005; 102:1188-93.
- Reddy RP, Smyrk TC, Zapiach M, Levy MJ, Pearson RK, Clain JE, et al. Pancreatic mucinous cystic neoplasm defined by ovarian stroma: demographics, clinical features, and prevalence of cancer. ClinGastroenterolHepatol 2004; 2:1026-31.
- Tokuyama Y, Osada S, Sanada Y, Takahashi T, Yamaguchi K, Yoshida K. Mucinous cystic neoplasm of the pancreas in a male patient. Rare Tumors 2011; 3:e14.
- Suzuki M, Fujita N, Onodera H, Kayaba Y, Suzuki S, Kagaya H, et al. Mucinous cystic neoplasm in a young male patient. J Gastroenterol 2005; 40:1070-4.
- Goh BK, Tan YM, Kumarasinghe MP, Ooi LL. Mucinous cystic tumor of the pancreas with ovarian-like stroma in a male patient. Dig Dis Sci 2005; 50:2170-7.
- Wouters K, Ectors N, Van Steenbergen W, Aerts R, Driessen A, Van Hoe L, Geboes K. A pancreatic mucinous cystadenoma in a man with mesenchymalstroma, expressing oestrogen and progesterone receptors. Virchows Arch 1998; 432:187-9.
- Basturk O, Coban I, Adsay NV. Pancreatic cysts: pathologic classification, differential diagnosis and clinical implications. Arch Pathol Lab Med 2009; 133:423-38.



